
Michael R. McDermott M.S. DO1, Ante Rebic DO1, Luke DiPasquale DO1 and Jerrod Steimle DO1,2
1Kettering Health Grandview Orthopedic Surgery, Dayton Ohio
2Orthopedic Associates of Southwest Ohio, Dayton Ohio
DOI: 10.70709/ZXL123-0045
Background
Fracture nonunion is a rare but devastating outcome that can result in significantly increased morbidity and a lengthy recovery for the patient. In the cases of septic nonunion, treatment options include IV antibiotics and debridement of all nonviable bone. While this approach is often successful at clearing infection, it can result in a substantial bony void. To combat these defects, many surgeons have implemented multi-stage procedures such as the Masquelet technique (MT). MT is a well-studied concept that consists of debridement and the placement of an antibiotic cement spacer. After the infection has cleared, the second procedure removes the spacer and fills the void with bone graft. While successful, this multi-stage procedure can be associated with significant patient burden, a long, non-weight-bearing period, and an overall lengthy recovery. This case series highlights a variation of the standard MT technique, utilizing concepts of cement augmentation for fracture treatment while reducing the need for the second stage of the procedure.
Case Series
In this retrospective series, four consecutive patients with complicated fracture nonunions were subjected to a first-stage MT procedure with placement of an antibiotic polymethylmethacrylate cement spacer and definitive hardware placement. These nonunions included two distal femur fractures, a spiral humeral shaft fracture and a clavicle fracture. These four patients demonstrated good bone healing and quickly returned to their baseline activity levels. In each case, elective permanent retention of the cement spacer was discussed, and exchange for bone graft was only performed on an as-needed basis. All patients went on to develop bridging bone around the spacer with full healing of the adjacent cortices.
Conclusions
Maintaining the cement spacer allowed these patients to regain function quickly and return to their daily living activities while eliminating the risks associated with a second procedure.
Level of Evidence = IV
Keywords: Trauma, osteomyelitis, infected nonunion, Masquelet technique, Cement augmentation, Cement spacer, Reconstruction, bony defect, Polymethylmethacrylate, PMMA
Introduction
Nonunions are an uncommon, but feared complication following a fracture, occurring in 1.9 – 4.9% of fractures (1-4). While there is some variance in the definition of nonunions among surgeons, the FDA defines nonunions as a fracture at least nine months old that has not shown any evidence of healing for three consecutive months (2-4). Simple radiographs are often adequate for assessing healing, and a fracture is usually considered to be at union when three of the four cortices have healed. Patients who fail to achieve union can have debilitating outcomes, with studies demonstrating worse time trade-off scores than stroke, acute myocardial infarctions, and acute immunodeficiency syndrome (AIDS) (3-5). Many factors play a role in the development of a nonunion including injury mechanism, nutritional status, and tobacco use (1-3,6-8). In cases where the initial fracture does not heal, care is often transferred to an orthopedic traumatologist to salvage the fixation. While other options exist, reoperation is the mainstay of treatment, focusing on providing optimal fracture stabilization (9,10).
The salvage process can also be complicated by infection, non-viable bone, or severe comminution, making achieving the desired fixation difficult. If infection or non-viable bone is present, substantial debridement of the bony surface is required, often leading to a substantial bony void. The Masquelet technique (MT) is a two-stage procedure that was developed to specifically address these large bony defects, utilizing a PMMA cement space to fill the void, followed by removal of the cement spacer, replacement with bone grafting and definitive fixation 4-8 weeks later (11-12). While successful, this multi-stage procedure can be associated with significant patient burden, a long non-weight-bearing period, bone graft donor site morbidity, and an overall lengthy recovery (11-15). Cement augmentation (CA) has also been explored in fracture treatment showing improved screw purchase in femoral neck fractures, increased stability of trochanteric hip fractures, and significantly higher strength in distal radius fractures (16). The case series presented here demonstrates a variation of CA and the MT by permanently filling the large bony void with a cement spacer and maintaining it to treat complicated fracture nonunions.
Case Overview
This retrospective series presents four consecutive patients with various complicated fracture nonunions, which resulted in large bony defects following debridement. For each patient, bone grafting in the acute setting was not recommended due to the defect’s size and/or the concern for infection. Ultimately, an antibiotic polymethylmethacrylate (PMMA) cement spacer was placed to fill the bony void and hardware fixation was placed around or through the spacer. In each patient, the plan was to replace the spacer with a bone graft at the four-to-eight-week time point, in traditional MT fashion. All of the patients were doing well in the early postoperative period, and at eight weeks postoperatively, each patient elected permanent retention of the cement instead of planned cement removal and exchange for bone graft. All patients went on to develop bridging bone around the spacer with full healing of the adjacent cortices and observed a timely return to their activities of daily life. Each case is described below to demonstrate how this technique was applied to each fracture nonunion.
