
William Littlefield, DO, UPMC; Shaan Sadhwani, DO; Jamie Henzes, DO; Brendan Sweeney, DO; Matthew Kendall, DO; Brian Omslaer, DO; Scott King, MD
UPMC
DOI: http://doi.org/10.70709/1anpaj6mz5
Abstract
Background
Outpatient total joint arthroplasty has been at the forefront of orthopedic surgery. While there have been many publications regarding outpatient total joint arthroplasty in large academic settings, large-volume studies examining outcomes in community settings are lacking. This investigation reports a community institution’s experience in implementing same-day total hip arthroplasty (THA), total knee arthroplasty (TKA) and factors influencing failure to complete same-day discharge.
Methods
A retrospective chart review of patients scheduled for same-day THA and TKA across 7 community hospitals within a single institution from December 2021 to September 2023 was performed. Patients were given the same-day discharge designation based on a pre-established institutional protocol. The primary outcome was the successful completion of the same-day discharge. Secondary outcomes included factors associated with failure to discharge on the day of surgery. Multivariate regression analysis was used to investigate several of these factors.
Results
688 patients were included of which 434 underwent TKA, 254 underwent THA. 113 in the TKA group and 70 in the THA group failed to discharge on the same calendar day and were admitted for an overnight stay. Overall, poor ambulation (< 105ft) with physical therapy in the post-operative unit was the most important determinate of failed discharge (OR 5.61, 95% CI 3.63-8.65, p=<.0001). In TKA, patients who received peripheral nerve blocks were significantly more likely to successfully discharge (OR 0.49, 95% CI 0.27-0.88, p=0.0170).
Conclusions
At this institution, peripheral nerve blocks resulted in higher successful discharges. The single most important factor regarding successful discharge at this institution, also demonstrated by many others, seemed to be ambulation in the post-operative unit, which is in congruity with a pre-established institutional protocol of 75 feet of minimal ambulation distance. Therefore, perioperative decision making should focus on factors that will enable patients to be most successful with physical therapy.
Keywords: Outpatient, Total Hip, Total Knee, Same-Day, Arthroplasty
Introduction
Same-day total joint arthroplasty (TJA) has seen tremendous growth in recent years. Factors influencing this paradigm shift have included improvements in surgical techniques, preoperative optimization, recovery protocols, and the removal of TJA from the Medicare inpatient only list.1 Many prior studies have shown outpatient total hip arthroplasty (THA) and total knee arthroplasty (TKA) to be safe, cost-effective and have similar complication rates with low admission rates when compared to inpatient arthroplasty.1-3 Given the opportunity to decrease healthcare costs and improve patient outcomes without increasing adverse outcomes, same-day arthroplasty is expected to continue to gain popularity over traditional overnight hospital stays.
Various protocols have been utilized for rapid recovery, enabling same-day discharges that have improved recovery rates without increasing adverse events. These protocols often include use of spinal anesthetics, decreasing intrathecal narcotics, and initiation of early post-operative physical therapy.2,4,5 Furthermore, patient selection remains a crucial aspect in ensuring successful same-day discharge. Identifying medical conditions that may require additional perioperative care or social issues that may be detrimental to the patient discharging to their home after their TJA is paramount to ensuring optimal patient outcomes and safety.1
While factors influencing same day TJA have been examined in the literature, many of these reports are in small volumes of patients in large academic centers. In turn, there is a paucity of data reporting larger volume experiences in the community setting. Therefore, the purpose of this study was to report the experience of our community institution in regard to successful same-day THA and TKA, termed as the ability to leave prior to midnight on the day of surgery. In doing so, we aimed to report factors that influenced the failure of same-day discharge and subsequent admission in an effort to find areas of optimization.
