
Jason Fink, BS1; Bradley A. Fink, DO2
1Second year medical student, Philadelphia College of Osteopathic Medicine,
2Orthopedic Surgeon, TrinityHealth Mid-Atlantic Nazareth Hospital
DOI: 10.70709/AK5798-QW
Abstract
The authors present a case involving a closed complex distal metadiaphyseal femoral fracture that lacked inherent stability to allow conventional provisional stabilization prior to definitive fixation. Comminution, traumatic soft tissue stripping and poor bone quality due to osteopenia or intramedullary bone loss may make provisional stabilization of complex fractures difficult. An intact periosteal and myofascial envelope provides inter-fragmentary stability as well as blood supply for bone union. An intramedullary plate was successfully used primarily to maintain provisional reduction but was retained as a part of the definitive construct. This technique should be familiar to any surgeon that operatively manages complex fractures in which conventional techniques for provisional stabilization fail or are not optional.
Keywords: Intramedullary, metadiaphyseal, provisional, stabilization, reduction, unicortical
Introduction
Standard techniques for provisional stabilization include reduction clamps, combination plate and reduction clamps (reduction plating), Kirchner wires, cerclage wires, cables, and inter-fragmentary lag screws. When these conventional techniques fail to maintain provisional reduction of a complex, unstable fracture or are not optional due to the fracture pattern, comminution, poor bone quality or traumatic soft tissue disruption, intramedullary plate osteosynthesis should be considered. Fracture instability can lead to the loss of reduction during the application of fixation implants.(1) This occurs when there is a lack of bony architecture necessary for conventional reconstruction.(2) This is also seen when the local soft tissue envelope is disrupted and unable to provide interfragmentary stability. Intramedullary plating is a useful option for fractures that are irreducible by standard direct and indirect reduction techniques, especially when metaphyseal comminution is present.(3) An intramedullary plate acts as a reduction tool when direct and indirect manipulation techniques such as Schanz pin joysticks, external fixators and traction prove difficult.(4) Awareness of this technique may improve fracture reduction maintenance.
Case Report
A 92-year-old female non-ambulator with Alzheimer’s dementia and diabetes mellitus presented to the emergency room with left thigh and knee pain, swelling and deformity after an unwitnessed fall from bed at the nursing home where she resides. Imaging of the left femur and knee demonstrated a displaced distal third metadiaphyseal femoral fracture with a butterfly fragment, supracondylar extension and osteopenia.

The following day, the patient was taken to the operating room. General anesthesia was administered and indirect reduction by traction and closed manipulation revealed that the fracture was grossly unstable and irreducible. Comminution with butterfly fragmentation precluded the use of percutaneous reduction techniques such as joysticking. Through a lateral approach, direct reduction was performed however provisional stabilization using reduction clamps and a K-wire failed. The butterfly fragment consisted of an anterior, lateral, and posterior shell without a soft tissue hinge necessary for inter-fragmentary stability, contributing to the loss of reduction. Additionally, the femur was a hollow cortical tube, void of intramedullary cancellous bone stock. This deficiency contributed to the loss of cortical reduction as there was no intramedullary counterforce to support and buttress the butterfly fragment. As a result, the butterfly fragment countersunk within the intramedullary canal, leading to malreduction, during the application of a reduction clamp and K-wire. A cerclage wire and cable would similarly fail. Moreover, the comminution precluded the opportunity for fracture interdigitation, adding to further inherent instability. The main proximal and distal fragments could not be held reduced with a clamp or K-wire because their bony approximation consisted of a short oblique medial cortical wall. Since maintaining reduction by standard techniques failed or were contraindicated, intramedullary plate stabilization was necessary to provisionally repair the two main medial cortices. Prior to this, a 3.5 mm cortical lag screw (Synthes, Paoli, PA) was used to stabilize a vertically split distal fragment. The distal fragment was then provisionally fixed to the proximal fragment, medially, through the butterfly defect using a 6 hole 3.5mm 1/3 tubular unicortical plate (Synthes, Paoli, PA) placed perpendicular to the main fracture line (Fig. 2-3).
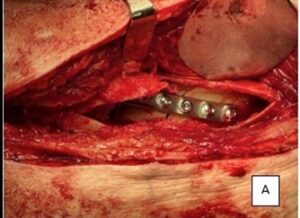 Fig. 2 Intraoperative intramedullary plating |
 Fig. 3 Intraoperative AP, Lat left femur after intramedullary plating and lag screw insertion |
Cancellous allograft and demineralized bone matrix (Synthes, Paoli, PA) were placed intramedullary at the fracture site, filling the bony void (Fig 4).

Fig. 4 Intra-operative composite allografting
The butterfly fragment was reduced and supported by the allograft composite on which it lays (Fig. 5-6).
 Fig. 5 Intra-operative butterfly fragment reduction |
 Fig. 6 Intraoperative AP after allografting and butterfly fragment reduction |
Finally, a periarticular locking distal femoral plate (Synthes, Paoli, PA), incorporating a 3.5mm interfragmentary lag screw, was placed over the butterfly fragment and spanned the fracture for definitive fixation (Fig. 7).

