
S. Jake Shine DO1; H. Brent Bamberger DO1; Adam Dann DO1; Kanu Goyal DO2
1Kettering Health Network Grandview Medical Center Orthopedic Surgery Residency
2The Ohio State University Department of Orthopedics
DOI: 10.70709/KJ8765-MP
Abstract
The painful, stiff elbow can be a debilitating problem for patients, especially the young and active. Few good options exist for this population, as the limitations that come with total elbow arthroplasty are typically poorly tolerated. Distraction interposition elbow arthroplasty is a viable alternative to alleviate pain and restore function in this group. The literature is limited and the few available studies have shown unpredictable outcomes with a high complication rate, yet it continues to score well in terms of patient reported satisfaction scores and can prove beneficial in a population with few other options. Success depends on careful patient selection and expectations, preoperative stability, and precise recreation of the normal joint axis. Recent advances in both technique and implants have shown promise in expanding the indications and improving the success of this procedure.
Keywords: Arthroplasty, interposition, arthritis, elbow, salvage, young
Introduction
The optimal treatment of severe elbow arthritis remains elusive, especially for the population of younger active patients. When elbow arthritis is present, significant disability can follow. Basic activities of daily living such as eating and hygiene require a minimum flexion/extension arc of 30-130 degrees (though this is somewhat variable in the literature) and pronation/supination of 50 degrees, with flexion deficits most poorly tolerated1. While motion short of this is not an absolute indication for surgery, it certainly warrants consideration in an attempt to restore motion to functional levels, with a priority on flexion.
Mild and moderate cases of elbow arthritis are generally adequately managed with non-operative interventions such as simple stretching programs, splinting, corticosteroid injections, anti-rheumatic drugs, etc., depending on the etiology. For those who fail conservative management, however, there are a number of surgical options available. Open or arthroscopic debridement and capsular release or olecranon fossa debridement can be particularly useful in cases of post-traumatic arthritis with bony blocks, osteophytes, loose bodies, or capsular contractures that block or restrict motion1. In patients >65 years old with advanced rheumatoid or primary osteoarthritis and lower functional demands, hemi or total elbow arthroplasty (TEA) can be effective in restoring motion and alleviating pain2. Despite its success in certain patient populations, however, it comes with significant functional limitations and considerable risk of additional surgery if performed in younger or higher demand patients2. In this population with significant cartilage loss and motion restrictions but preserved ulnohumeral bone stock, interposition arthroplasty can be a reasonable option to restore motion to a functional level1.
The concept of interposition arthroplasty originated around 1860 as an improvement on the basic resection arthroplasty in an attempt to correct joint ankylosis3. It started with a wood block interposed in the temporomandibular joint, followed by trials of numerous different joints and interposition materials, both organic and non-organic, with varying degrees of success3. In the early 1900s, it was discovered that autogenous fat and fascia grafts provided the greatest longevity with the most comparable properties to the native joint, which significantly improved the success rate4. As the techniques and grafts continued to improve, outcomes followed, and the procedure gained traction4.
Today, there are a few common graft materials for interposition. An Achilles tendon allograft is a popular choice in the literature and is our preference due to its bulk and longevity, sufficient length for collateral ligament reconstruction if necessary, lack of a donor site, and inclusion of calcaneal bone for graft if needed4. There is no literature to our knowledge comparing grafts, however, and acceptable alternatives commonly reported in the literature include fascia lata, dermal graft, and synthetic allografts5. Fascia lata has the benefits of ease of harvesting and lack of donor site morbidity but is thinner and less robust than achilles and as such often must be doubled over to achieve adequate graft thickness and prevent early failure6. Dermal grafts are often thick and durable with good bony adherence but can be more challenging to harvest with the potential for higher donor site morbidity5. Finally, newer synthetic grafts are effective and avoid the need for graft harvesting and donor sites, but at a significantly higher cost5.