Methods
A retrospective chart review of patients scheduled for same-day THA and TKA across seven community hospitals within a single institution from December 2021 to September 2023 was performed. Patients were designated for same-day discharge prior to their presentation to the hospital for their arthroplasty based on a pre-established institutional protocol implemented by scheduling staff consistently across all seven hospitals. To be eligible for same-day designation across the institution, patients had to meet the following criteria: have a support caregiver at home, no active smoking >1 pack per day, no active heavy alcohol or illicit drug use, and no high-risk medical comorbidities. These include chronic obstructive pulmonary disease, uncontrolled diabetes, chronic opioid use, chronic kidney disease, neurologic conditions with severe immobility, dementia, delirium, or cardiovascular disease including recent angina, myocardial infarction, or chronic heart failure. Surgeries were performed by fellowship and non-fellowship trained surgeons, with most patients undergoing a medial parapatellar approach for TKA. Patients were allowed to discharge the same calendar day if they cleared physical therapy protocols (PACU ambulation >100 ft), pain was controlled, and they did not have a medical issue precluding them from discharge (nausea, vomiting, urinary retention, hypotension). Patients were excluded if the case was bilateral arthroplasties, any revision procedures, and patients who had to undergo hardware removal to perform their THA or TKA. Institutional review board approval was obtained for this retrospective chart review.
Medical records were reviewed to collect pre-operative, operative, and post-operative data. Pre-operative data included age, gender, body mass index (BMI), diabetes history, chronic kidney disease history, pre-operative anemia, prior arthroplasty history, smoking history, American Society of Anesthesiologists (ASA) score, pre-operative ambulatory status and Charleston Comorbidity Index (CCI). Operative data included operative time (incision to skin closure), anesthesia type, approach, block percentage and type, tourniquet inflation time, pressure, and size. Post-operative data included ambulation with physical therapy (PT) in the post-anesthesia care unit (PACU) on the day of surgery. Approach, cement use, robotic use, as well as peripheral nerve block (adductor canal) utilization, was based on surgeon preference. . For the patients who failed same day discharge, reason for failure, length of stay and ambulation with physical therapy on the subsequent post-operative days were recorded. For failure to discharge or readmission, reason criteria included failed physical therapy, medical issue (nausea, vomiting, hypotension), numbness, pain control, wound concern, and other. “Other” included all patients who did not fall into the aforementioned categories. The primary outcome measured was failure to complete the same day discharge designation (discharge on the same calendar day).
Multiple statistical methods were used to evaluate the data. Normality tests for continuous variables were performed using the Shapiro–Wilk test. Variables with a normal distribution were displayed as mean ± standard deviation and range and were compared using independent samples t-tests. Non-normally distributed data are presented as median (interquartile range) and were compared using the Wilcoxon two-sample test. Categorical variables, expressed as percentages, were compared using the chi-square test or Fisher’s exact test, as appropriate. Multiple logistic regression models were used to identify significant predictors of the outcome, with odds ratios and 95% confidence intervals reported. Statistical significance was considered if P < 0.05. All statistical analyses were performed using SAS Version 9.4 (SAS Institute, Cary, NC).
Results
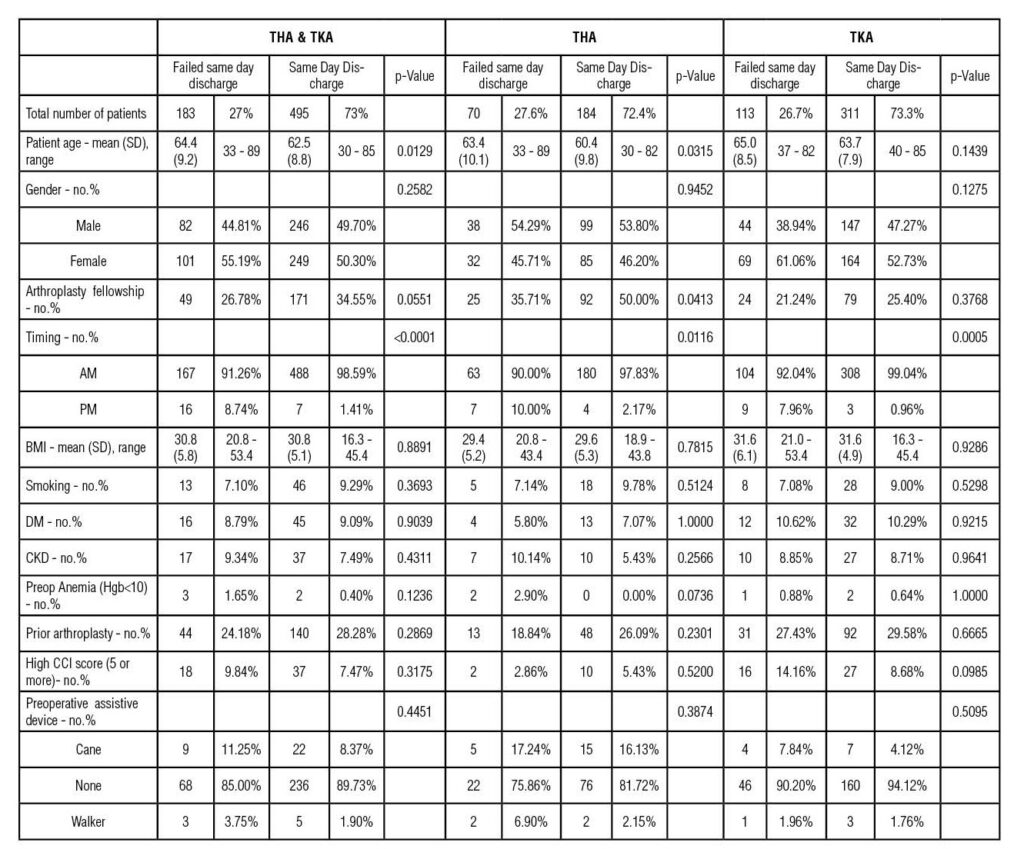
Legend: SD, standard deviation; BMI, body mass index; DM, diabetes mellitus; CKD, chronic kidney disease; CCI, Charleston Comorbidity Index.
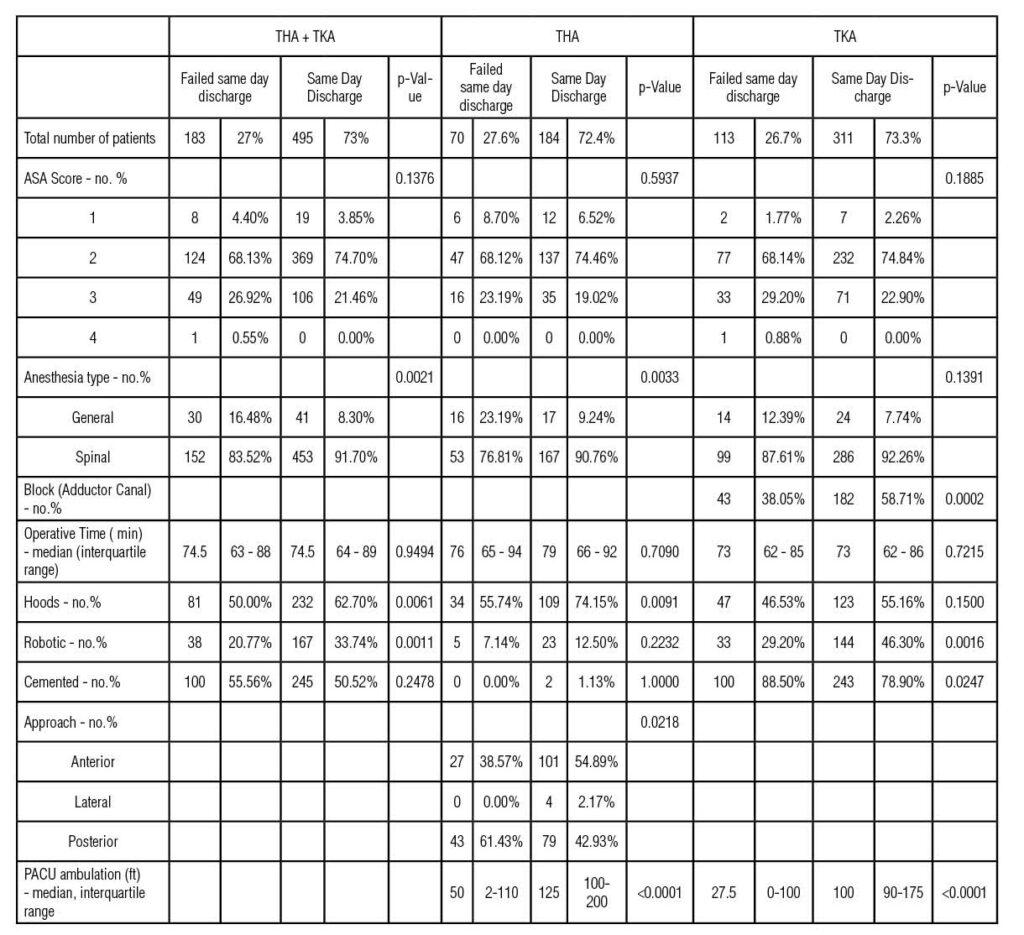
Legend: ASA, American Society of Anesthesiologists; Min, minutes; PACU, post-anesthesia care unit
Demographic data between the successful same day (SSD) and failed same day (FSD) discharge groups was similar in terms of BMI, smoking status, CCI, preoperative ambulatory status, diabetes history, and CKD history were similar in the overall and THA or TKA specific analysis (Table 1). There was also no statistically significant difference in ASA score or operative times in the SSD and FSD groups (Table 2). Interestingly, in patients undergoing THA, the FSD group had patients of higher age (mean 63.4 vs 60.4, p=0.315) and had more of their procedures done by a non-fellowship trained surgeon (Table 2).
