
Alfred-John Bayaton, DO1, Michael McDermott, DO2, Lindsey K. Meding, BS3, Ashish Patel, MD1
1The Spine Center, Duly Health and Care, Naperville, IL
2Kettering Health Grandview, Dayton OH
3William Carey University College of Osteopathic Medicine, Hattiesburg MS
DOI: 10.70709/9021-RT56
Abstract
Vertebral body fracture is the most common manifestation of proximal junctional failure (PJF), a frequent complication following adult spinal deformity surgery and a leading cause of reoperation(1). In the absence of established consensus regarding optimal revision techniques for PJF, this case report presents two patients with non-traumatic vertebral fractures secondary to PJF, successfully managed with intravertebral reduction device (SpineJack®) and bone cement augmentation, combined with the extension of previous instrumentation. While the etiology of PJF in these two cases remains undetermined, this report aims to contribute to the evolving literature on surgical revision strategies for PJF, particularly in the context of vertebral fractures.
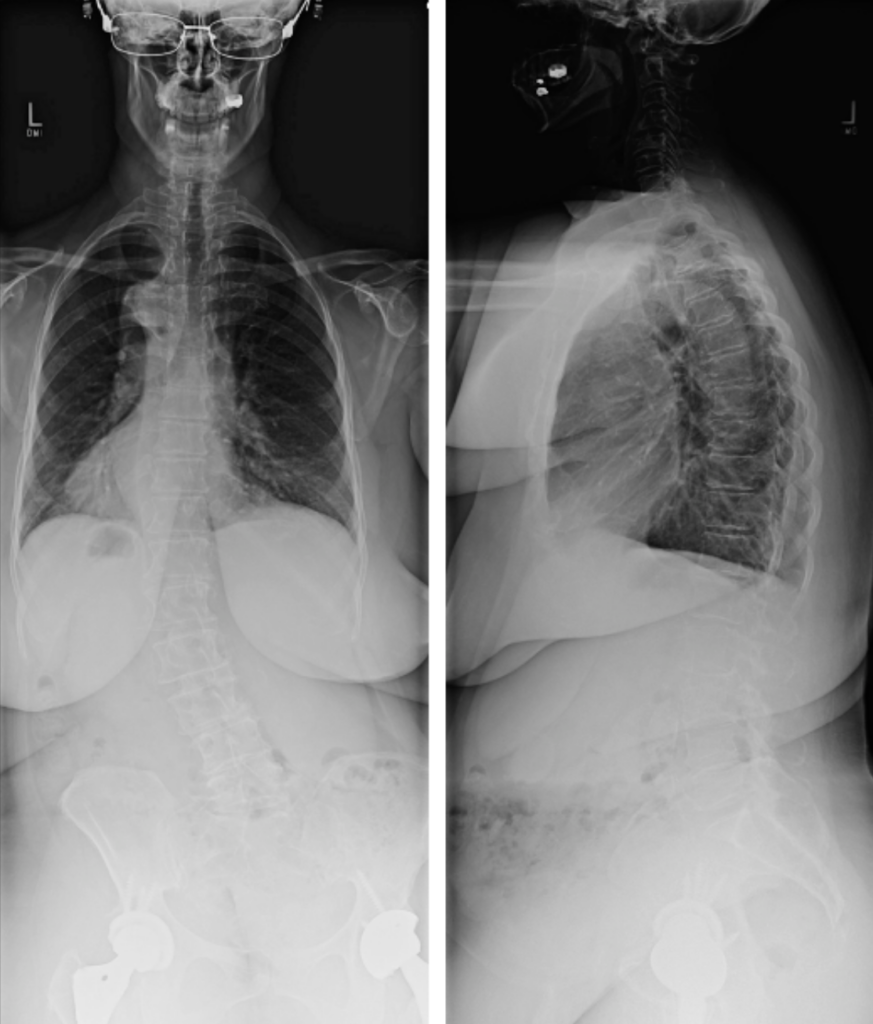
The first case involves a 62-year-old female with degenerative scoliosis, flat back deformity, adult idiopathic scoliosis, coronal malalignment, and degenerative disc disease with lateral listhesis underwent lateral lumbar interbody fusion (LLIF) at L2-3, L3-4, and L4-5 with titanium interbody devices and posterior L1 to pelvis instrumentation and fusion. Following L1 compression fracture at the proximal end of the instrumentation, the patient underwent surgical revision at 6 weeks postoperative. The pedicle screws at L1 were explanted, and the pedicle tracks were utilized for open placement of SpineJack® implants under fluoroscopic guidance to reduce and elevate the compressed L1 vertebra, restoring anterior vertebral height. The postoperative course was unremarkable, and the patient exhibited significant clinical improvement.