Indications/Contraindications
While the exact indications and contraindications for this procedure continue to be debated, there are a few common themes. It is generally agreed upon that the best candidates for this procedure are young or physiologically young (<60 years old), relatively high-functioning patients with end-stage elbow post-traumatic or primary osteoarthritis and significant loss of motion and function7. For the older or less active patient populations that can tolerate the restrictions of a conventional TEA, this remains the preferred treatment1.
The only absolute contraindications are recent septic arthritis, absence of flexion motor power, open physes, and significant loss of bone4. Pain without significant dysfunction or motion restriction as well as significant pre-operative instability are relative contraindications due to the risk of further disability and lower functional scores resulting from post-operative instability7. Finally, rheumatoid patients should be given careful consideration due to the likelihood of poor bone stock, instability, and lower functional demand, all of which are associated with poorer outcomes8. Figure 1 shows the preoperative radiographs of a patient who underwent this procedure for chronic ulnohumeral subluxation and significant post-traumatic arthritis with restricted range of motion, and whose case will be used to demonstrate the technique through intraoperative photos. This patient’s pre-operative active range of motion was restricted to 20-80 degrees flexion/extension, passively flexion to about 110 degrees with significant pain, pronation of 70 degrees, and supination of 20 degrees.
As with any surgery but particularly important here due to the narrow indications and high risk profile, a thorough discussion regarding the specific goals and risks prior to committing to surgery is crucial for patient satisfaction5. It should be clearly communicated that the surgery aims to give the patient a mobile, functional elbow, but that this may come at the cost of instability, unchanged or worsened pain, or future surgery. Shared decision making after thorough discussion will help ensure that the surgery is performed for the appropriate reasons.

Choice of External Fixators
The primary purpose of the fixator is to maintain a concentric reduction of the ulnohumeral joint to protect the resurfaced joint and allow the static elbow stabilizers to scar in while still allowing for early postoperative range of motion 4. If the primary elbow static and dynamic stabilizers are left intact and the elbow is stable post-operatively, the use of an external fixator is not necessary, however its addition can be of benefit in maximizing graft longevity and minimizing post-operative instability4.
There are multiple fixator options currently on the market and some are better suited than others for use with this procedure. The choice of fixator will depend on the amount of stability needed, patient lifestyle and body habitus factors, and the familiarity of the surgeon with the device and its application technique9. A list comparing a few commonly used fixator styles as well as their features, pros and cons, and examples of each is included in Table 19,10.
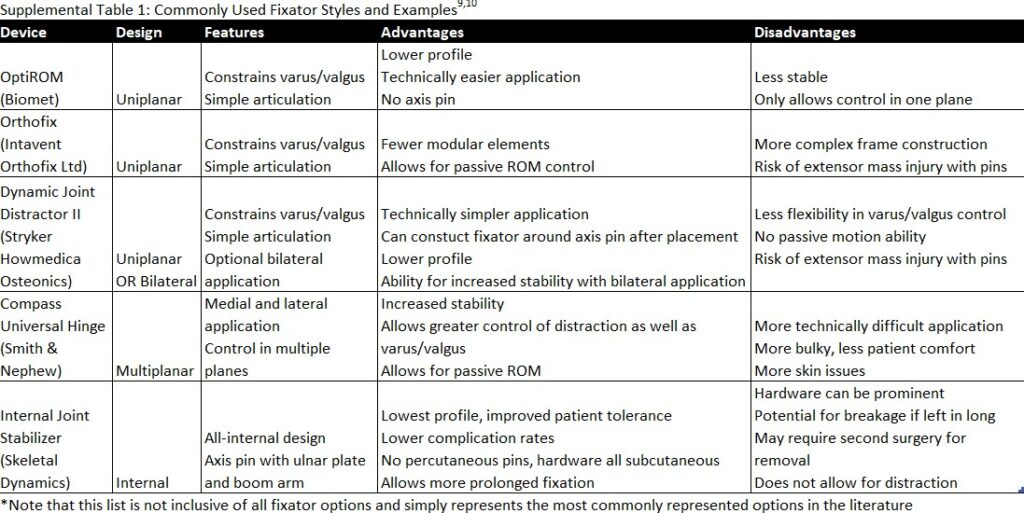
Due to the importance of axis pin placement, congruent joint space, and equal distraction across the joint, it is important to choose a fixator with a radiolucent frame which allows fluoroscopic visualization of the joint during application5. Additional considerations based on patient needs include unilateral (radial side only) vs bilateral (radial and ulnar) application (depending on stability needs), ease of distraction/motion restriction control after application, and technical difficulty of application9,10.