Interestingly, significantly more patients in the SSD group overall received spinal anesthesia (91.70% vs 83.52%, p=0.0021) (Table 2). When examining THA and TKA alone, this trend was maintained, however only THA continued to have a significantly higher proportion of patients who received spinal anesthesia in the SSD group when compared to the FSD group (90.76% vs. 76.81%, p=0.0033) (Table 2). Significantly more patients in the SSD TKA group received an adductor canal block prior to surgery (58.71% vs. 38.05%, p=0.0022). Interestingly, more SSD patients who underwent TKA had the use of robotics in their procedure (Table 2). In terms of patients who underwent THA, there was a significantly higher proportion who underwent anterior THA in the SSD group (Table 2).
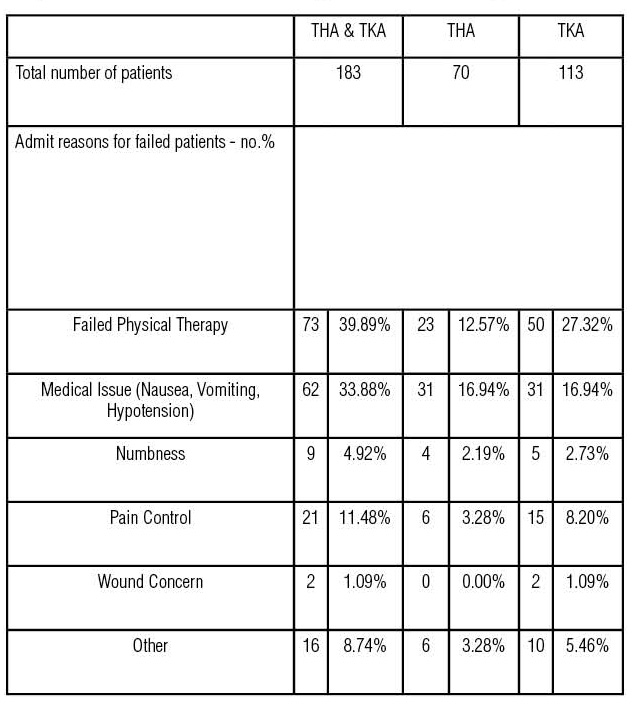
In terms of the FSD patients, the majority were admitted after failing to be cleared by physical therapy (38.25%), with the next most common reason being a medical issue (33.33%) (Table 3). This was consistent among the overall, THA, and TKA groups (Table 3). In the TKA patients, ambulation in the post-anesthesia care unit (PACU) on the day of surgery was significantly longer in feet in the SSD group (100ft vs. 27.5ft, p<0.0001) (Table 2). In the THA patients, PACU ambulation on the day of surgery was also significantly longer in feet ambulated in the SSD group (125ft vs. 50 ft., p<0.001) (Table 2). 89.20% of patients in the overall group were admitted for a length of stay of 1 day, and the median feet ambulated with physical therapy on post-operative day 1 was 200ft.
