
1Kettering Health Grandview Orthopedic Surgery, Dayton, OH
Abstract
Background
Greater trochanteric pain syndrome (GTPS) affects up to 25% of people and was once thought to be caused mainly by trochanteric bursitis. However, newer studies suggest that gluteus medius and minimus tendinopathy or tears are often the main issue in patients with these symptoms, especially in patients who have had hip replacements. This study was designed to characterize the presenting symptoms of patients with a glute medius or minimus tears, and report on the outcomes of their surgical repair.
Methods
We reviewed 10 patients who had endoscopic repairs of the gluteus medius with previous hip replacements. We compared preoperative and postoperative Modified Harris Hip Scores (MHHS) to measure functional improvement. Diagnoses were confirmed through physical exams, using the a 30-second Trendelenburg test, single-leg squat, and single-leg bridge test, along with ultrasound imaging performed by musculoskeletal-trained radiologists.
Results
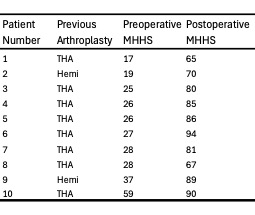
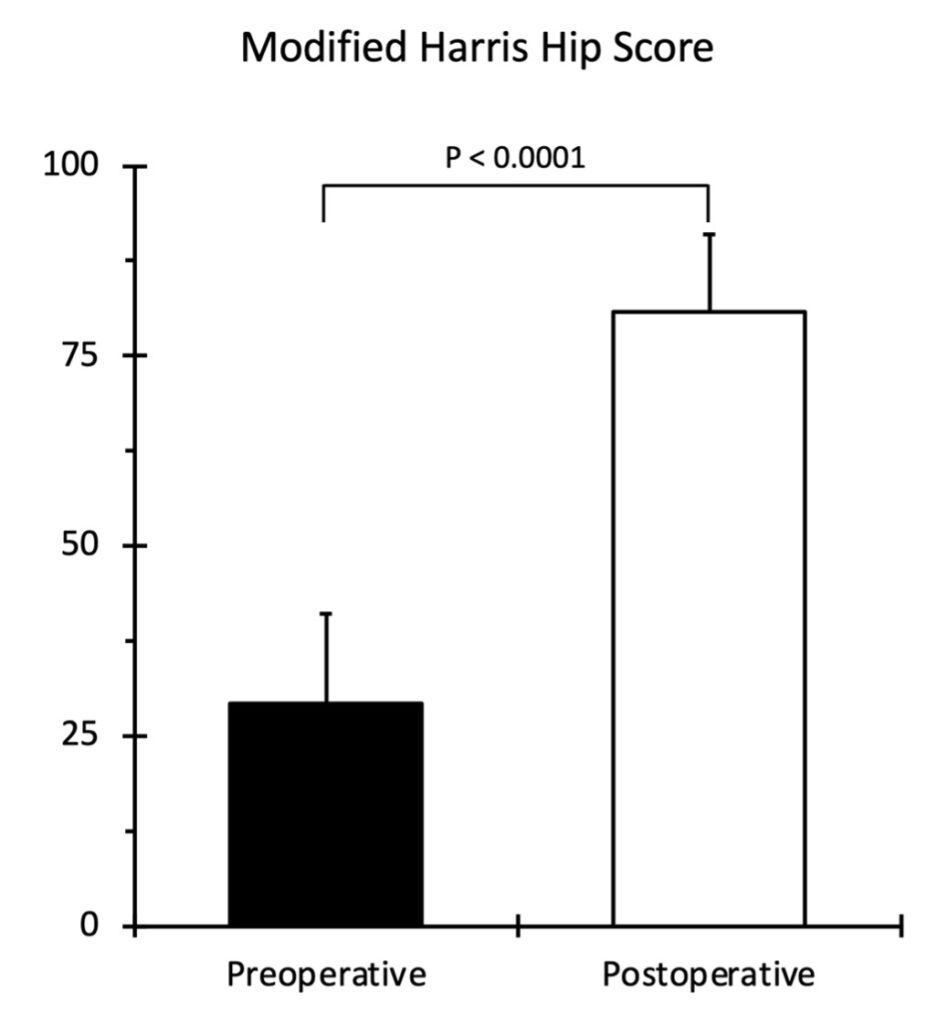
All patients had lateral hip pain and weakness. After surgery, MHHS scores significantly improved from an average of 29 to 81. All patients reported pain relief, and follow-up ultrasounds showed good tendon healing.