While distraction is often implemented through the external fixator in order to reduce shear on the graft as it heals, it is not imperative as long as a concentric reduction is maintained4. Hinged internal fixation devices and non-distracting fixators are therefore also viable options with a stable reduction11.
Surgical Technique
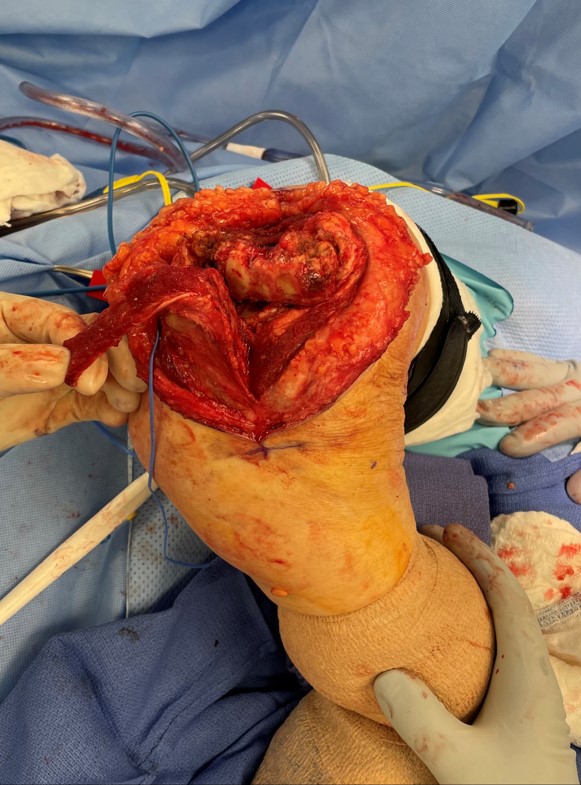
The following represents one common technique for performing this procedure and our preferred technique, however it is not meant to be inclusive of all variations and modifications. Additionally, it includes more recent modifications, such as the hinged internal fixator, which have not yet been formally researched in this particular procedure. Choice of approach is by surgeon preference but must allow extensive joint exposure4,5. Triceps splitting direct posterior approach, as depicted in Figure 2, is our preferred technique as it provides sufficient joint exposure with minimal collateral ligament disruption.

An extensive anterior and posterior capsulotomy is performed, maintaining the collaterals and common flexor and extensor mass muscle bellies if possible, with the option of an olecranon osteotomy for added exposure4,5. The ulnar and humeral joint surfaces are carefully prepared by denuding the cartilage and reshaping the trochlea as needed, as seen in Figure 3, leaving at least 3mm of joint gap for the interposition graft4,5,12. If painful or restricted preoperative pronation/supination was present, the ulnar articular margin for the radial head can be resected12.
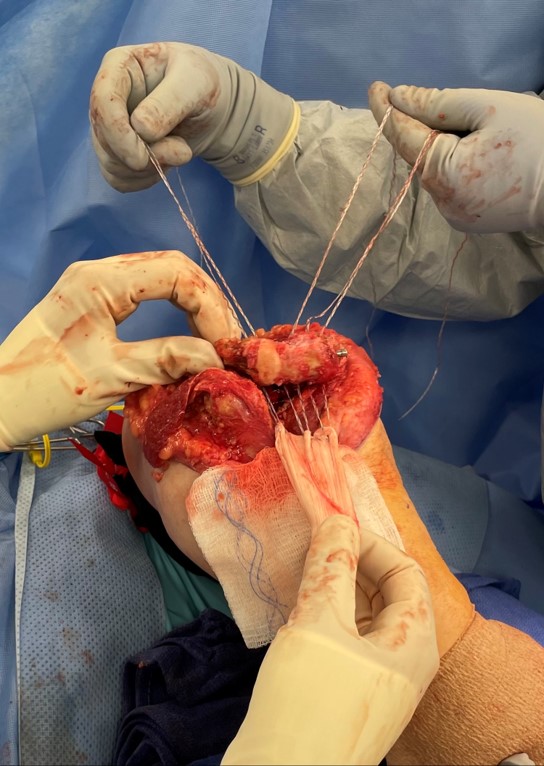
Once prepared, the graft of choice is wrapped tightly around the trochlea and fixed in place with non-absorbable sutures or suture buttons passed through three to four drill holes across the distal humerus from anterior to posterior, as seen in Figure 45. The joint is reduced and gently taken through its range of motion to assess for gliding, motion, impingement, and ligamentous integrity4.
