
Rachael Larkin, BS, OMS-III1; Michael Bagnoli, DO1; Micah Jones, DO2
1Edward Via College of Osteopathic Medicine
2LewisGale HCA Medical Center
Abstract
A 61-year-old male presented with a left hamstring avulsion and an incidentally discovered gluteal mass on MRI. Surgical excision confirmed extraskeletal myxoid chondrosarcoma (EMC), managed with adjuvant radiation therapy. Serial imaging showed no recurrence or metastasis, though late wound complications required additional intervention. The patient remained free of recurrence or metastasis at 2.5 years postoperatively. This case underscores the importance of thorough imaging review and coordinated care. Recent large series highlight EMC’s indolent but persistent risk for recurrence, and demonstrate that chemotherapy has limited efficacy, emphasizing the need for aggressive local control and long-term management.
Keywords: Myxoid chondrosarcoma, soft tissue sarcoma, incidentaloma, hamstring avulsion, extraskeletal
Introduction
Extraskeletal myxoid chondrosarcoma (EMC) is a rare soft tissue sarcoma, comprising less than 3% of all soft tissue sarcomas, first described by Enzinger and Shiraki in 1972 (1,2). EMC typically arises in the deep soft tissues of the proximal extremities of adults, with a median age at diagnosis of approximately 50 years and a male predominance (3,4). Its hallmark is a unique chromosomal translocation, specifically in the EWSR1-NR4A3 fusion gene which distinguishes itself from other sarcomas (5,6). While EMC often follows an indolent clinical course, its propensity for local recurrence and distant metastasis, commonly to the lungs, necessitates vigilant long-term management (7-10).
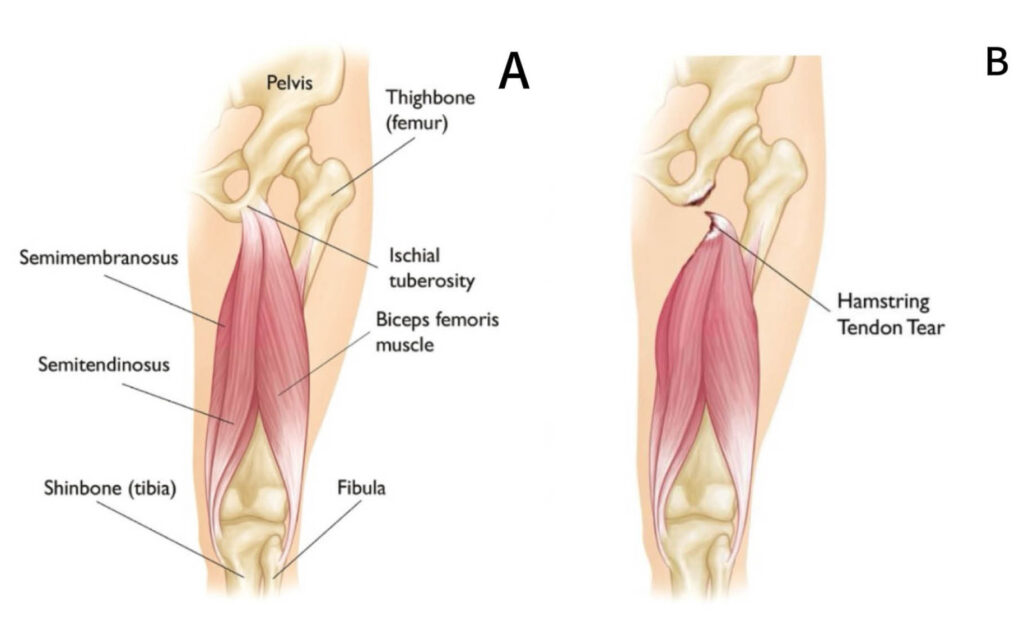
Understanding the anatomy of the proximal hamstring origin and the typical patterns of avulsion (11, Figure 1A-B) was essential for both surgical planning and interpretation of the imaging findings. Hamstring avulsions are common in sports injuries, typically involving proximal tendon origins at the ischial tuberosity, possibly pulling a piece of bone away as well (11). Surgical repair is indicated for complete tears with retraction to restore function and prevent chronic disability (11).
