
Phillip Dunn, MS41; Michael Bagnoli, DO2; Micah Jones, DO3
1Edward Via College of Osteopathic Medicine, Blacksburg, VA
2University of Virginia, Charlottesville, VA
3Lewis Gale Medical Center, Salem, VA
DOI: 10.70709/rgj7pyq5g0
Abstract
Introduction
Carpal tunnel syndrome (CTS) is the most common upper extremity compressive neuropathy found in roughly 4% of the population. Furthermore, up to 60% of those cases are found to have bilateral symptoms. Amyloid accumulation can cause carpal tunnel syndrome, bilateral in most cases. CTS is one of the earliest manifestations of amyloidosis. Prompt recognition and early intervention are critical for improving patients’ given the insidious and progressive nature of this disease. There are published recommendations for testing patients with CTS for amyloidosis, but no current guidelines on how to follow these patients, especially if they have no other symptoms or pathology related to deposition of amyloid.
Case Presentation
We present a 59-year-old, right-hand-dominant male with severe, ongoing right-hand pain, numbness, tingling, and weakness. The patient had been diagnosed previously with CTS and has progressed through conservative management. An electromyography (EMG) study was obtained from a prior visit, which resulted in severe right carpal tunnel syndrome. He was scheduled for open carpal tunnel release of his right carpal ligament, and due to high clinical suspicion, tenosynovial biopsy was sent to test for amyloidosis, which was read as positive for amyloid. Post-operatively, he returned to the clinic for suture removal of his right hand and presented with similar carpal tunnel symptoms in his left hand. Currently, no other clinical symptoms of systemic amyloidosis are present. He was referred to hematology and cardiology for further management and workup of amyloidosis.
Discussion
Bilateral CTS is a common, red flag manifestation of amyloidosis and can predate overt cardiac manifestations of amyloidosis by several years. Once symptomatic of cardiac involvement, the prognosis is poor. This case aims to highlight the importance of early detection using pathological specimen biopsies of the carpal tunnel and the importance of appropriate specialist referral to screen for organ involvement.
Keywords: Carpal tunnel syndrome, bilateral, amyloidosis
Background
Carpal tunnel syndrome (CTS) is the most common upper extremity compressive neuropathy found in roughly 4% of the population (1). Carpal tunnel syndrome is due to compression of the median nerve under the flexor retinaculum at the wrist. CTS presents with numbness and tingling in the median nerve distribution, including the thumb, 1st finger, long finger, and the radial aspect of the ring finger. In severe cases, you may see atrophy of the thenar eminence and impaired opposition of the thumb. Current treatment regimens start conservatively with the use of a nighttime wrist brace, activity modification, and NSAIDs. If progression of symptoms occurs, effective treatments include full-time use of a wrist brace, steroid injections into the carpal tunnel to relieve pressure on the median nerve (2). If progression persists, one may elect for surgical release of the flexor retinaculum to relieve pressure on the median nerve.
In patients with carpal tunnel syndrome (CTS), bilateral symptoms are observed in up to 60% of cases (3). These symptoms may result from various systemic and structural factors. Fluid retention within the carpal tunnel, as seen in conditions such as pregnancy and hypothyroidism, can contribute to bilateral presentation (3). Anatomical variations, including a high division of the median nerve (bifid or trifid), a reversed or duplicated palmaris longus tendon, and a persistent median artery, may serve as space-occupying lesions, leading to compression of the median nerve. Autoimmune diseases, particularly rheumatoid arthritis, can also lead to bilateral CTS due to synovial inflammation affecting the joints and surrounding soft tissues of the carpal tunnel. Furthermore, intracarpal masses, such as tophaceous deposits in gout or organized hematomas in hemophilia, may contribute to bilateral nerve compression (6). Another important etiology is the deposition of misfolded amyloid proteins, most commonly transthyretin (TTR), which can lead to local edema and subsequent median nerve compression. Notably, a recent study reported that all positive amyloid biopsies obtained from the flexor retinaculum were associated with bilateral CTS symptoms (10).