Collateral ligament repair or reconstruction is not always necessary even if taken down, as they typically will scar back down as long as concentric post-operative reduction in maintained5. If electing to do so, however, this can be performed using the tails of the interposed graft, palmaris tendon, or the lateral triceps tendon4,5,13. If both collateral ligaments were sacrificed, a “sling reconstruction” can be performed by passing the graft through an ulnar bone tunnel 4. If the collaterals were maintained and the elbow is stable and concentric a fixator is not mandatory, though one can be utilized to ensure stability4.
The fixator is applied per its technique guide. Alignment of the fixator axis pin with the natural rotational axis is arguably the most important part of the case as this ensures a concentric reduction post-operatively9. This is found via fluoroscopy at the center of perfect overlapped circles of the trochlea and capitellum on the lateral view and parallel with the articular margin of the trochlea on a perfect AP view9. Optimal distraction allows for 3-5mm of congruent joint space, or until the graft no longer impinges in the joint4,4,5,13. Any reconstructed collateral ligaments are tensioned, and motion and stability are again assessed4. Figure 5 shows the final graft position and tension with a hinged internal fixator in place.

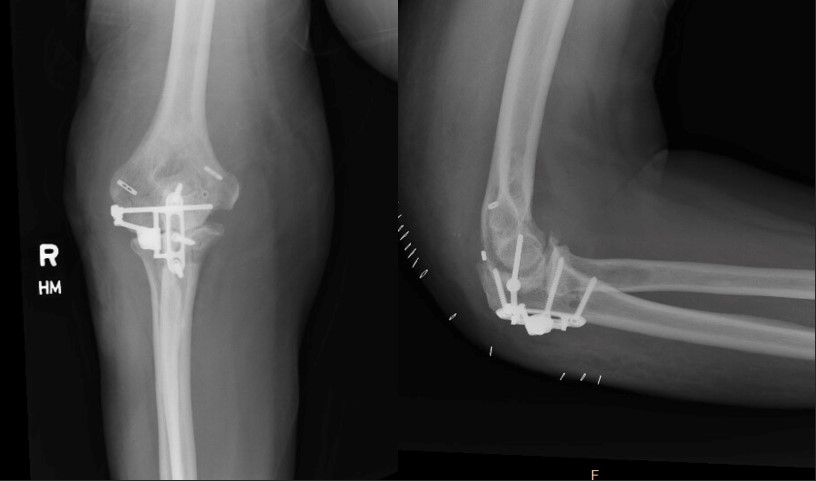
Muscular repair and ulnar nerve transposition is performed as necessary, and the skin is closed and dressing applied to allow for early postoperative motion4. Figure 6 shows radiographs of the final construct of the patient presented earlier in the paper, with suture buttons fixing the interposition graft in place on the distal humerus and a hinged internal fixator device in place to provide distraction across the joint space while the graft heals and incorporates.
Rehabilitation
A continuous passive motion (CPM) machine can be used with long, slow cycles to maintain maximal range of motion while minimizing wound issues, though its utility is debated in the literature4,5. Many of the older studies have demonstrated acceptable results in elbow rehabilitation with minimal risk, however most of these were lower-level studies and did not compare it to other rehab protocols14. Newer literature comparing CPM to physical therapy after arthroscopic elbow contracture release suggests that CPM may result in better overall motion and improved patient satisfaction, especially for those with the most significant motion limitations, however more research is needed to definitively recommend CPM use, and for the time being it should be used by patient and surgeon preference14. If opting for CPM use, this should be initiated as quickly as possible post-operatively to reduce swelling and achieve best results4,5,14.