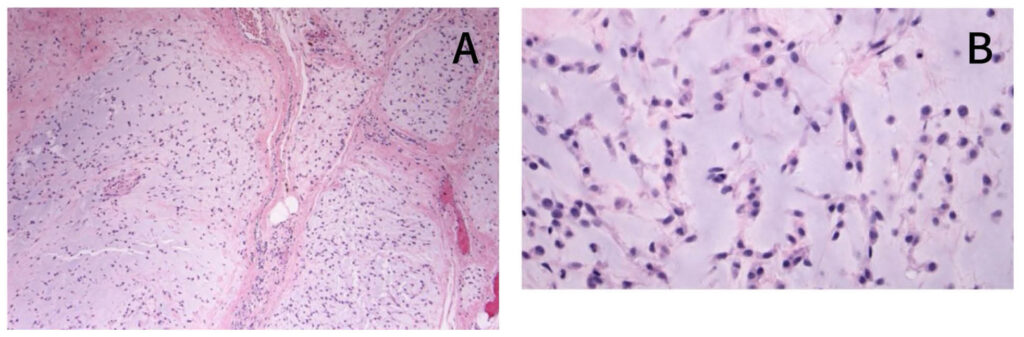
Ultimately, the diagnosis was confirmed by histological examination, which demonstrated the classic myxoid matrix and cord-like arrangement of tumor cells seen in EMC (12, Figure 2A-B).
This case highlights the multidisciplinary approach required for optimal management of rare sarcomas by integrating advanced imaging, anatomical correlation, and pathologic confirmation in the context of common musculoskeletal injuries.
Statement of Informed Consent
The patient was informed that data concerning this case would be submitted for publication and provided consent for the use of anonymized clinical information and imaging studies in this report. All identifying information has been removed to protect patient confidentiality.
Case Report
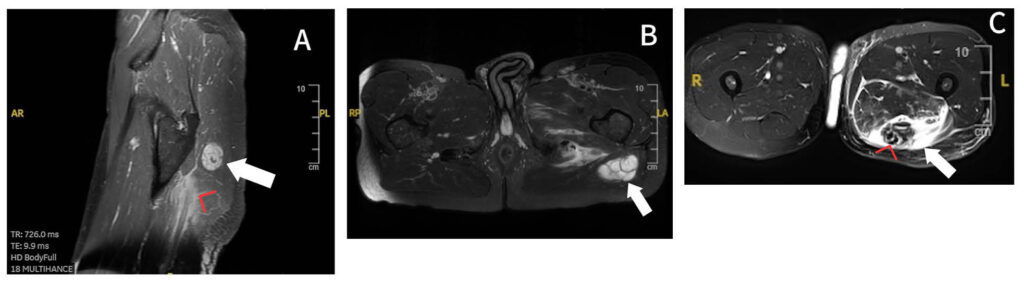
A 61-year-old male with no significant past medical history presented with acute left posterior thigh pain following participation in jet skiing. Physical examination revealed ecchymosis, tenderness over the ischial tuberosity, and a palpable defect consistent with hamstring avulsion. Preoperative MRI confirmed complete avulsion of the long head of the biceps femoris and semitendinosus tendons from the ischial tuberosity, with significant tendon retraction (Figure 3A). Incidentally, a well-circumscribed 10.5 x 3.3-centimeter mass was discovered within the left gluteus maximus muscle, distinct from the site of tendon injury. The mass exhibited internal septations, mild diffusion restriction, and diffuse enhancement post-contrast. Furthermore, there was a clear cleavage plane from the sciatic nerve with no surrounding edema or atrophy (Figure 3B, 3C).
Given the unexpected finding, the patient was referred to orthopedic oncology. After multidisciplinary discussion, the decision was made to proceed with surgical excision of the mass in conjunction with hamstring repair. The patient underwent successful resection of the gluteal mass and primary repair of the avulsed hamstring tendons.
