
Jonathan Tobin, OMS-IV; John Higgins, OMS-IV; Micah Jones, D.O.
Edward Via College of Osteopathic Medicine, Virginia Campus
DOI: 10.70709/x4oymciy7v
Abstract
Case
A 65-year-old right-hand dominant female presented with right-sided wrist pain after a fall one month prior. She had a history of left-sided carpal tunnel syndrome (CTS) treated with carpal tunnel release (CTR) and 9-tendon synovectomy one year earlier. Four weeks after a right-sided CTR, she sustained a right-sided hook of hamate fracture (HHF). Physical examination revealed tenderness over the hamate and pain with resisted flexion of the small and ring fingers. Radiographs confirmed a nondisplaced HHF, and CT imaging showed an acute/subacute fracture with cystic changes. Initially managed non-surgically, follow-up imaging revealed a nonunion, and she underwent surgical excision. Postoperatively, her pain significantly improved, with mild dysesthesia in the small finger.
Conclusion
This case suggests a potential link between CTR and subsequent HHF, possibly due to altered biomechanical forces. This observation highlights the need for further research on the long-term impact of CTR on carpal bone stability and fracture risk.
Keywords: Hook of Hamate, Carpal Tunnel, Fracture
Introduction
Hamate fractures are a relatively rare, but significant type of carpal bone fracture, accounting for approximately 5% of all carpal factures (1,2). These injuries typically occur in ball-and-stick sports such as baseball, golf, and tennis (3-5). Repetitive impact to the palm from the swinging motion of a racquet or club predisposes individuals to traumatic fractures of the hook of the hamate bone. The mechanism of injury for a HHF is classically understood to involve a sudden forceful impact to the palm, which causes the hook of the hamate to fracture, potentially leading to complications like non-union or malunion if not appropriately managed (6,7). While the clinical presentation and management of HHFs is well understood in the context of sport-related trauma, there is limited literature on fractures in patients who have recently undergone a CTR procedure. A CTR is a common surgical procedure that is used to treat CTS refractory to conservative treatment. While the complications associated with CTR operations are well studied, the potential for HHFs in the post-CTR population has received little attention despite the anatomical and biomechanical changes that may predispose the hamate bone to fracture.
This case report describes a unique presentation of a HHF following a fall in a patient with a prior history of CTR for CTS. To our knowledge, no cases have been reported in the literature that link HHF to a recent CTR, and few have explored the predisposing factors that could make patients who have undergone CTR more susceptible to HHF. The clinical significance of this case lies in its rarity and in the consideration that CTR, by altering the carpal anatomy and biomechanics, may act as a predisposing factor for subsequent fracture to the hook of the hamate bone.
Statement of Informed Consent
The patient was informed that data concerning the case would be submitted for publication and provided consent.
Case Report
A 65-year-old right-hand dominant female presented to the orthopedic clinic with right-sided wrist pain following a fall in the bathroom one month prior. She reported breaking her fall with her right hand. Her past surgical history included left-sided CTR one year earlier. At presentation, she was four weeks post-op from right CTR. The patient is a non-smoker and is on vitamin D supplementation. Upon arrival, the patient was afebrile, with a blood pressure of 133/87 mmHg, a heart rate of 89 bpm, and a body mass index of 28. On physical examination, she demonstrated a right-sided, well-healed, carpal tunnel scar. Tenderness was noted over the hook of the hamate, and increased pain was elicited with resisted flexion of the small and ring fingers during ulnar deviation, consistent with pressure on the hook of the hamate. Sensation was intact in the small and ring fingers, and flexion/extension were also intact. There were no signs of infection, and no pain was noted in the remainder of the hand, wrist, or digits. The axillary, musculocutaneous, radial, and ulnar nerves were grossly intact, and sensory function was preserved.
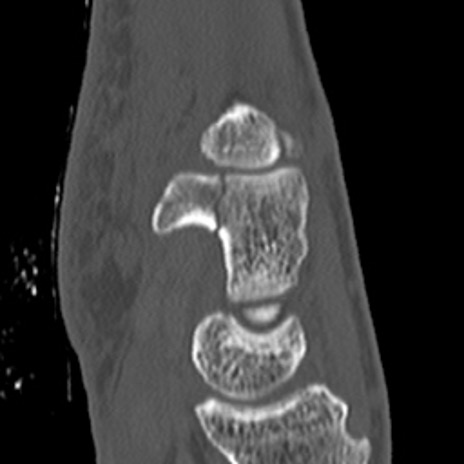
Hand and wrist radiographs were obtained, which demonstrated a nondisplaced HHF fracture on the carpal tunnel view. Mild osteopenia was noted, but no arthritic changes were observed in the hand or wrist joints. There were no other acute findings. Given the patient’s recent CTR and the subtle nature of the HHF, a CT scan was performed to further characterize the fracture. The CT scan revealed a nondisplaced acute/subacute irregular fracture through the base of the hook of hamate, with small 3mm cysts on both sides of the fracture line involving the body of the hamate. No significant new bone formation was observed, and there was some scarring and infiltration from the skin line to the flexor retinaculum of the carpal tunnel.