The second case involves a 60-year-old female patient with a history of painful thoracolumbar scoliosis who underwent a T8-Pelvis posterior spinal fusion (PSF) with multiple Smith-Petersen osteotomies (SPOs) and L4-S1 transforaminal lumbar interbody fusion (TLIF) with right-sided instrumentation. Following discovery of a T8 vertebral compression fracture at 8 weeks postoperative, existing hardware at the fracture level was removed, and SpineJack® implants were inserted bilaterally into T8, under fluoroscopic direction. The patient’s postoperative course was unremarkable with significant clinical improvement in pain and neurological function. This report aims to contribute to the literature on surgical strategies for managing vertebral fractures associated with PJF. The use of SpineJack® with cement augmentation appears effective in restoring vertebral body height and spinal alignment while offering a less invasive alternative to more extensive procedures like vertebral column resection (VCR). This technique may offer promising results for spine surgeons addressing vertebral fractures in the context of PJF. While the limitations inherent to case reports preclude establishment of intravertebral reduction devices with cement augmentation as a standard clinical practice guideline for vertebral fractures in the setting of proximal junctional kyphosis and/or failure (PJK/PJF), the successful treatment of two patients with this combined approach aims to contribute to the existing literature by presenting the safety and efficacy of such a technique. It suggests its potential utility for spine surgeons encountering this PJF vertebral fractures moving forward.
Keywords: Spine, PJF, intravertebral reduction, kyphosis, vertebral column resection
Introduction
Vertebral body fracture is the most common manifestation of proximal junctional failure (PJF), a frequent complication following adult spinal deformity surgery and a leading cause of reoperation (1). PJF is associated with increased need for revision, risk of neurological injury, deformity, and pain (1,2,3). In the absence of established consensus regarding optimal revision techniques for PJF, this case series presents two patients with non-traumatic vertebral fractures secondary to PJF, successfully managed with intravertebral reduction device, SpineJack® System (Stryker Corporation; Kalamazoo, MI.) with bone cement augmentation, and combined with the extension of previous instrumentation. While the etiology of PJF in these two cases remains undetermined, this report aims to contribute to the evolving literature on surgical revision strategies for PJF, particularly in the context of vertebral fractures.
Case Presentation
The first case involves a 62-year-old female with degenerative scoliosis, flat back deformity, adult idiopathic scoliosis, coronal malalignment, and degenerative disc disease with lateral listhesis (Figure 1) who underwent lateral lumbar interbody fusion (LLIF) at L2-3, L3-4, and L4-5 with titanium interbody devices and posterior L1 to pelvis instrumentation and fusion.