Histopathological analysis revealed a malignant myxoid neoplasm measuring 9.2 cm with classic features of extraskeletal myxoid chondrosarcoma, grade 2 of 3, with NR4A3 rearrangement confirmed by fluorescence in situ hybridization (FISH). Margins were microscopically positive. The tumor was staged as T2N0.
Postoperative staging CT of the chest, abdomen, and pelvis showed no evidence of metastatic disease. The case was presented at a multidisciplinary tumor board, where adjuvant radiation therapy was recommended due to the positive margins and the risk of functional impairment with further resection.
The patient completed adjuvant radiation therapy to the surgical bed and was monitored with serial MRI and CT imaging. Initial recovery was excellent; by six months postoperatively, he had returned to cycling and running up to four miles. Follow-up imaging at 3, 6, and 12 months showed no evidence of local recurrence or metastasis, and the hamstring repair demonstrated expected healing.
At 2.5 years postoperatively, the patient developed new symptoms of pain and tightness in the left thigh and buttock. He reported a significant inflammatory response following a COVID-19 booster, with persistent wound drainage and a small area of wound dehiscence in the previously irradiated bed. He underwent surgical debridement and removal of retained suture material, followed by a course of doxycycline. Despite these interventions, a small area of persistent drainage remained, though there were no signs of systemic infection or tumor recurrence on imaging. The patient continued to be managed in collaboration with plastic surgery for consideration of rotational flap closure. At last follow-up 2.5 years postoperatively, he remained free of local recurrence or metastasis, with ongoing functional recovery and no evidence of disease progression.
Discussion
This case highlights several key aspects of EMC and the broader implications for musculoskeletal oncology. First, it underscores the importance of comprehensive imaging interpretation. While most soft tissue masses identified during imaging for trauma are benign, vigilance is warranted for atypical features, as the prevalence of unexpected malignant findings is low but clinically significant (1). EMC is often asymptomatic and discovered incidentally, as in this case, which aligns with its typically indolent presentation and tendency to reach large size before detection (3,7,13).
EMC is a rare entity with unique clinical and pathological features. The indolent nature of EMC often leads to delayed diagnosis, with tumors frequently reaching large sizes before detection (13,14). In this case, the tumor was asymptomatic and discovered only due to imaging for an unrelated injury. This underscores the need for a high index of suspicion and the value of multidisciplinary evaluation when unexpected masses are identified.
The management of EMC is challenging, particularly when resection margins are positive and further surgery risks significant morbidity. In this case, adjuvant radiation therapy was chosen to balance oncologic control with preservation of function, consistent with published guidelines (15). The patient’s excellent initial recovery and return to high-level activity demonstrate the potential for good functional outcomes with coordinated, multidisciplinary care (7). Despite the complex oncologic and functional challenges, personalized treatment strategies can achieve meaningful long-term quality of life without compromising disease control.
However, the case also illustrates the potential for late complications in previously irradiated and surgically treated tissues. The patient’s persistent wound drainage and inflammatory response, possibly exacerbated by immune activation following COVID-19 vaccination, required additional surgical intervention and prolonged wound care. Chronic wound complications are a known risk in irradiated fields, with rates reported as high as 20% in some series (8). Multidisciplinary collaboration, including plastic surgery, is essential for optimal management of such complications.
From an epidemiological perspective, the incidental discovery of a malignant tumor during workup for a tendon rupture is exceedingly rare. Hamstring avulsions are common in athletes and typically managed with surgical repair, while soft tissue sarcomas are rare, with an annual incidence of approximately 4–5 per 100,000 population (10). The likelihood of encountering both conditions concurrently is extremely low, highlighting the novelty of this case.
In summary, this case demonstrates the importance of thorough imaging review, multidisciplinary management, and long-term follow-up in patients with rare soft tissue sarcomas. It reinforces the need for vigilance in the evaluation of incidental findings and provides a framework for addressing the complex challenges posed by concurrent traumatic and oncologic pathology.