Conclusion
This study supports endoscopic repair as an effective, minimally invasive option for gluteus medius tears in patients with hip replacements. Our results indicate possible benefits over open surgery, such as less pain and quicker recovery. More studies are needed to confirm long-term outcomes and the advantages of double-row fixation.
Keywords: Greater Trochanteric Pain Syndrome, Gluteus Medius, Tears, Endoscopic, Repair, Arthroplasty
Introduction
Greater trochanteric pain syndrome (GTPS) is a common complaint seen in 10-25% of the population (10). Previously, it had been thought that the vast majority of these cases were due to trochanteric bursitis; however, it has been increasingly noted that tendinopathy of the gluteus medius and minimus tendons is the primary pathology in GTPS (7). Imaging studies have reported that trochanteric bursitis is present in only a minority of patients with GTPS(8,11). These results have implications on the treatment of GTPS. Bursitis is usually treated with corticosteroid injections, while surgical repair is recommended for gluteus medius tears that fail conservative measures (3).
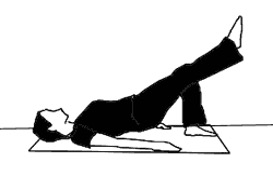
Gluteus medius tears are seen in four settings: 1) trauma, 2) degenerative disease, 3) femoral neck fractures, and 4) following hip arthroplasty surgery. Incidental gluteal tears have been noted during exposure for patients undergoing hip arthroplasty for osteoarthritis or fractures (1,2). Despite normal x-rays, some patients that have previously undergone hip arthroplasty continue to have lateral hip pain and weakness. To help with diagnosising these patient, we describe a gluteal triad of physical exam findings: 1) 30-second Trendelenberg test, 2) single stance squat test, and 3) unilateral bridge test (Fig. 1) (9). Due to difficulties examining the gluteal tendon with conventional MRI secondary to metal artifact, we also examined the presence of the tear through ultrasound preoperatively.
Repair of gluteus medius tears have been reported in the literature in patients with both native hips and hip arthroplasty. The treatment of gluteus medius tears using an endoscopic technique has been previously described in patients with native hips (4). However, only open surgical techniques have been described in patients with hip arthroplasty (3). To our knowledge, this is the first report of endoscopic repair for gluteal tendon tears in patients with hip arthroplasty. The goal of this paper is to examine the clinical outcomes of patients with previous hip arthroplasty undergoing endoscopic repair of their gluteal tendons, and provide a detailed technical guide for surgeons who are interested in adopting the technique.
Material and Methods
This study was reviewed and approved by our institutional review board. We retrospectively reviewed consecutive cases of endoscopic gluteal tendon repair over a 2-year period that were performed by a single surgeon. Candidates for surgery were patients who had a satisfactory appearance of hip arthroplasty on radiographic imaging, with no apparent loosening, malalignment, or subsidence of the prosthesis. Patients who complained of persistent lateral hip pain and associated weakness despite conservative management. All of the patients underwent MRI and dynamic ultrasound imaging performed and interpreted by musculoskeletal-trained radiologists to examine the presence and extent of the tear. Surgical history and interoperative notes were reviewed to assess for a history of hip arthroplasty. Perioperative parameters were examined. Patients were followed for a minimum of 1 year, and outcomes were gaged by modified Harris hip scores (MHHS) compared to preoperative values. The postoperative course was recorded, including complications and reoperations. Patients underwent ultrasounds at follow-up appointments to assess the healing status of the tendon. All of the statistics were performed using IBM SPSS Statistics software (version 29.0.2.0 (20)). Categorical variables were analyzed using Fisher’s exact test and the Chi-squared test. Continuous variables were compared with an independent samples t-test. A p-value of 0.05 was set to determine statistical significance for all analyses.