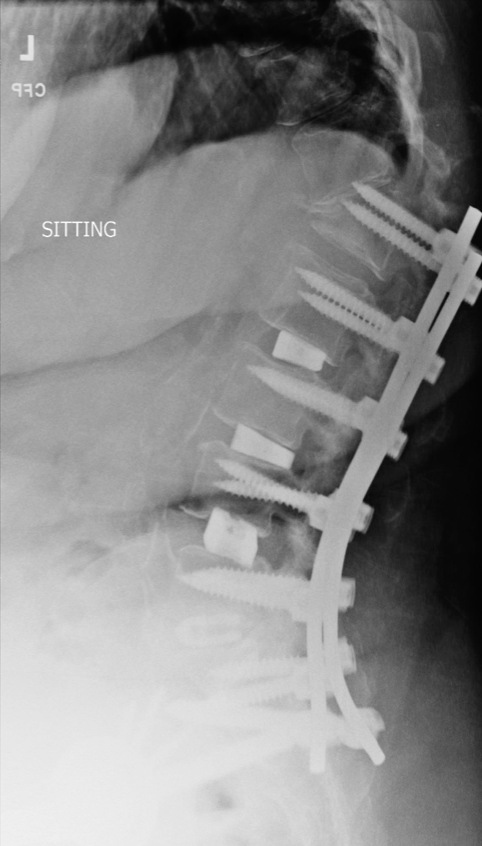
The initial postoperative course was uneventful. However, five weeks postoperatively, the patient presented with urinary tract infection, altered mental status, wound erythema and drainage, and superficial dehiscence. One week later, the patient developed increased pain, proximal junctional kyphosis (PJK), and an L1 compression fracture at the proximal end of the instrumentation, along with new neurological deficits (Figure 2).
Surgical revision was performed at six weeks postoperatively. The prior incision was extended proximally to T9, and the L1 segment was re-exposed. The pedicle screws at L1 were explanted, and the pedicle tracks were utilized for open placement of intravertebral reduction device implants under fluoroscopic guidance to reduce and elevate the compressed L1 vertebra, restoring anterior vertebral height. Percutaneous bone cement augmentation of L1 was performed to maintain fracture reduction, followed by posterior element decortication and grafting. New pedicle screws from T9 to T12 and supplemental titanium rods spanning from the pelvis to T9 were implanted, with an additional rod bridging the fracture site.
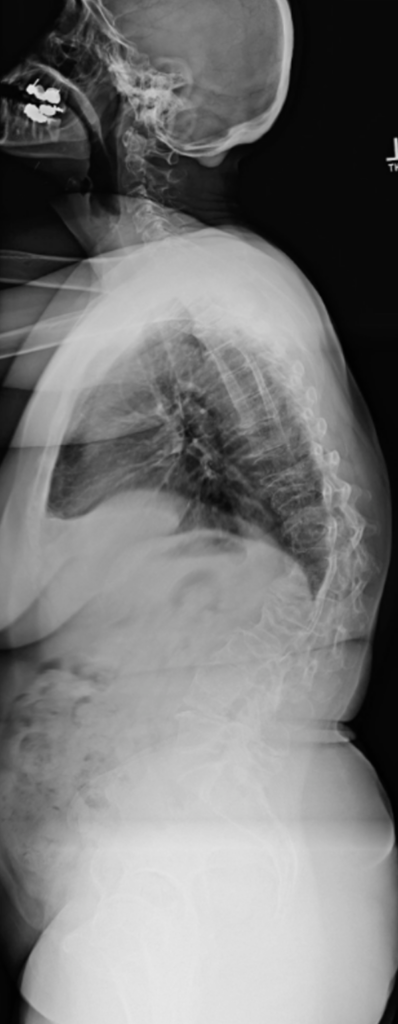
The postoperative course was unremarkable. The revision surgery successfully restored vertebral body height and corrected the kyphotic deformity. At one year postoperatively, the patient exhibited significant clinical improvement, with imaging confirming the integrity of the intravertebral reduction device implants, appropriate hardware positioning, and improved coronal and sagittal spinal alignment (Figure 3).

The second case involves, a 60-year-old female patient with a history of painful thoracolumbar scoliosis who underwent a T8-Pelvis posterior spinal fusion (PSF) with multiple Smith-Petersen osteotomies (SPOs) and L4-S1 transforaminal lumbar interbody fusion (TLIF) with right-sided instrumentation (Figure 4).
Despite initial progress in rehabilitation, the patient experienced an acute decline at eight weeks postoperatively. She presented in the office with proximal back pain, bilateral lower extremity weakness, and hyperreflexia in the legs. Imaging studies revealed a non-traumatic T8 vertebral compression fracture with associated spondylolisthesis, proximal screw cut out and proximal junctional kyphosis (PJK) (Figure 5).