Patient was uneventfully discharged to a skilled nursing facility on postoperative day four. Two weeks after surgery, she was seen in the clinic. There was no edema, extremity deformity, ecchymosis or signs of infection. The wound was healed and her surgical clips were removed. She was maintained on non-weightbearing. At three months postoperative, there were clinical and radiographic signs of successful fracture healing. She was upgraded to full weight-bearing and discharged.
Discussion
Open reduction of unstable fractures are typically maintained with a reduction clamp, combination plate and reduction clamp or Kirchner wire before provisional stabilization is accomplished with a cerclage wire, cable, interfragmentary lag screw or plate. When reduction is not easily maintained and provisionally stabilized in challenging fractures with comminution, traumatic soft tissue stripping or bone deficiency or when reduction clamps hinder definitive plate placement, provisional reduction plating is needed.(5-8) Circumferential metaphyseal comminution makes lag screw application difficult.(5) When standard options prove inadequate or fail to maintain reduction, intramedullary unicortical plating should be considered. A butterfly fragment that prevents visualization and reduction of the main fragments is an indicator for intraosseous plating.(3) Intraosseous plating requires intramedullary access through a cortical bone window produced by a large butterfly defect or bone loss.(4) Retracting or removing the butterfly fragment permits visualization, reduction and application of an endosteal plate. This technique avoids periosteal stripping of the opposite (medial) cortex required for standard extramedullary “sandwich” plating. Intramedullary plating decreases the risk of nonunion and neurovascular injury incurred from exposure around the opposite cortex.(3,4) Since our patient had the nonunion risk factors of diabetes mellitus and older age with intramedullary bone loss, endosteal plating allowed us to avoid the need for further soft tissue stripping on the periosteal surface. A 3–6 hole 2.0, 2.4, 2.7 or 3.5 mm 1/3 tubular unicortical provisional metadiaphyseal or periarticular plate using 1-3 screws on either side of the fracture has been recommended.(3,5) This implant is low profile and easily contours to the bony architecture avoiding further fracture displacement.(5) The large canal of the metadiaphyseal region easily accommodates the larger length and diameter plate. The medial endosteal plate is used for provisional support and fixation, not as a plate reduction technique.(1,4) The plate is not used to reduce the fracture but is instead used to stabilize the fracture after manual reduction. The medial intramedullary plate maintains medial bone length, allowing lateral butterfly fixation with a 3.5 cortical lag screw.(4) The intramedullary plate should be applied in compression if the fracture permits.(4) The plate provides a provisional intramedullary buttress prior to grafting.(2) This technique may be used for fractures with or without medial bone loss. Composite fixation with intramedullary and extramedullary plating is indicated when there is a lack of medial cortical buttress due to comminution, severe osteoporosis or in pathologic fractures.(1)
The bone graft used in this case enhances the biologic properties for healing while providing a bed to support the butterfly fragment and prevent its settling, similar in concept to grafting tibial plateau fractures. The use of a unicortical intramedullary medial plate did not preclude the concomitant use of a retrograde nail instead of the lateral plate for definitive fixation. A plate was chosen for definitive fixation because it could be placed through the existing incision, avoiding a secondary incision and arthrotomy necessary for nail placement which would add to the risk of postoperative joint sepsis, joint adhesions, joint stiffness and nail interference of the intramedullary grafting. A theoretical alternative to intramedullary plate fixation and composite allografting would be screw fixation of an intramedullary fibular strut allograft. This construct would function as a provisional stabilizer while providing the osteoconductive biology to promote bone union, similar to its use in humeral shaft nonunion revision surgery.
A potential complication to intramedullary plating is intramedullary infection and osteomyelitis, which is a concern no different from intramedullary nailing. This has not been experienced in the literature and this technique has a low complication rate.(3) Retention of a provisional plate has no impact on union.(7) Intramedullary plating is a noteworthy technique to be aware of as it brings value to surgeons who perform fracture repair when simpler, routine methods of provisional stabilization are contraindicated or fail as is seen in this case.
Conclusion
Our patient presented with a complex fracture pattern that lacked the intact soft tissue hinges and sufficient endosteal cancellous bone stock necessary for effective provisional stabilization by standard means. Through a window of opportunity provided by a large butterfly fragment, an intramedullary 3.5mm 1/3 tubular plate was utilized to allow anatomic provisional fracture stabilization and permit successful bone grafting and definitive reconstruction.
References
- Mast J, Jakob R, Ganz R. Planning and Reduction Technique and Fracture Surgery, Berlin Heidelberg: Springer-Verlag; 1989: 201-227.
- Russell GV, Pearsall AW. Intramedullary plate Fixation of a Distal Humerus Fracture: A Case Report. Journal of Orthopedic Trauma. 2002; 16:353–361.
- Archdeacon MT, Wyrick JD. Reduction Plating for Provisional Fracture Fixation. Journal of Orthopedic Trauma. 2006; 20:206–211.
- Dolch Hj, Chase RD. Intramedullary Minifragmentary Plate Fixation: A Helpful Reduction Tool. American Osteopathic Academy of Orthopedics. 2023.
- Jong-Keon O, Dipit S, Jong-Woong P, Chang-Wug O, Jin–Ho H. Use of 2.0 Mini Plate System as Reduction Plate. Archives of Orthopedic and Traumatic Surgery. 2010; 130: 1239-1242.
- Hreha J, Ulitto JM, Reilly M, Sirkin M, Adams M. Provisional Reduction Plating in the Treatment of Ankle Fractures: A Technical Trick. European Journal of Orthopedic Surgery and Traumatology. 2022; 32:1215–1217.
- Bishop JA, Castillo TN. Provisional Mini-Fragment Plate Fixation in Clavicle Shaft Fractures. The American Journal of Orthopedics. 2013; 470-472.
- Dunbar RP, Nork SE, Barei DP, Mills WJ. Provisional Plating of Type III Open Tibia Fractures Prior to Intramedullary Nailing. Journal of Orthopedic Trauma. 2005; 19:415–417.
- Ganz R, Isler B, Mast J. Internal Fixation Technique and Pathological Fractures of the Extremities. Archives of Orthopedic and Traumatic Surgery. 1984; 103:73–80