Clavicle Fracture Nonunion
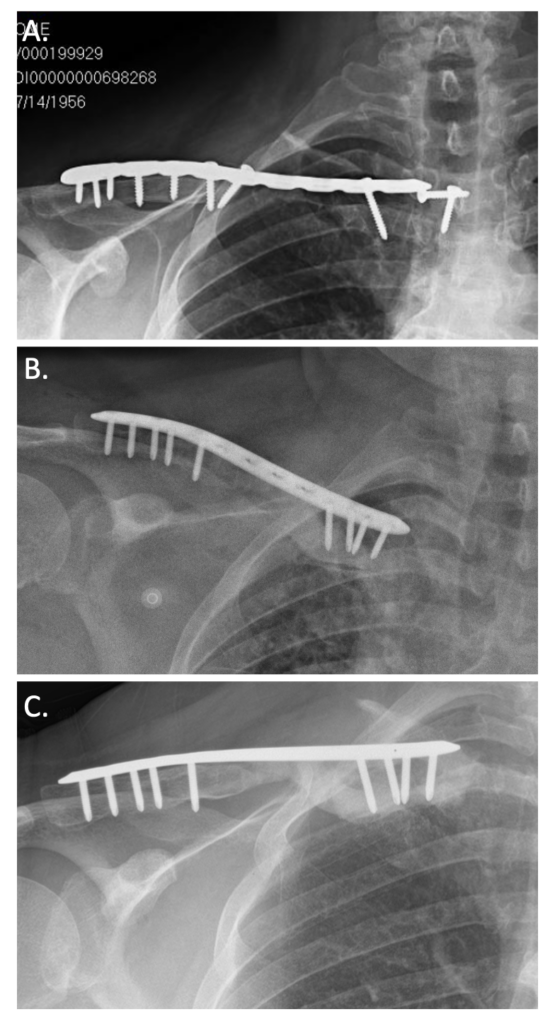
A 65-year-old diabetic female with a history of stage 3 liver fibrosis, hypertension, hypercholesterolemia, venous thromboembolism, and a previous clavicle fracture presents with clavicle pain, a clicking sensation, and discomfort when swallowing. Fifteen years earlier, she sustained a midshaft clavicle fracture which was treated operatively with plates and screws. Imaging on presentation demonstrated a nonunion of the clavicle with osteolysis and hardware loosening (Figure 1A). The patient elected to undergo revision open reduction internal fixation with the removal of her previous hardware and exchange for new implants. Intraoperatively, substantial bone loss was appreciated once the old implants were successfully removed. A 3 cm by 1 cm by 1 cm void was present with only a shell of bone remaining proximally. There was a concern for a possible deep infection, and intraoperative cultures were taken. Given the concern for infectious nonunion, it was decided to place an antibiotic cement spacer to fill the void, as acutely bone grafting in the setting of infection is not recommended. A superior locking plate was secured distally to the remnants of the cortical shell of bone using locking screws. The cement spacer was placed within the cortical shell and spanned across the nonunion site to fill the void. The cement was then allowed to cure, and holes were then drilled through the cement to allow for excellent screw purchase (Figure 1B). The intraoperative cultures were positive for infection. However, the definitive cultures were never able to be characterized beyond the rare growth of anaerobic gram-negative bacilli. The patient did well in the early postoperative period, quickly regaining arm motion. By three months, she was pain-free and back to her normal life. By six months, radiographic imaging demonstrated an intact plate and screw construct with bridging bone around the intact cement spacer (Figure 1C).
Distal Femur Fracture
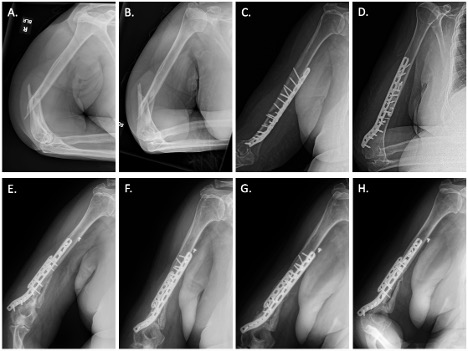
A 64-year-old diabetic male with a history of hypertension, coronary artery disease, peripheral artery disease, and previous left foot digit amputation secondary to a diabetic foot ulcer presented with a comminuted distal femur fracture with bilateral Hoffa fragments and ipsilateral tibial plateau fracture following a motor vehicle versus motorcycle collision (Figure 2:A-B). The patient was initially stabilized with an external fixator. Once soft tissue swelling had diminished, they underwent initial open reduction and internal fixation (ORIF) utilizing headless compression screws to realign the condyles, followed by a medial and lateral locking plate construct to stabilize the distal femur. An intramedullary tibial nail with rafting screws was used to treat the tibial plateau fracture (Figure 2:C-D). The patient initially did well postoperatively, but with subsequent follow-up visits, there was a developing concern for distal femoral nonunion, and a bone stimulator was added to salvage the initial fixation.