The patient was directly admitted from the office and surgical revision was performed the next day to address the fracture and associated neurological compromise. The previous surgical site was reopened, and subperiosteal dissection was performed to expose the fractured T8 vertebra. Existing hardware at the fracture level was removed, and intravertebral reduction device implants were inserted bilaterally into T8, under fluoroscopic direction. The implants were then expanded to restore vertebral body height, and each was augmented with bone cement. Following vertebral augmentation, the existing spinal instrumentation was extended to T4 with four rods connected by axial and side-to-side connectors to provide additional stability to the construct. The posterior elements from T4-T9 were decorticated, and a combination of autograft and allograft bone, along with bone morphogenetic protein (BMP), was applied to promote fusion.
The patient’s postoperative course was unremarkable, with significant improvement in pain and neurological function. One year after surgery, she had progressed from wheelchair dependence to ambulating with a cane. Imaging studies demonstrated that the intravertebral reduction device implants at the fracture site remained intact, the hardware was correctly positioned, and the overall alignment of the spine was within normal parameters (Figure 6).

Discussion
Our study looks to add to the current body of literature on the management of anterior column bone loss and/or vertebral fractures in the setting of proximal junctional failure (PJF). We present two cases of revision adult deformity surgery using an intravertebral body reduction device, SpineJack® (Stryker, Kalamazoo, MI USA) with cement augmentation.
With the aging global population, the incidence of adult spinal deformity (ASD) and subsequent surgical interventions may increase. Proximal junctional kyphosis (PJK), a recognized complication of ASD surgery, is defined as a change in the sagittal Cobb angle exceeding 10 degrees or a minimum 10-degree increase from the preoperative measurement (3,5). Structural failure and mechanical instability, manifesting as vertebral body fracture, implant complications, or disruption of the posterior ligamentous complex, is the hallmark of proximal junctional failure (PJF). This distinguishes PJF from the less severe proximal junctional kyphosis (PJK), which does not typically involve such structural compromise (1,2,3,6).
The etiology of proximal junctional kyphosis (PJK) is multifactorial and remains a topic of considerable debate, with most cases diagnosed within the first postoperative year (7,8). The clinical significance of PJK, whether it is merely a radiographic finding or a condition that substantially impacts clinical outcomes, continues to be questioned. Although no single definitive predictor of PJK or proximal junctional failure (PJF) exists, various interrelated factors are believed to contribute to their development. Surgical risk factors, such as fusion extending to the sacro-pelvis, combined anterior-posterior spinal fusion, extensive open dissection of adjacent structures, persistent sagittal imbalance, and overcorrection of sagittal alignment, are well-documented (2). Non-surgical factors, including advanced age (>55 years) and severe preoperative sagittal imbalance, also heighten the risk (9). While the roles of elevated body mass index, comorbidities, and low bone mineral density are less conclusive, they may also serve as contributing factors (9). The debate extends to whether PJK arises from natural processes, such as the recurrence of pre-existing deformities or age-related spinal changes, or is a direct consequence of surgical intervention, which can disrupt the posterior soft tissue tension band, alter spinal biomechanics, and accelerate adjacent segment degeneration. It is likely that both surgical and natural factors play significant, interconnected roles in PJK pathogenesis, with surgical interventions potentially exacerbating pre-existing vulnerabilities.
In contrast to PJK, which is often asymptomatic and lacks significant structural compromise, proximal junctional failure (PJF) is a more severe condition characterized by mechanical instability and structural failure, often necessitating surgical revision (1,2,3,8). The structural failure associated with PJF manifests in three primary ways: disruption of the posterior osseo-ligamentous complex, implant failure (including pullout or breakage), and most frequently, vertebral fracture (2,6,7). Neurological compromise, including weakness, sensory changes, or spasticity, is a distinguishing feature of PJF compared to PJK (1,2,3,8,9). Additional clinical manifestations of PJF range from severe pain and neurological deficits to milder symptoms like back pain and altered posture (1,2,3,8). Kyphotic deformity, tenderness at the instrumentation site, and implant prominence are also notable findings. PJF frequently manifests acutely in the early postoperative period, although it can also progress gradually over time.