Detailed Surgical Technique Description
After failing conservative measures with corticosteroid injections, anti-inflammatories, and physical therapy, these recalcitrant cases of greater trochanteric pain syndrome underwent endoscopic gluteus medius repair by a single surgeon. Using a knotless, double row, suture bridge technique to repair the gluteus medius tear to the anatomic footprint of the tendon.
Under general anesthesia, the patient is placed in the lateral decubitus position on a bean bag with a pillow/bump between the legs to relieve tension on the iliotibial band and gluteus medius tendon. This positioning allows the surgeon to perform this procedure without the need for imaging, traction, or central compartment hip arthroscopy. Gravity irrigation with epinephrine and a 30° arthroscopic camera are used for the procedure. Antero-inferior and postero-inferior portals are created 2 cm distal to the tip of the greater trochanter and along the anterior and posterior borders of the proximal femur, respectively. Using the arthroscopic blunt trochar in the posterior portal and a colored plastic blunt trochar in the anterior portal, dissect down to the iliotibial band, triangulating the trocars aiming toward the bare spot of the trochanter. We recommend placing the arthroscopic camera in the posterior portal and visualizing the colored blunt trochar while establishing inflow through the scope and outflow through the colored trochar. A thermal wand is then used in the anterior portal to incise through the iliotibial band, targeting the trochanteric bare spot. The trochanteric bursa is carefully excised using the thermal wand in its entirety to reveal the greater trochanter and the tendons of the gluteus medius, gluteus minimus, gluteus maximus, and vastus lateralis.