Upon CPM cessation or if CPM is not utilized, active, active assisted, and passive range of motion should be initiated promptly and continued until the external fixator is removed around 4-6 weeks. If the elbow remains grossly unstable at the time of removal, the fixator can be left in place for another 3 weeks4,5,13. If an internal hinged fixator was used this can be left in place indefinitely unless hardware related complications necessitate removal, however it should be noted that the manufacturer recommendations are for removal at 6-8 weeks11. Once removed, activities are progressed as tolerated but part-time maintenance bracing is recommended for another 8-12 weeks4,5. Continued stiffness or regression of ROM can be addressed with periods of static splinting as needed4,5.
Outcomes
To our knowledge, no large high-level studies and few meta-analyses or systematic reviews exist on this procedure, so conclusions must be drawn from a number of smaller studies. Unfortunately, these vary widely in their indications, follow-up, techniques, and outcome measures, making it difficult to draw strong conclusions, however they do highlight the highly variable outcomes of the procedure. It should be noted that the following outcomes and complications data are drawn primarily from surgical techniques that include the use of an external fixator, and it is yet to be determined what impact the newer hinged internal fixator presented above will have on overall outcomes. Outcomes data regarding the use of this internal fixator in interposition arthroplasty has yet to be reported, however its use in other elbow instability cases has demonstrated at least equivocal outcomes to external fixators with decreased complication rates owing to its all-inside nature11.
Motion is one of the most important outcome measures for this surgery, and did improve across the board, with some studies showing a more impressive gain than others. In one study mean flexion/extension arc improved from 42 to 110°, flexion from 85 to 129°, flexion contracture from 44 to 20°, pronation from 43 to 72°, and supination from 43 to 70°15. In another, flexion/extension arc improved from 24 to 81° with all patients obtaining a functional level of >100° flexion, while flexion contracture improved from 74 to 38° and pronation/supination arc from 25 to 67°6. In nearly all of the studies reviewed post-operative flexion reached “functional” levels6,7,15.
When looking at secondary outcomes, graft survival rate averaged 79% at 5 years, and functional and satisfaction scores showed consistent improvement6,7,16. Reported post-operative MEPS scores averaged 69 points and DASH scores ranged from 19-316,7,15,16. Patient-reported satisfaction rates showed improvement, ranging from 67% to 83% satisfaction post-operatively7,12,15.
Complications
Cited complication and revision rates for this procedure are notably high, with revision rates averaging 21%16. The majority of complications are “minor”, however, and did not require a change in treatment course, and were most often related to the fixator and not the interposition4,17. These include superficial pin site or tract infections, neuropraxias, skin tension around the pin site, heterotopic bone formation, and seromas, and were seen in 23-46% of cases4,12,15,17. The more significant “major” complications, those which did require invasive intervention, were seen in 15-23% of cases and included triceps rupture, joint subluxation, deep tissue infections, and pin breakage or loosening4,12,15,17.
Of all the complications, however, instability was the most commonly cited and arguably the most important, as it has shown the largest overall impact on outcomes in surviving grafts18,15. Instability reporting and definitions are inconsistent across the literature but is reported in 10-70% of cases related to a number of different factors such as decreased bone stock, joint erosion for improper axis pin placement, or improper ligamentous or distraction balancing5,9,15,18. Regardless of the cause, preoperative instability has been well-established as the greatest predictor of postoperative instability5,7,12,18.
Fortunately, the high complication and revision rates do not seem to preclude successful future procedures. Even a failed interposition arthroplasty can be successfully revised to other procedures such as repeat interposition, arthrodesis, or total elbow arthroplasty with grossly equivalent outcomes as when these procedures are performed in the primary setting7,18.