Surgical excision of the hook of hamate was discussed in detail with the patient, and a shared decision-making approach led her to opt for initial nonsurgical management. She was informed that nonsurgical management could take up to three months and carried a risk of nonunion or malunion. She was provided with an ulnar gutter brace for support. At 6 weeks follow-up, the patient continued to experience pain, and radiographs revealed a nonunion of the hook of hamate fracture. She elected for surgical excision of the nonunion, which was performed. Two weeks post-operatively, the patient reported significant improvement in her pain. She continued to experience occasional dysesthesia in the small finger but was able to perform gentle range of motion exercises for her hand and wrist.
Discussion
Fractures of the hook of the hamate are uncommon but clinically significant carpal bone fractures. These fractures are typically reported in athletes involved in ball-and-stick sports such as baseball and golf. Common presenting symptoms of HHFs include wrist pain, tenderness over the hook and body of the hamate, and pain elicited with specific maneuvers, such as the hamate pull test (9).
In general, HHFs represent a small proportion of carpal bone fractures, though their incidence may be underreported due to their subtle clinical presentation and often occult nature on standard radiographs (10). The mechanism of injury for HHFs is classically understood to be related to direct trauma from high-impact forces, such as those generated from striking a ball with a bat or club. However, recent literature highlights a chronic etiology for these fractures, where high-tensile gripping activities, exerting pressure on the hook of the hamate through tension in the adjacent deep flexor tendons, mechanically weaken the bone over time (3,4). This chronic overuse predisposes leads to fractures even in the absence of acute trauma, particularly in those who perform repetitive gripping motions such as rock climbers and bowlers (11,12). Recognizing the acute versus chronic mechanism of injury in HHFs may not directly influence treatment but can provide useful clinical context for explaining the injury to patients and guiding post-injury activity modifications. The proportion of acute versus chronic mechanisms in HHFs remains incompletely understood in the literature, considering previously described acutely traumatic events may represent a most recent manifestation of a prolonged chronic injury.
Anatomically, the hook of the hamate serves as an attachment point for a number of both static and dynamic structures. The flexor retinaculum spans the volar wrist, attaching ulnarly to the pisiform and hook of the hamate, and radially to the scaphoid tubercle and trapezial ridge, forming the roof of the carpal tunnel (13). The flexor digiti minimi brevis and opponens digiti minimi originate, in part, from the hook of the hamate and course distally toward the hypothenar region. Additionally, the flexor carpi ulnaris partially inserts into the hook. The hook itself contributes to the ulnar border of the carpal tunnel and lies adjacent to the fourth and fifth flexor digitorum profundus tendons as they exit the tunnel.
In the present case, the patient’s history of recent CTR and tendon synovectomy raised concerns regarding how these surgical interventions might have affected the biomechanical environment of the wrist and hand. Disruption of the transverse carpal ligament and its attachments to the hook may contribute to a destabilized carpal environment leading to postoperative wrist pain, commonly referred to as pillar pain. Pillar pain is a frequently reported complication after CTR, characterized by diffuse aching in the thenar and hypothenar regions (17,18). While its etiology is considered multifactorial, including contributions from neurogenic irritation and scar tissue formation, altered carpal biomechanics have been cited as a plausible contributor (17). In this context, the hook of the hamate can act as a biomechanical liability following CTR by contributing to postoperative discomfort.
To our knowledge, no prior studies have directly established an increased vulnerability of the hook of the hamate following CTR. Several investigations have demonstrated that the transverse carpal ligament plays a significant role in maintaining carpal stability (15,16). Release of this ligament during CTR results in measurable changes to carpal tunnel architecture, including increased tunnel volume, widened carpal arch, and altered musculotendinous dynamics (17). These biomechanical shifts may not independently cause injury but could render the hook more susceptible to trauma in the setting of an acute event, such as a fall, or contribute to injury through the recently described chronic mechanism (3).
A predisposing alteration in carpal tunnel anatomy, such as a CTR, certainly affects the native stability of the hook due to the disruption of its ligamentous attachments. Such a risk factor could leave the hook vulnerable to forces in an acutely traumatic event or chronic tension-induced fractures. However, in the absence of consistent evidence linking CTR to carpal fractures, it remains equally plausible that an open carpal tunnel could reduce the likelihood of a HHF by relieving chronic tension, and that this patient’s injury resulted primarily from the acute traumatic mechanism rather than any surgically induced predisposition.