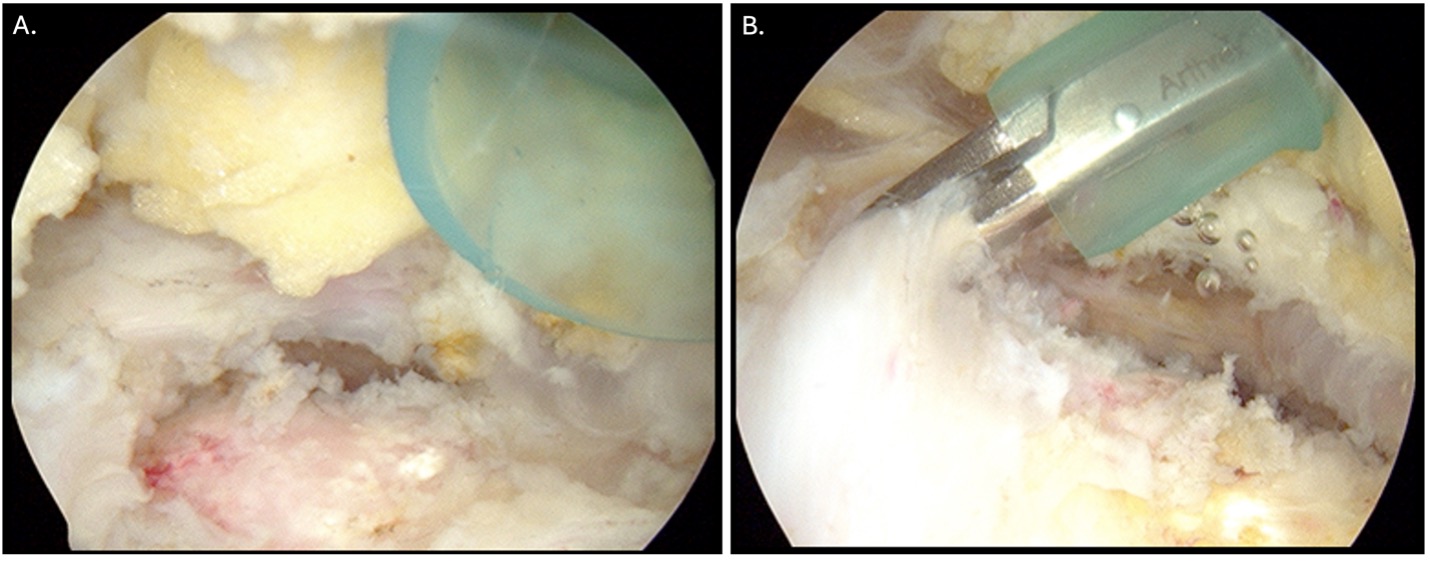
The fan-shaped gluteus medius is identified, assessing for size and mobility of any tears using a grasper (Fig. 2). The subgluteal space is entered, and the gluteus minimus insertion to the anterior facet is then assessed. Mobilization of the gluteal tendon tear with a grasper is assessed. A bleeding bone bed is created at the tendon footprint using a motorized burr. A spinal needle is placed superior to the midline of the tip of the trochanter to place planned anchors at a 45-degree deadman angle. The broad 35mm lateral facet allows 1.5 cm spacing between the two proximal row anchor holes. [Load a solid-colored 2 mm suture tape into the first 5.5 mm anchor to use as the first proximal row anchor. A second striped suture tape may be loaded into a separate anchor for later placement]. Prepare proximal row holes using a punch through the third, superior midline portal created around the spinal needle.
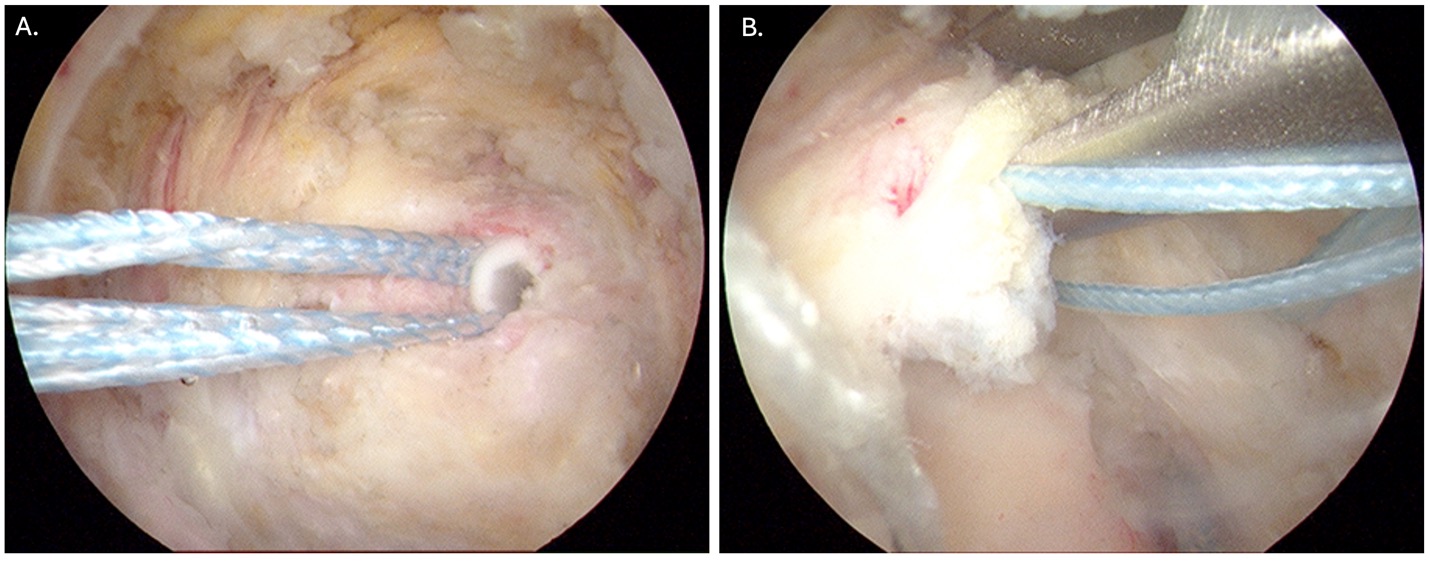
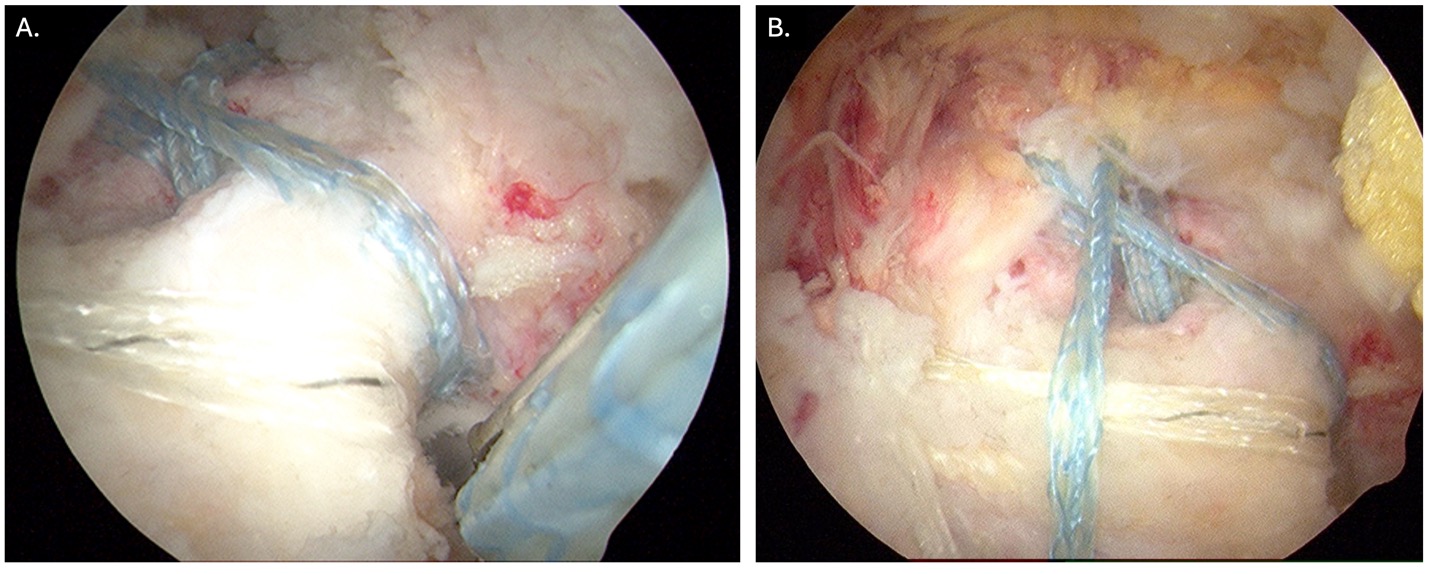
Insert the first loaded anchor into the first prepared proximal bone hole (Fig. 3A). Retrieve one limb of suture tape through the colored cannula in the Antero-inferior portal and load in a suture passer (Fig. 3B). Pass the suture through the posterior edge of the tendon tear and retrieve through a newly passed second colored 7.5mm cannula through the superior midline portal. Retrieve the 2nd suture tape from the first anchor, reload the suture passer through the anteroinferior canula, and repass through the torn tendon, marching