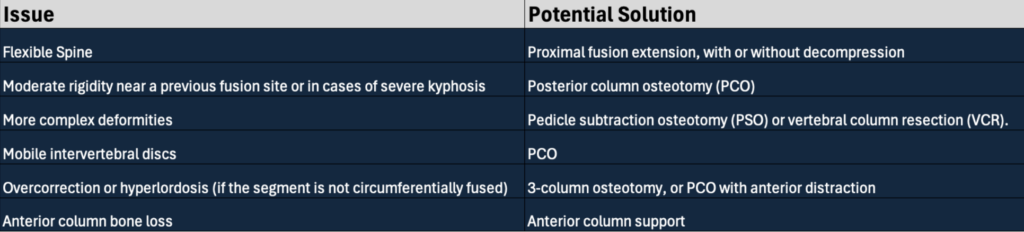
Accurate diagnosis of PJF requires a comprehensive radiographic evaluation, beginning with upright long-cassette radiographs as the initial imaging modality. Computed tomography (CT) and magnetic resonance imaging (MRI) may then be used for a more detailed assessment of the deformity, associated fractures, and neural structures (9). Although no standardized protocols currently exist for revision surgeries in proximal junctional failure (PJF), a fundamental principle guiding surgical decision-making is the consideration of individual patient needs and the specific anatomical defects present. Upon diagnosis of PJF, a strategic approach involves evaluating several key factors: spinal flexibility, overall severity and rigidity of the deformity, presence and degree of rigidity near a prior fusion, severe kyphosis, mobility of the intervertebral discs, presence of overcorrection or hyperlordosis, and the need for anterior column support (10,11).
In cases where the spine retains flexibility, a proximal fusion extension, with or without decompression, may be sufficient. However, when moderate rigidity is present near a previous fusion site or in cases of severe kyphosis, a posterior column osteotomy (PCO) is often indicated. More complex deformities may necessitate more extensive procedures such as pedicle subtraction osteotomy (PSO) or vertebral column resection (VCR). For patients with mobile intervertebral discs, PCO can also be an effective solution. In contrast, overcorrection or hyperlordosis may require a 3-column osteotomy if the segment is circumferentially fused, or a PCO with anterior distraction if not. Finally, if anterior column bone loss is present, anterior column support can be employed to improve sagittal correction, promote fusion and reduce the failure rate (Figure 7) (10,11).
Anterior column bone loss is a common manifestation of proximal junctional failure (PJF) (2,3), often presenting as vertebral compression fractures (VCFs). VCFs are also the most frequently reported fragility fracture, with an estimated 1 to 1.5 million cases annually in the United States (12). While non-surgical treatments like medications, bracing, and physical therapy are available, these options are often poorly tolerated by patients. Minimally invasive percutaneous procedures, such as vertebroplasty and kyphoplasty, have demonstrated efficacy in treating symptomatic VCFs (12).
Vertebroplasty and kyphoplasty are established minimally invasive procedures utilized in the management of painful vertebral compression fractures (13,14,15). Vertebroplasty involves the direct injection of bone cement into the fractured vertebra, whereas kyphoplasty incorporates an initial step of utilizing an inflatable bone tamp to restore vertebral height prior to cement injection. Kyphoplasty was developed as an advancement upon vertebroplasty, aiming to enhance procedural control and potentially improve patient outcomes. However, a recognized limitation of kyphoplasty is the potential for loss of restored vertebral height after balloon deflation due to the inherent elastic recoil of the compressed bone. Furthermore, the force distribution during balloon kyphoplasty is largely dictated by the interaction between the balloon and individual patient anatomy, often following the path of least resistance rather than the surgeon’s precise intention. This passive nature of force application can lead to suboptimal fracture reduction and anatomical restoration (13,14,15).