Future Considerations
Though this procedure has been around for >150 years it has not evolved very far past its early days. As a result, it remains a procedure with narrow indications, unpredictable outcomes, and high complications, but in certain populations can be the last hope of regaining function. Advancements in technology can help us improve on this procedure and provide a better option for patients with a difficult problem and few other places to turn.
Improvements in joint axis determination is one of the major recent areas of advancement and has the possibility to improve graft longevity and overall outcomes. As mentioned previously, accurate axis pin placement is one of the most important portions of the case as this is what ensures a concentrically reduced joint which is critical to success5,9. The use of an intra-operative computerized navigation system has shown early success in improving the accuracy and reproducibility of determining the anatomic axis and placing the external fixator without the use of any x-ray fluoroscopy19. Similarly, a small cadaveric study found that a new custom 3D printed aiming guide for axis pin placement resulted in significantly less divergence between the normal joint axis and external fixator axis while reducing the number of fluoroscopic shots necessary for placement20. A new “auto-centering” external fixator that self-aligns with the axis of rotation without an axis pin has shown accurate axis and alignment maintenance without interfering with interposition fixation while simultaneously reducing complication rate and cutting down on procedural time21. These and other similar advancements show great promise in improving many aspects of this complex procedure and their use in interposition arthroplasty warrants further exploration and research.
Another modification which has been described more recently is the replacement of the external fixator with a new low-profile fully internal hinged fixator device, as was shown and described in the presented technique11. Owing to its all-inside nature, this device can be left in place for continued stability longer than external fixators, which could ultimately improve long-term stability even after removal11. Additionally, it is typically tolerated much better due to its significantly smaller profile compared to external fixators11. In a multicenter study of 24 patients, the device was effective in maintaining concentric reduction in 23 out of 24 elbows while maintaining functional motion22. At 6 month follow-up, mean flexion/extension arc was 119 degrees, mean pronosupination arc was 151 degrees, and functional outcome scores rated as good or excellent in all but 2 patients22.
It is clear that additional research in the form of larger prospective studies is needed to provide further clarity of outcomes and more accurate rates of complications in order to assist in individual risk/benefit analyses more appropriately. Studies utilizing the promising new technique and device enhancements outlined above would also be extremely beneficial in helping guide the future direction of the procedure. Cost of the primary procedure and its complications additionally need to be assessed and compared with longevity and functional/quality of life metrics to determine if there is truly value in this temporizing or bridge procedure.
Summary
Distraction interposition arthroplasty of the elbow can be a useful technique for decreasing pain and restoring function in younger (<60 years old), active patients with debilitating stiff, painful elbows secondary to end-stage arthritis in whom the restrictions or poor long-term survivorship of a total elbow arthroplasty are not acceptable18. With the lack of many better options for this population, this procedure continues to be utilized despite a high cited complication rate and level of technical difficulty6,1815. Though the objective functional scores are mediocre at best, it has shown high patient reported satisfaction rates and motion restoration7,12,15. Recent advancements in the technique of axis pin placement and the fixators themselves have shown early promise in making this procedure technically simpler, reducing complications rates, and improving stability, and could potentially expand its indications and success11,19,20,21. Strong efforts towards research into this procedure and its advancements need to be continued in order to provide a better solution to a very difficult issue.
References
- Hotchkiss RN. Treatment of the Stiff Elbow. In: Wolfe S, Pederson W, Kozin S, Cohen, M. Green’s Operative Hand Surgery. 7th ed. Elsevier; 2016. p 843-62.
- Chou, T. A., Ma, H., Wang, J., Tsai, S., Chen, C., Wu, P., & Chen, W. Total elbow arthroplasty in patients with rheumatoid arthritis: a systematic review and meta-analysis. Bone Joint J. 2020 Aug;102-B(8):967-80.
- Aldini NN, Angelini A, Pagani S, Bevoni R, Girolami M, Fini M. Past and present of interposition arthroplasties for joint repair with special tribute to the contribution by Vittorio Putti. Knee Surg Sports Traumatol Arthrosc. 2016;24:4005-4011.