sutures more anteriorly. Grasp through the superior midline cannula, and then remove the cannula to clear for the second anchor with striped suture tape insertion. Seat the second anchor, retrieve and pass 3rd suture, and grasp through the midline superior cannula. The final suture can be left in the anteroinferior cannula after passing through the anterior extension of the torn tendon. Next, grasp the 2nd (solid colored) suture tape and bring it out to join with the final suture to be placed into the initial distal row anchor, which is loaded outside the anteroinferior cannula with sutures number 2 and 4 (one solid and one striped). Prepare with a thermal wand, a flat surface distal to the vastus ridge, and a site for a punch for the initial distal row anchor. while visualizing the punch seated in the hole, remove the punch and insert the tip of the anchor into the hole with the free ends of the sutures facing distally away from the tear, and individually tension both sutures until the slack is gone in the suture tape. Insert anchor until seated and use knot-cutter for a flush bone cut. Retrieve the 1st and 3rd sutures, load them into the second distal row anchor, and prepare the punch hole at least 1.5 cm from the other distal row anchor. Rotating the leg while resting the ankle on a mayo stand can expose a good flat site distal to the vastus ridge for the punch. Insert the tip of the anchor and tension each suture before seating the anchor and cut the suture tape flush with the bone (Fig. 4A). Visualize double row, knotless suture bridge repair by rotating the leg and assessing tendon-to-bone interface and water seal closure of gluteal tear (Fig. 4B).