Case Report
A 59-year-old right-handed male presents with severe, persistent right-hand pain that worsens throughout the day. He reports a new onset of nocturnal symptoms, including numbness and tingling. The patient has attempted to manage symptoms with a wrist brace at night and as needed during work hours. He is employed as a truck assembly worker, where he builds tractor-trailer trucks and operates a welding machine for extended periods, activities that exacerbate his symptoms. He denied any recent trauma, systemic symptoms, or any other relevant medical history.
Physical exam included positive Tinel’s, Durkan, and Phalen tests, all confirming the diagnosis of CTS. Electromyography (EMG) was performed to assess the severity of damage to the median nerve, which resulted in severe median nerve compression at the wrist level. Given the severity of symptoms and failure of conservative management, surgical intervention was pursued.
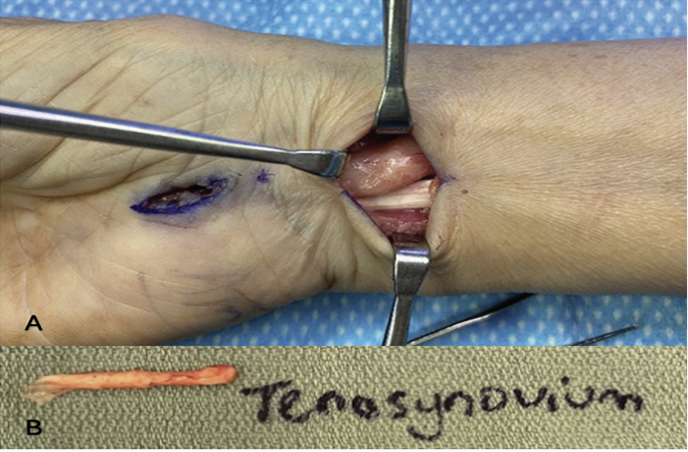
The patient underwent an open surgical release of the carpal tunnel, nine-tendon tenosynovectomy, and a hypothenar fat pad transfer. Intraoperatively, a biopsy of the tenosynovium was sent to pathology for amyloid testing, given the clinical suspicion raised by visualization of the synovium, as well as the patient’s male sex and age over 50 years (9) (Figure 1).
At his 2-week post-operative visit, he began experiencing similar symptoms in his contralateral hand. Repeat clinical testing, including a comprehensive physical examination, was performed, and a diagnosis of CTS was confirmed. Open surgical release was scheduled for the left hand.
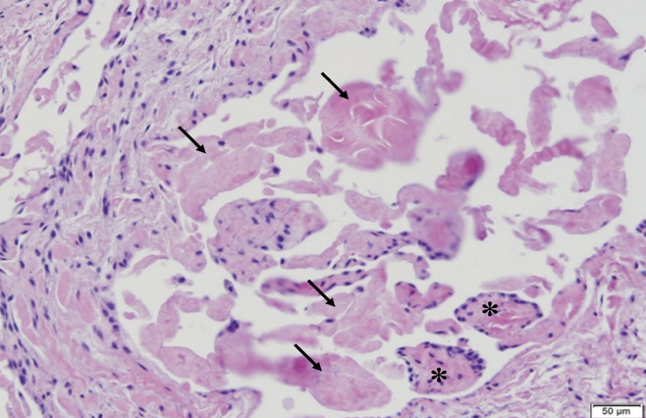
Pathological analysis of the tenosynovium was positive for amyloid deposition (Figure 2), and a referral was placed to cardiology for evaluation of cardiac involvement. Along with the cardiology referral, a complete blood count (CBC) and electrocardiogram (EKG) were ordered to screen for any systemic amyloid manifestations. Unfortunately, due to unrelated emerging medical concerns, the patient was unable to follow up with testing for amyloid evaluation and specialty referrals.