This case highlights a rare but clinically relevant presentation of a hook of hamate fracture following recent carpal tunnel release. While the injury likely resulted from acute trauma, the potential role of altered carpal biomechanics post-CTR warrants consideration, particularly in patients with additional risk factors. Further research is needed to clarify whether post-CTR anatomical changes meaningfully increase susceptibility to carpal fractures.
References
- Zander MEL, Swärd E, Björkman A, Wilcke M. Carpal fractures: epidemiology, classification and treatment of 6542 fractures from the Swedish Fracture Registry. J Hand Surg Eur Vol. 2024;49(4):470-476. doi:10.1177/17531934231202012
- Dennis HHW, Sze ACK, Murphy D. Prevalence of Carpal Fracture in Singapore. The Journal of Hand Surgery. 2011;36(2):278-283. doi:10.1016/j.jhsa.2010.11.009
- Suzuki A, Kanda T. Understanding the Injury Mechanism in Hamate Hook Fractures by Investigating Fracture Morphologies: A Case Series Study. Hand (N Y). Published online February 29, 2024:15589447241232096. doi:10.1177/15589447241232096
- Campbell FC, Jones SW, Campbell DA. The aetiology of fracture and nonunion in the hook of the hamate. J Hand Surg Eur Vol. 2024;49(9):1172-1178. doi:10.1177/17531934241235803
- Bachoura A, Wroblewski A, Jacoby SM, Osterman AL, Culp RW. Hook of Hamate Fractures in Competitive Baseball Players. Hand (New York, N,Y). 2013;8(3):302-307. doi:10.1007/s11552-013-9527-4
- Ta CN, Finley Z, Medvedev GA. Complications after Nonoperative Management of Hamate Fractures. Plast Reconstr Surg Glob Open. 2022;10(5):e4352. doi:10.1097/GOX.0000000000004352
- Donohue JK, Calcaterra MJ, Fowler JR. Surgical Management of Hook of Hamate Fractures: A Systematic Review of Outcomes. J Hand Surg Glob Online. 2023;6(2):183-187. doi:10.1016/j.jhsg.2023.11.011
- Knipe H. Hook of hamate fracture | Radiology Reference Article | Radiopaedia.org. Radiopaedia. doi:10.53347/rID-49117
- Wright TW, Moser MW, Sahajpal DT. Hook of Hamate Pull Test. The Journal of Hand Surgery. 2010;35(11):1887-1889. doi:10.1016/j.jhsa.2010.08.024
- Welling RD, Jacobson JA, Jamadar DA, Chong S, Caoili EM, Jebson PJL. MDCT and Radiography of Wrist Fractures: Radiographic Sensitivity and Fracture Patterns. American Journal of Roentgenology. 2008;190(1):10-16. doi:10.2214/AJR.07.2699
- How Kit N, Malherbe M, Hulet C. Hamate hook stress fracture in a professional bowler: Case report of an unusual causal sport. Hand Surgery and Rehabilitation. 2017;36(1):62-65. doi:10.1016/j.hansur.2016.06.007
- Lutter C, Schweizer A, Hochholzer T, Bayer T, Schöffl V. Pulling Harder than the Hamate Tolerates: Evaluation of Hamate Injuries in Rock Climbing and Bouldering. Wilderness & Environmental Medicine. 2016;27(4):492-499. doi:10.1016/j.wem.2016.09.003
- Li ZM, Marquardt T, Evans P, Seitz W. Biomechanical Role of the Transverse Carpal Ligament in Carpal Tunnel Compliance. Jnl Wrist Surg. 2014;03(04):227-232. doi:10.1055/s-0034-1394136
- Ulnar approach to the hamate hook. Accessed May 10, 2025. https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/carpal-bones/approach/ulnar-approach-to-the-hamate-hook
- Kimura H, Sato K, Matsumura N, et al. Evaluation of Dynamic Carpal Arch Stability following Carpal Tunnel Release Using Four-Dimensional Computed Tomography. Journal of Hand and Microsurgery. 2021;13(3):138-142. doi:10.1055/s-0040-1718969
- Ratnaparkhi R, Xiu K, Guo X, Li ZM. Changes in carpal tunnel compliance with incremental flexor retinaculum release. J Orthop Surg Res. 2016;11:43. doi:10.1186/s13018-016-0380-3
- Brooks JJ, Schiller JR, Allen SD, Akelman E. Biomechanical and anatomical consequences of carpal tunnel release. Clinical Biomechanics. 2003;18(8):685-693. doi:10.1016/S0268-0033(03)00052-4
- Boya H, Özcan Ö, Özteki̇n HH. Long‐term complications of open carpal tunnel release. Muscle and Nerve. 2008;38(5):1443-1446. doi:10.1002/mus.21068