Results
The retrospective review identified 10 patients who had undergone arthroscopic glute medius repair and had previous arthroplasty surgery. Eight patients had undergone total hip arthroplasty, and the remaining two had hemiarthroplasty of the hip. All ten patients complained of persistent lateral hip pain and associated weakness despite conservative management. Appropriate workup for infection, loosening, or referred pain and weakness was unremarkable. The average preoperative MHHS was 29.2 ± 11.8, scoring well below the threshold of 70 for a “Fair Result”. There was a significant increase in MHHS at the 1-year postoperative follow-up, yielding an average MHHS of 80.7 ± 10.2 (p < 0.0001). Every patient saw an increase in their MHHS, with an average increase of 51.5 ± 10.4 points. Categorizing the outcomes at one year, two patients still had a score that was categorized as a poor result (<70), one had a fair result (70-79), five had a good result (80-89), and two had an excellent result (>90). Individual MHHS for each patient can be seen in Table 1. All 10 patients reported resolution of lateral hip pain following surgery; however, most reported they felt some weakness at 1 year. All 10 patients underwent ultrasound imaging at least 6 months after the operation, and the images at that time demonstrated satisfactory healing of their repairs in each patient.
Discussion
Many articles have reported the success of endoscopic gluteus medius tendon repair in native hips, and open repair in arthroplasty patients (3,4). Patients discussed in our study comprise two of the four subgroups of gluteal tendon tears (femoral neck fractures and osteoarthritis). In a prospective study done by Bunker et al., gluteus medius tears were seen in 22% of elderly patients with femoral neck fractures (1). Howell et al. noted that in patients undergoing a total hip arthroplasty for osteoarthritis, up to 20% have abductor tears (2). The most common location for a gluteal tear is at the insertion sites on the lateral facet of the greater trochanter.
Studies using MRI and ultrasound have helped clarify the misconception that most GTPS cases are caused primarily by trochanteric bursitis. In a prospective study, Bird et al. used MRI to examine 24 women presenting with signs and symptoms of GTPS. The results of the imaging identified that trochanteric bursitis accounted for less than 10% of the actual cause of GTPS, while gluteal tendinopathy and full-thickness gluteal tears were present in 62.5% and 45.8% of cases, respectively (8). Long et al. performed a retrospective review of both male and female patients with GTPS who received an ultrasound. Only 20.2% of patients showed signs of trochanteric bursitis, while half of the patients had gluteal tendinosis or tears (11).
When imaging patients with previous hip arthroplasty, the metallic artifact of the implant may hinder the ability to diagnose this pathology from conventional MRI accurately. We encourage the use of dynamic ultrasound, which is inexpensive and often readily available in office and hospital settings. Interpretation of ultrasound results is operator-dependent and should be performed by a trained professional.