Discussion
Amyloidosis comprises a heterogeneous group of disorders characterized by the extracellular deposition of insoluble fibrillar proteins, ultimately leading to organ dysfunction. The two most common forms are light chain (AL) amyloidosis, caused by clonal plasma cells producing monoclonal light chains, and transthyretin (ATTR) amyloidosis, involving the deposition of wild-type or mutant transthyretin protein (10). Clinical manifestations vary widely depending on the organ system involved. Common presentations include nephrotic syndrome, heart failure with preserved ejection fraction (HFpEF), peripheral neuropathy, hepatomegaly, and gastrointestinal symptoms such as diarrhea, constipation, and unintentional weight loss (8). Cardiac involvement, in particular, is associated with markedly reduced survival. Early diagnosis and timely intervention, through chemotherapy, immunotherapy, and supportive care, are essential to improving patient outcomes (8). Although historically underdiagnosed, amyloidosis now has approved therapies that improve survival, reduce disability, and enhance quality of life.
CTS is increasingly recognized as one of the earliest clinical manifestations of amyloidosis, including both hereditary (ATTRv) and wild-type (senile systemic amyloidosis, SSA) forms (11,12). Research shows that both amyloid types manifest with symptoms before (particularly with ATTRv) cardiac manifestations of amyloid deposition by up to a decade. This delay in diagnosis contributes to the advanced cardiac disease often seen at the time of discovery, typically characterized by severe ventricular thickening, restrictive cardiomyopathy, and impaired systolic function (8,13). Given the insidious progression of amyloidosis, it is of utmost importance to recognize the early warning signs of amyloidosis, such as bilateral CTS, which is of paramount importance.
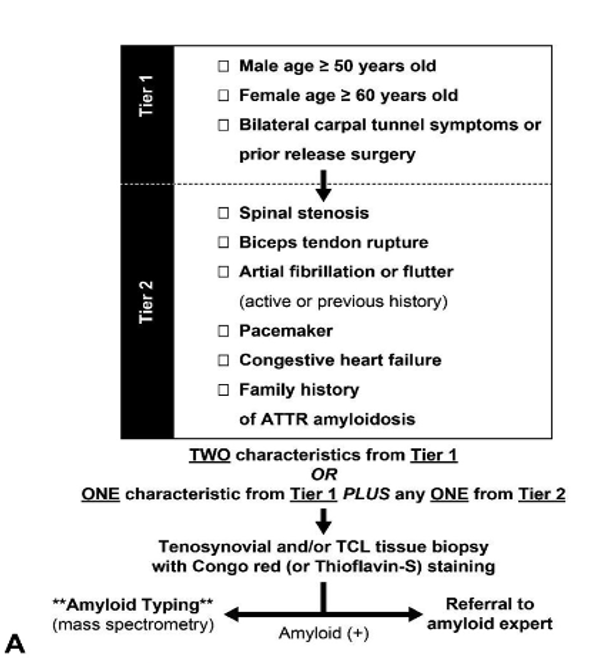
Despite published recommendations (Figure 3) for testing patients for amyloidosis, there are no current guidelines on how to manage or monitor these patients who test positive on biopsy but are not exhibiting symptoms. This presents a clinical challenge for orthopedic surgeons, particularly as early-stage amyloidosis is typically asymptomatic outside of CTS.
Recommendation
In the setting of a tenosynovial biopsy positive for amyloid following carpal tunnel release, contact the patient with their test result and make the test result available to their primary care provider and specialists already involved. With a positive result, we recommend a stratified approach. If the patient presents with any symptoms or comorbid conditions suggestive of systemic amyloid involvement, the corresponding organ system should be evaluated and considered for biopsy. In cases where the patient is asymptomatic apart from CTS, a baseline screening panel including laboratory tests, electrocardiogram, and echocardiogram should be performed to assess for subclinical organ involvement. Additionally, referrals should be made to hematology, oncology, and cardiology for any further specific workup and stratification based on the baseline testing results. If abnormalities are detected, further specialized workup is warranted. For patients with isolated CTS and no other findings, patients’ primary care providers should maintain a low threshold for future evaluation if new symptoms arise, as early detection remains key to improving long-term outcomes.