- Morrey BF. Interposition Arthroplasty of the Elbow. In: Morrey B, Sanchez Sotelo J, Morrey M. Morrey’s the Elbow and its Disorders. 5th ed. Elsevier; 2017. p 1043-1053.
- Chen DD, Forsh DA, Hausman MR. Elbow Interposition Arthroplasty. Hand Clinics. 2011; 27(2):187–97.
- Ersen A, Demirhan M, Atalar AC, Salduz A, Tunali O. Stiff elbow: Distraction interposition arthroplasty with an Achilles tendon allograft: Long-term radiological and functional results. Acta Orthopaedica et Traumatologica Turcica. 2014;48(5):558–62.
- Larson AN, Morrey BF. Interposition arthroplasty with an achilles tendon allograft as a salvage procedure for the elbow. J Bone Joint Surg Am. 2008 Dec 1;90(12):2714–23.
- Studer A, Athwal GS. Rheumatoid Arthritis of the Elbow. Hand Clinics. 2011; 27(2):139–50.
- Chen NC, Julka A. Hinged external fixation of the elbow. Hand Clinics. 2010; 26(3):423–33.
- Morrey BF. Hinged External Fixators of the Elbow. In: Morrey B, Sanchez Sotelo J, Morrey M. Morrey’s the Elbow and its Disorders. 5th ed. Elsevier; 2017. p 471-479.
- Sochol KM, Andelman SM, Koehler SM, Hausman MR. Treatment of Traumatic Elbow Instability With an Internal Joint Stabilizer. J Hand Surg. 2019 Feb 1;44(2):161.e1-161.e7.
- Cheng SL, Morrey BF. Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br. 2000; 82(2):233-8.
- Bravo CJ, Shuler TE. Arthritis and Arthoplasty: The Hand, Wrist, and Elbow. 1st ed. Elsevier; 2010. Interposition Arthroplasty of the Elbow; p 279-88.
- O’Driscoll SW, Lievano JR, Morrey ME, et al. Prospective randomized trial of continuous passive motion versus physical therapy after arthroscopic release of elbow contracture. JBJS. 2022 Mar 2;104(5):430-440.
- Nolla J, Ring D, Lozano-Calderon S, Jupiter JB. Interposition arthroplasty of the elbow with hinged external fixation for post-traumatic arthritis. J Shoulder Elbow Surg. 2008 May;17(3):459–64.
- Lanzerath F, Hackl M, Pucher CJ, et al. Interposition arthroplasty for post-traumatic osteoarthritis of the elbow: a systematic review. International Orthopedics. 2022; 46:2603-2610.
- Cheung E v., O’Driscoll SW, Morrey BF. Complications of hinged external fixators of the elbow. J Shoulder Elbow Surg. 2008 May;17(3):447–53.
- Laubscher M, Vochteloo AJH, Smit AA, Vrettos BC, Roche SJL. A retrospective review of a series of interposition arthroplasties of the elbow. Shoulder and Elbow. 2014 Apr 1;6(2):129–33.
- Song J, Ding H, Han W, Wang J, Wang G. An X-ray-free method to accurately identify the elbow flexion-extension axis for the placement of a hinged external fixator. Int J CARS. 2017 Nov 3;13:375-387.
- Dos Santos A, Creze M, Begin M, Laemmel E, Assabah B, Soubeyrand M. Cadaveric assessment of a 3D-printed aiming device for implantation of a hinged elbow external fixator. Eur J Orthop Surg Traumatol. 2017;27:405-414.
- Bigazzi P, Biondi M, Corvi A, Pfanner S, Checcucci G, Ceruso M. A new autocentering hinged external fixator of the elbow: A device that stabilizes the elbow axis without use of the articular pin. J Shoulder Elbow Surg. 2015 Aug 1;24(8):1197–205.
- Orbay J, Ring D, Kachooei A, Santiago-Figueroa J, Bolano L, Pirela-Cruz M, Hausman M, Papandrea R. Multicenter trial of an internal joint stabilizer for the elbow. J Shoulder Elbow Surg. 2017 Jan;26(1):125-32.