The diagnosis of GTPS caused by a gluteal tear can often be made clinically using the methods described above. The first and most reliable of these is the 30-second Trendelenberg test, which is assessed by having the patient stand on the affected leg and examining for pelvic tilt. MRI has helped confirm that a positive Trendelenberg test has 72.7% sensitivity and 76.9% specificity (8). Secondly, a patient’s ability to perform the single-leg squat test correlates with the strength of hip abductor muscles (9). Poor performance could indicate weakness of the hip abductors, due to damage of the gluteus medius muscle or tendon. Finally, the supine unilateral bridge test activates the gluteal muscles, and failure to maintain the position indicates muscle weakness. When used together, these clinical tests can substantially aid in accurately diagnosing a gluteus medius tear or tendinopathy.
Our findings are similar to another study in the literature looking at endoscopic repair of gluteus medius tears in patients with native hips. Voos et. al report satisfactory results in 10 patients, as well (4). All ten patients had complete resolution of lateral hip pain following repair. Their modified Harris Hip Scores averaged 94 at one year. Domb, et al, found excellent results after endoscopic repair of gluteal tendons in non-arthroplasty patients at two-year follow-up (17).
Though we also describe an endoscopic technique, open approaches can accomplish similar benefits for patients with gluteal tendon tears. Rajkumar et al. described open gluteus medius repairs in patients after total hip arthroplasty (3). Nine of the 11 patients were satisfied with the surgery and would recommend the procedure. Several other factors should be taken into consideration with endoscopic gluteus medius repairs. One factor is double-row versus single-row repair. Multiple articles in the shoulder literature have shown double-row repairs to be superior to single-row repairs in large and massive rotator cuff tear categories. Barber et al. described double-row repairs in the shoulder as having greater footprint coverage and less displacement during rotation, with a larger mean failure load in mechanical testing (5). Park et al. compared single and double-row fixation of rotator cuff repairs at two-year follow-up. Though no difference was seen in small to medium tears (less than 3 cm), large to massive tears showed statistically significant improvement in all outcome measures with double row techniques (12). A cadaveric study demonstrated that double-row repairs have statistically significant advantages in strength, gap formation, and resistance to cyclic displacement compared to single-row repairs (13). Re-tears of the surgical repair are lower when using a double repair (9.8%) compared to a single-row repair (25.6%) (14). Many comparisons can be made between the rotator cuff of the shoulder and the gluteal cuff; however, the lower extremity is unique due to its weight-bearing nature. The load demand of the gluteal tendons with ambulation can exceed 3.5 to 6 times body weight (15,16). Double-row repair strength may be beneficial and necessary for both small and large gluteal tendon tears due to the unique and increased stresses placed on the lower extremity.
Anchor placement is another key factor to take into consideration. Anatomic studies have described the broad insertion of the gluteus medius tendon onto the lateral facet of the greater trochanter as having the largest surface area (35mm) compared to the superoposterior facet insertion (8mm) (10). The lateral facet insertion, therefore, has the greatest tendon-to-bone contact and can easily accommodate two anchors with adequate spacing potential.
Osteoporotic bone must also be acknowledged as a critical factor in affecting tendon repair. Dishkin-Pasat et al. looked at two different double-row repair techniques in osteoporotic bone (6). They determined that the failure load of the double-row knotless lateral anchors strongly correlated to bone mineral density.
At short-term follow-up, we seem to have similar satisfying results in the endoscopic repair of gluteus medius tears in hip arthroplasty patients, compared to open repair in arthroplasty patients and endoscopic repair in native hips.
Limitations
A limitation of this study is our small sample size and single surgeon cohort. This could cause a selection bias, and limit the statistical power and generalizability of our findings. In an attempt to mitigate this, consecutive patients were selected. A larger sample size would provide better insight into the outcomes of this technique. Second, as a retrospective review, we cannot fully account for information that is not reported in the medical records. We also recognize the limitations with only using the modified Harris Hip Score (MHHS) for functional outcome assessment. Only using one outcome measure may not fully capture the true functional abilities of the patients. Using additional outcome measures could provide a better assessment of patient satisfaction and functional recovery. Lastly there is no control group in this study, which would have allowed for a better understanding of the impact of this technique in these patients.