Unfortunately, by one year, this patient still did not have radiographic signs of union, and hardware replacement was deemed necessary. Intraoperatively, it was discovered that a large amount of bone was nonviable. Debridement led to a bony void measuring 8 cm by 6 cm by 6cm. The void was thought to be too large to acutely bone graft, therefore it was planned to proceed with an antibiotic cement spacer at this time. The femur was reconstructed to the appropriate length with locking plates and screws. The void was then washed with a copious amount of saline, followed by placement of the spacer (Figure2:E-F). The patient did well in the early postoperative period and progressed to weight bearing as tolerated (WBAT) with a walker by four weeks, fully ambulating pain-free with a cane by six months, and had discontinued the use of his cane by his nine-month visit. At twelve months, radiographic imaging demonstrated an intact plate and screw construct with bridging bone around an intact cement spacer (Figure 2: G-H).

Periprosthetic Distal Femur Fracture
A 79-year-old female with a history of hypertension, morbid obesity, tobacco use, and a memory disorder presented with a comminuted supracondylar distal femur periprosthetic fracture with a well-fixed total knee component (Figure 3 A-B). Once medically cleared, she underwent initial fixation with a locking plate construct (Figure 3 C-D). She did well in the initial postoperative period but developed an infection two weeks later and underwent irrigation and debridement. During debridement, a substantial amount of nonviable bone was noted, and after debridement, there was a 6.5 cm by 4.5 cm by 3.5 cm void. Given the concern for infection and the large size of the defect, acute bone grafting was not recommended; therefore, an antibiotic spacer was placed (Figure 3 E-F). She progressed well in the postoperative period and was able to begin weight-bearing as tolerated by three months. By eight months, radiographic imaging demonstrated an intact plate and screw construct with bridging bone around an intact cement spacer and stable total knee components (Figure 3 G-H).

Spiral Humeral Shaft Fracture
A 72-year-old female with a history of COPD, hypertension, hypothyroidism, morbid obesity, and a former smoker presents with an extraarticular, comminuted, short spiral fracture of the distal third of the humerus after a ground level fall. (Figure 4 A-B). Once medically cleared, she underwent open reduction and internal fixation with a locking plate construct (Figure 4 C-D). She did well in the initial postoperative period but unfortunately would have a hardware failure at 10 weeks with no signs of healing were seen after that point. There was concern for a deep infection, so she was scheduled for a revision procedure with an irrigation and debridement. After cultures were take, debridement of nonviable bone led to a bony void measuring a 7.2 cm by 3.5 cm by 2.5 cm. Given the concern for infection and the large size of the defect, acute bone grafting was not recommended; therefore, an antibiotic spacer was placed (Figure 4 E-F). She progressed well in the postoperative period and progressed well with therapy. At 4 months her pain has decreased and radiographic imaging demonstrated an intact plate and screw construct. She is now starting to have bridging bone growing around her intact cement spacer (Figure 4 G-H). Due to her improving symptoms, past medical history, and no additional broken hardware, we elected to forego bone grafting at this point.
Discussion
Since it was first described in 2000, the Masquelet technique has been successfully utilized to manage large bony defects secondary to septic nonunion, with literature demonstrating an 86% success rate (12). This case series demonstrates the adaptability of this technique and shows four patients with bony voids who achieved a stable and mechanically appropriate, pain-free lower extremity without the need to undergo an additional procedure.
The use of the MT has been used in a wide variety of settings in various complex fracture situations. In Japan, seven patients with acute tibial shaft fractures successfully underwent the MT, demonstrating its appropriate usage in an acute setting (17). In Egypt, thirty-two patients underwent a Masquelet/Ilizarov technique hybrid for septic tibial nonunion with a 94% rate of successful reconstruction with no recurrent infection (18). Despite the recommendation to perform the second procedure within 4-8 weeks, no literature has shown a clear correlation between an increased procedure interval and worsening outcomes (19). Interestingly, there is one reported case of a successful MT second-stage procedure eight years after the initial placement of the antibiotic spacer (20).
This case series demonstrates a hybrid of the MT and CA by placing a large cement spacer combined with definitive fixation. While the intent was to remove the spacer and bone graph a few weeks later, in each case, maintaining the cement spacer from the first stage of the MT allowed all four patients to regain function quickly, return to their baseline function without any complications, and showed radiographic healing of at least three of four cortices surrounding the spacer. Maintaining the cement spacer spared these patients from the risks, morbidity, and lengthy recovery associated with a second procedure. With the documented success of Assal’s procedure eight years following the first stage procedure, combined with the cases presented herein, we propose using cement as an adjunct to fill smaller bony voids and simultaneously augment fixation in the setting of a septic nonunion. The second stage could be postponed indefinitely and only performed later, if necessary, with good outcomes.