To address the limitations of traditional vertebral augmentation, expandable intravertebral implants have emerged as a promising alternative. These devices enable a more active and controlled approach to fracture reduction, potentially minimizing height loss and facilitating precise force application. Among the available options, the SpineJack® system distinguishes itself with its smaller size compared to similar devices like Vertebral Body Stenting (VBS®) (DePuy Synthes; Raynham, MA.) and its unique cranio-caudal expansion mechanism (16). In contrast to multidirectional expansion devices, which may create additional cavities within the vertebral body, SpineJack®’s vertical expansion generates two vertical fissures that are filled with bone cement. This injected cement interdigitates within the bone trabeculae between the implants, effectively creating a supportive ring around the vertebral endplates, which enhances support areas and improves load distribution throughout the vertebra (17,18). Furthermore, the SpineJack® system minimizes disruption to healthy, unfractured bone, allowing for increased cement interface and contact area, thus enhancing construct stability. As the device remains within the vertebral body, less cement is required for stabilization, further contributing to its advantages over other systems.
Although vertebral column resection (VCR) is a viable surgical option for severe kyphotic deformities resulting from vertebral body fractures, its inherent risks and morbidity often relegate it to a last-resort procedure. As suggested by Lehmer et al., patients with fractured vertebral bodies and posterior height exceeding two-thirds of the vertebral body may be suitable candidates for pedicle subtraction osteotomy (PSO) (19). However, posterior vertebral column resection (PVCR) may be considered for patients with posterior height less than two-thirds, requiring local correction of 35° or more, or presenting with rigid kyphosis (20). In the present case, the kyphotic deformity and fracture were deemed acute and non-rigid due to the timing of their discovery, 6 to 8 weeks after the initial procedure. Therefore, we opted for SpineJack with cement augmentation and extension of the previous instrumentation as the first-line treatment, prioritizing its less invasive nature and lower inherent risk compared to VCR.
Conclusion
The results from this case series suggests that intravertebral reduction devices combined with cement augmentation and extension of instrumentation may be a viable option for managing vertebral fractures associated with proximal junctional failure (PJF). While case reports inherently limit the generalizability of findings, the observed safety and efficacy in these cases indicate that this approach could be considered in similar clinical scenarios. Further studies, including larger cohorts and comparative trials, are necessary to establish more definitive guidelines and to better understand the long-term outcomes of this technique in the management of PJF-related vertebral fractures.
References:
- Hostin R, McCarthy I, OʼBrien M, et al. Incidence, mode, and location of acute proximal junctional failures after surgical treatment of adult spinal deformity. Spine (Phila Pa 1976). 2013;38(12):1008-1015. doi:10.1097/BRS.0b013e318271319c
- Hart R, McCarthy I, Oʼbrien M, et al. Identification of decision criteria for revision surgery among patients with proximal junctional failure after surgical treatment of spinal deformity. Spine (Phila Pa 1976). 2013;38(19):E1223-1227. doi:10.1097/BRS.0b013e31829fedde
- Hart RA, McCarthy I, Ames CP, Shaffrey CI, Hamilton DK, Hostin R. Proximal junctional kyphosis and proximal junctional failure. Neurosurg Clin N Am. 2013;24(2):213-218. doi:10.1016/j.nec.2013.01.001
- Jesse MK, Cleveland AW, Reiter MJ, Patel VV, Kleck CJ. Transpedicular-Transdiscal Cement Augmentation Treatment of Thoracolumbar Fusion Proximal Junctional Failure. Int J Spine Surg. 2019;13(5):470-473. doi:10.14444/6062