Conclusion
Gluteus medius tears can significantly cause lateral hip pain and weakness after hip arthroplasty. A triad of gluteal symptoms is often present in these patients, including the single-leg squat test, unilateral bridge test, and positive Trendelenberg sign, are extremely useful for diagnosing gluteus medius tears. In our study, patients underwent an endoscopic double-row suture bridge repair as an outpatient procedure. In our short-term follow-up, repair of gluteus medius tears using our endoscopic technique appears to provide hip arthroplasty patients with gluteus medius tears significant pain relief, and help regain significant function. More long-term follow-up will be necessary to confirm our outcome results.
References
- Bunker TD, Esler CNA, Leach WJ. Rotator-cuff tear of the hip. J Bone Joint Surg Br. 1997;79(4): 618-620.
- Howell GE, Biggs RE, Bourne RB. Prevalence of abductor mechanism tears of the hips in patients with osteoarthritis. J Arthroplasty. 2001;16(1): 121-123.
- Rajkumar S, Singer GC, Jones JR. Results following repair of gluteus medius defects following total hip arthroplasty. Hip Int. 2011;21(3): 293-298.
- Voos JE, Shindle MK, Pruett A, Asnis PD, Kelly BT. Endoscopic repair of gluteus medius tendon tears of the hip. Am J Sports Med. 2009;37(4): 743-747.
- Barber FA, Drew OR. A Biomechanical Comparison of Tendon-Bone Interface Motion and Cyclic Loading Between Single-Row, Triple-Loaded Cuff Repairs and Double-Row, Suture-Tape Cuff Repairs Using Biocomposite Anchors. Arthroscopy. 2012;28(9): 1197-205
- Dishkin-Pasat JG, Salata MJ, Gross CE, Manno K, Shewman EF, Wang VM, Bush-Joseph CA, Nho SJ. A biomechanical comparison of repair techniques for complete gluteus medius tears. Arthroscopy. 2012;28(10): 1410-1416.
- Aaron DL, Patel A, Kayiaros S, Calfee R. Four common types of bursitis: diagnosis and management. J Am Acad Orthop Surg. 2011;19(6): 359-367.
- Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 2001;44(9): 2138-145.
- Crossley KM, Zhang WJ, Schache AG, Bryant A, Cowan SM. Performance on the single-leg squat task indicates hip abductor muscle function. Am J Sports Med. 2011;39(4): 866-873.
- Robertson WJ, Gardner MJ, Barker JU, Boraiah S, Lorich DG, Kelly BT. Anatomy and dimensions of the gluteus medius tendon insertion. Arthroscopy. 2008;24(2): 130-136.
- Long SS, Surrey DE, Nazarian LN. Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis. Am J Roentgenol. 2013;201(5): 1083-1086.
- Park JY, Lhee SH, Choi JH, Park HK, Yu JW, Seo JB. Comparison of the clinical outcomes of single- and double-row repairs in rotator cuff tears. Am J Sports Med. 2008;36(7): 1310-1316.
- Meier SW, Meier JD. The effect of double-row fixation on initial repair strength in rotator cuff repair: a biomechanical study. Arthroscopy. 2006;22(11): 1168-1173.
- Sugaya H, Maeda K, Matsuki K, Moriishi J. Functional and structural outcome after arthroscopic full-thickness rotator cuff repair: single-row versus dual-row fixation. Arthroscopy. 2005;21(11): 1307-1316.
- Crowninshield RD, Brand RA, Johnston RC. The effects of walking velocity and age on hip kinematics and kinetics. Clin Orthop. 1978;132: 140-144.
- Brand RA, Crowninshield RD. The effect of cane on hip contact force. Clin Orthop. 1980;147: 181-184.
- Domb BG, Botser I, Giordano BD. Outcomes of endoscopic gluteus medius repair with minimum 2-year follow-up. Am J Sports Med. 2013 May;41(5):988-97. doi: 10.1177/0363546513481575. Epub 2013 Mar 22. PMID: 23524152.