References
- Sharrak, S. Hand nerve compression syndromes. StatPearls [Internet]. (2023, August 8). https://www.ncbi.nlm.nih.gov/books/NBK547683/
- Piazzini DB, Aprile I, Ferrara PE, et al. A systematic review of conservative treatment of carpal tunnel syndrome. Clinical Rehabilitation. 2007;21(4):299-314. doi:10.1177/0269215507077294
- Szczecin, ul. Unii Lubelskiej. Bilateral Carpal Tunnel Syndrome – A Review. Department of General and Hand Surgery, Pomeranian Medical University in 1, 71-252 Szczecin, Poland. (2017, October 2). Neurologia i Neurochirurgia Polska.
- Elzinga, K. Amyloidosis and carpal tunnel syndrome: Surgical technique: Plastic and reconstructive surgery – global open. Amyloidosis and Carpal Tunnel Syndrome: Surgical Technique for Extended Carpal Tunnel Release with Tenosynovium and Transverse Carpal Ligament Biopsies. https://journals.lww.com/prsgo/fulltext/2023/01000/amyloidosis_and_carpal_tunnel_syndrome_surgical.54.aspx
- Fuller, John B., Kelly L. Scott, Moheb S. Moneim, Vann E. Schaffner. Case Report: Amyloid Deposits in the Flexor Tenosynovium Found During Primary Carpal Tunnel Release. Western Journal of Orthopaedics 11, 1 (2022).
- Dorwart, Bonnie Brice. Carpal tunnel syndrome: A review. Seminars in Arthritis and Rheumatism, Volume 14, Issue 2, 1984, Pages 134-140, ISSN 0049-0172. https://doi.org/10.1016/0049-0172(84)90003-9
- Pawel Dec, Andrzej Zyluk. Bilateral carpal tunnel syndrome – A review, Neurologia i Neurochirurgia Polska, Volume 52, Issue 1, 2018. Pages 79-83, ISSN 0028-3843. https://doi.org/10.1016/j.pjnns.2017.09.009.
- Gertz, Morie A, Dispenzieri, A. Jama. Systemic Amyloidosis Recognition, Prognosis, and Therapy: A Systematic Review. 2020;324(1):79-89.
- Carroll, G. J., Committee, A. Q. A., Girlanda, P., Kimura, J., & MacDonnell, R. A. L. (2003, August 14). Incidence of bilateral symptoms in carpal tunnel syndrome. The Journal of Hand Surgery: British & European Volume. https://www.sciencedirect.com/science/article/abs/pii/S0266768198800107
- Donnelly, J. P., Hanna, M., Sperry, B., & Seitz, W. (n.d.). Carpal tunnel syndrome: A potential early, red-flag sign of amyloidosis – sciencedirect. Carpal Tunnel Syndrome: A Potential Early, Red-Flag Sign of Amyloidosis. https://www.sciencedirect.com/science/article/abs/pii/S0363502319303843
- Ton, V, Patel, S, Gottlieb, S. Carpal Tunnel Syndrome and Future Amyloidosis: Time to Heed the Warning Sign. JACC. 2019 Jul, 74 (1) 24–25.https://doi.org/10.1016/j.jacc.2019.04.055
- Chafic Karam, Diana Dimitrova, Megan Christ, Stephen B. Heitner. Carpal tunnel syndrome and associated symptoms as first manifestation of hATTR amyloidosis. Journal Article 2019, Neurology Clinical Practice PG – 309-313 VI – 9 IP – 4
- Papoutsidakis, Nikolaos et al. Time Course of Common Clinical Manifestations in Patients with Transthyretin Cardiac Amyloidosis: Delay From Symptom Onset to Diagnosis. Journal of Cardiac Failure, Volume 24, Issue 2, 131 – 133