Conclusion
This case illustrates the diagnostic and management challenges of incidentally detected EMC. Early multidisciplinary intervention and strong local therapy are critical, as systemic chemotherapy offers minimal benefit. Vigilance in imaging review and individualized, long-term care are essential for optimizing outcomes in rare sarcomas.
References
- Fice MP, Lee L, Kottamasu P, et al. Extraskeletal myxoid chondrosarcoma: A case series and review of the literature. Rare Tumors. 2022;14:20363613221079754. Published 2022 Feb 25. doi:10.1177/20363613221079754.
- Enzinger FM, Shiraki M. Extraskeletal myxoid chondrosarcoma. An analysis of 34 cases. Hum Pathol. 1972;3(3):421-435. doi:10.1016/s0046-8177(72)80042-x.
- Drilon AD, Popat S, Bhuchar G, et al. Extraskeletal myxoid chondrosarcoma: a retrospective review from 2 referral centers emphasizing long-term outcomes with surgery and chemotherapy. Cancer. 2008;113(12):3364-3371. doi:10.1002/cncr.23978.
- WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours. WHO Classification of Tumours. 5th ed. Vol 3. Lyon, France: International Agency for Research on Cancer; 2020.
- Agaram NP, Zhang L, Sung YS, Singer S, Antonescu CR. Extraskeletal myxoid chondrosarcoma with non-EWSR1-NR4A3 variant fusions correlate with rhabdoid phenotype and high-grade morphology. Hum Pathol. 2014;45(5):1084-1091. doi:10.1016/j.humpath.2014.01.007.
- Chiusole B, Le Cesne A, Rastrelli M, et al. Extraskeletal Myxoid Chondrosarcoma: Clinical and Molecular Characteristics and Outcomes of Patients Treated at Two Institutions. Front Oncol. 2020;10:828. Published 2020 Jun 16. doi:10.3389/fonc.2020.00828.
- Brodsky CN, Bucala MD, Abdulfatah EM, Siegel GW. Extraskeletal Myxoid Chondrosarcoma: Retrospective Case Series Examining Prognostic Factors, Treatment Approaches, and Oncologic Outcomes. Am J Clin Oncol. 2023;46(4):172-177. doi:10.1097/COC.0000000000000988.
- O’Sullivan B, Davis AM, Turcotte R, et al. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial. Lancet. 2002;359(9325):2235-2241. doi:10.1016/S0140-6736(02)09292-9.
- Kransdorf MJ, Jelinek JS, Moser RP Jr. Imaging of soft tissue tumors. Radiol Clin North Am. 1993;31(2):359-372.
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48. doi:10.3322/caac.21763.
- American Academy of Orthopaedic Surgeons. Hamstring Muscle Injuries. OrthoInfo. https://orthoinfo.aaos.org/en/diseases–conditions/hamstring-muscle-injuries/. Published May 2025. Accessed June 2, 2025.
- Dong F, Jo V. Soft Tissues: Extraskeletal Myxoid Chondrosarcoma. Atlas Genet Cytogenet Oncol Haematol. March 1, 2017. http://atlasgeneticsoncology.org/solid-tumor/5025/soft-tissues-extraskeletal-myxoid-chondrosarcoma
- Meis-Kindblom JM, Bergh P, Gunterberg B, Kindblom LG. Extraskeletal myxoid chondrosarcoma: a reappraisal of its morphologic spectrum and prognostic factors based on 117 cases. Am J Surg Pathol. 1999;23(6):636-650. doi:10.1097/00000478-199906000-00002.
- Stacchiotti S, Baldi GG, Morosi C, Gronchi A, Maestro R. Extraskeletal Myxoid Chondrosarcoma: State of the Art and Current Research on Biology and Clinical Management. Cancers (Basel). 2020;12(9):2703. Published 2020 Sep 21. doi:10.3390/cancers12092703.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Soft Tissue Sarcoma. Version 2.2024.