Conclusion
The Masquelet technique is a multistage procedure that has consistently been a successful option in treating nonunion and large bony voids. Cement augmentation has been shown to improve the purchase of hardware in patients with sub-optimal bone quality. This series demonstrates a successful variation of these techniques highlighted for voids and/or fractures with high comminution levels. Utilizing the cement spacer to not only fill the void but also as an augment for improved nonunion fixation allows for easier management of difficult nonunions. By postponing the second stage of the Masquelet technique and maintaining the cement spacer, the patients in this series had a timely return to their baseline activities without any of the risks associated with a second-stage surgery.
References:
- Zura R, Xiong Z, Einhorn T et al. Epidemiology of Fracture Nonunion in 18 Human Bones. JAMA Surg. 2016 Nov 16;151(11):e162775.
- Mills LA, Aitken SA, Simpson AHRW. The risk of non-union per fracture: current myths and revised figures from a population of over 4 million adults. Acta Orthop. 2017 Aug;88(4):434-439.
- Wildemann B, Ignatius A, Leung F et al. Non-union bone fractures. Nat Rev Dis Primers. 2021 Aug 5;7(1):57.
- Nicholson JA, Makaram N, Simpson A et al. Fracture nonunion in long bones: A literature review of risk factors and surgical management. Injury. 2021 Jun;52 Suppl 2:S3-S11.
- Schottel PC, O’Connor DP, Brinker MR. Time Trade-Off as a Measure of Health-Related Quality of Life: Long Bone Nonunions Have a Devastating Impact. J Bone Joint Surg Am. 2015 Sep 2;97(17):1406-10.
- Ekegren CL, Edwards ER, de Steiger R et al. Incidence, Costs and Predictors of Non-Union, Delayed Union and Mal-Union Following Long Bone Fracture. Int J Environ Res Public Health. 2018 Dec 13;15(12):2845.
- Mills LA, Simpson AH. The relative incidence of fracture non-union in the Scottish population (5.17 million): a 5-year epidemiological study. BMJ Open. 2013 Feb 8;3(2):e002276.
- Zura R, Braid-Forbes MJ, Jeray K et al. Bone fracture nonunion rate decreases with increasing age: A prospective inception cohort study. Bone. 2017 Feb;95:26-32.
- Brinker MR, O’Connor DP. Management of Aseptic Tibial and Femoral Diaphyseal Nonunions Without Bony Defects. Orthop Clin North Am. 2016 Jan;47(1):67-75.
- Rupp M, Biehl C, Budak M et al. Diaphyseal long bone nonunions – types, aetiology, economics, and treatment recommendations. Int Orthop. 2018 Feb;42(2):247-258.
- Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am. 2010 Jan;41(1):27-37; table of contents.
- Masquelet A, Kanakaris NK, Obert L et al. Bone Repair Using the Masquelet Technique. J Bone Joint Surg Am. 2019 Jun 5;101(11):1024-1036.
- Careri S, Vitiello R, Oliva MS et al. Masquelet technique and osteomyelitis: innovations and literature review. Eur Rev Med Pharmacol Sci. 2019 Apr;23(2 Suppl):210-216.
- Lavía KF, Boccolini HS, Hernández RA. Reconstruction of a tibial diaphyseal bone defect using the Masquelet technique. A case report. Trauma Case Rep. 2022 Nov 2;42:100728.
- Morelli I, Drago L, George DA et al. Masquelet technique: myth or reality? A systematic review and meta-analysis. Injury. 2016 Dec;47 Suppl 6:S68-S76.
- Larsson S. Cement augmentation in fracture treatment. Scand J Surg. 2006;95(2):111-8.
- Hatashita, S., Kawakami, R., Ejiri, S. et al. ‘Acute Masquelet technique’ for reconstructing bone defects of an open lower limb fracture. Eur J Trauma Emerg Surg (2021) 47, 1153–1162.
- Khaled A, El-Gebaly O, El-Rosasy M. Masquelet-Ilizarov technique for the management of bone loss post debridement of infected tibial nonunion. Int Orthop. 2022 Sep;46(9):1937-1944.
- Alford AI, Nicolaou D, Hake M et al. Masquelet’s induced membrane technique: Review of current concepts and future directions. J Orthop Res. 2021 Apr;39(4):707-718.
- Assal M, Stern R. The Masquelet procedure gone awry. Orthopedics. 2014 Nov;37(11):e1045-8.