- Glattes RC, Bridwell KH, Lenke LG, Kim YJ, Rinella A, Edwards C. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: incidence, outcomes, and risk factor analysis. Spine (Phila Pa 1976). 2005;30(14):1643-1649. doi:10.1097/01.brs.0000169451.76359.49
- Watanabe K, Lenke LG, Bridwell KH, Kim YJ, Koester L, Hensley M. Proximal junctional vertebral fracture in adults after spinal deformity surgery using pedicle screw constructs: analysis of morphological features. Spine (Phila Pa 1976). 2010;35(2):138-145. doi:10.1097/BRS.0b013e3181c8f35d
- Yagi M, King AB, Boachie-Adjei O. Incidence, risk factors, and natural course of proximal junctional kyphosis: surgical outcomes review of adult idiopathic scoliosis. Minimum 5 years of follow-up. Spine (Phila Pa 1976). 2012;37(17):1479-1489. doi:10.1097/BRS.0b013e31824e4888
- Kim HJ, Yagi M, Nyugen J, Cunningham ME, Boachie-Adjei O. Combined anterior-posterior surgery is the most important risk factor for developing proximal junctional kyphosis in idiopathic scoliosis. Clin Orthop Relat Res. 2012;470(6):1633-1639. doi:10.1007/s11999-011-2179-1
- Nguyen NLM, Kong CY, Kebaish KM, Safaee MM, Ames CP, Hart RA. Diagnosis and Classification of Proximal Junctional Kyphosis and Proximal Junctional Failure. In: Klineberg EO, ed. Adult Lumbar Scoliosis. Springer International Publishing; 2017:195-216. doi:10.1007/978-3-319-47709-1_17
- Cerpa M, Sardar Z, Lenke L. Revision surgery in proximal junctional kyphosis. Eur Spine J. 2020;29(Suppl 1):78-85. doi:10.1007/s00586-020-06320-y
- Nguyen NLM, Kong CY, Hart RA. Proximal junctional kyphosis and failure-diagnosis, prevention, and treatment. Curr Rev Musculoskelet Med. 2016;9(3):299-308. doi:10.1007/s12178-016-9353-8
- Donnally III CJ, DiPompeo CM, Varacallo M. Vertebral Compression Fractures. In: StatPearls. StatPearls Publishing; 2024. Accessed June 27, 2024. http://www.ncbi.nlm.nih.gov/books/NBK448171/
- Krüger A, Oberkircher L, Figiel J, et al. Height restoration of osteoporotic vertebral compression fractures using different intravertebral reduction devices: a cadaveric study. Spine J. 2015;15(5):1092-1098. doi:10.1016/j.spinee.2013.06.094
- Krüger A, Baroud G, Noriega D, et al. Height restoration and maintenance after treating unstable osteoporotic vertebral compression fractures by cement augmentation is dependent on the cement volume used. Clin Biomech (Bristol, Avon). 2013;28(7):725-730. doi:10.1016/j.clinbiomech.2013.06.007
- Eck JC, Nachtigall D, Humphreys SC, Hodges SD. Comparison of vertebroplasty and balloon kyphoplasty for treatment of vertebral compression fractures: a meta-analysis of the literature. Spine J. 2008;8(3):488-497. doi:10.1016/j.spinee.2007.04.004
- Moura DL, Gabriel JP. Expandable Intravertebral Implants: A Narrative Review on the Concept, Biomechanics, and Outcomes in Traumatology. Cureus. 2021;13(9):e17795. doi:10.7759/cureus.17795
- Vanni D, Galzio R, Kazakova A, et al. Third-generation percutaneous vertebral augmentation systems. J Spine Surg. 2016;2(1):13-20. doi:10.21037/jss.2016.02.01
- Rotter R, Schmitt L, Gierer P, et al. Minimum cement volume required in vertebral body augmentation–A biomechanical study comparing the permanent SpineJack device and balloon kyphoplasty in traumatic fracture. Clin Biomech (Bristol, Avon). 2015;30(7):720-725. doi:10.1016/j.clinbiomech.2015.04.015
- Yagi M, King AB, Boachie-Adjei O. Incidence, risk factors, and natural course of proximal junctional kyphosis: surgical outcomes review of adult idiopathic scoliosis. Minimum 5 years of follow-up. Spine (Phila Pa 1976). 2012;37(17):1479-1489. doi:10.1097/BRS.0b013e31824e4888
- Hasegawa T, Ushirozako H, Yamato Y, et al. Impact of Spinal Correction Surgeries with Osteotomy and Pelvic Fixation in Patients with Kyphosis Due to Osteoporotic Vertebral Fractures. Asian Spine J. 2021;15(4):523-532. doi:10.31616/asj.2020.0016