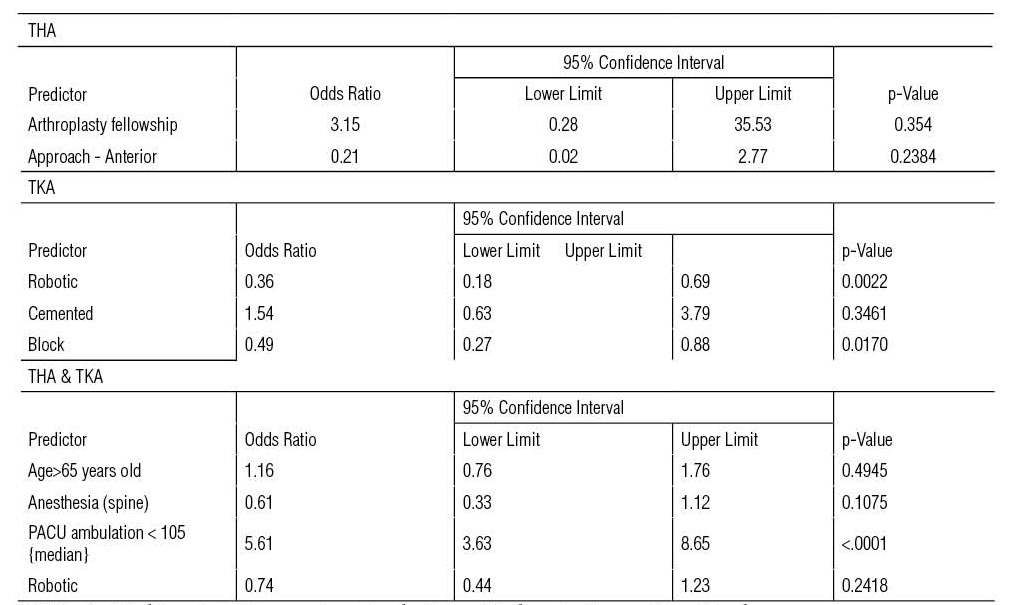
Upon multivariate regression analysis examining for overall risk factors amongst THA and TKA, chosen by the statistician based on bivariate analysis, PACU ambulation <105ft was seen to be the only statistically significant predictor of FSD (Table 4)(Figure 5). Multivariate regression analysis examining for potential risk factors for failing same-day discharge designation, in THA, patients ambulating less than 100ft in PACU had a significantly higher likelihood of failing their same-day designation (OR 26.61, 95% CI 9.48-74.73, p<0.001) (Table 4). In terms of approach used, the data suggests that an anterior approach trends toward an increased likelihood of successful same day discharge, however this did not reach statistical significance (OR 0.21, 95% CI 0.02-2.77, p=0.2384)(Table 4). Patients undergoing spinal anesthetic for THA also carried an increased likelihood of successful same day discharge, however this as well did not reach statistical significance (OR 0.54, 95% CI 0.18-1.62, p=0.2685) (Table 4). Multivariate regression analysis examining potential risk factors for failing same-day discharge designation in TKA revealed receiving a peripheral nerve block post-operatively was associated with a significantly decreased likelihood of failing (OR 0.49, 95% CI 0.27-0.88, p=0.0170) (Table 4) Additionally, patients who ambulated less than 100 feet in the PACU had a significantly higher likelihood of failing their same-day designation (OR 12.78, 95% CI 7.03-23.24, p<0.0001) (Table 4).
Discussion
In the present study, we found a successful overall same-day discharge rate of 73% (with a 72.4% success rate in THA and a 73.3% success rate in TKA (Table 1). When examining the other institutional experiences currently available for review, there seems to be a wide range of successful same day discharge rates reported. These reports are further confounded by location and by the definition of same-day discharge as on the same calendar day, or within 24 hours of surgery. In the current investigation, all cases were performed at an inpatient hospital and successful same-day discharge was defined as discharge on the same calendar day. The successful same day discharge rate in the current literature can range from 51.1% as reported by Shen et al to 85.3% as reported by Gong et al.6-8 It is important to note when comparing this investigation to existing literature, since cases included were performed at inpatient hospitals, rather than an ambulatory surgery center, this inherently creates an easier pathway for patients to convert to an inpatient status. In turn, this may increase the number of patients that failed same-day discharge given the accessibility of the hospital resources not found at an ambulatory surgery center. Interestingly, Lutz et al performed a recent retrospective analysis comparing outpatient THA and TKA done in the hospital setting versus at an ambulatory surgery center (ASC).2 In their analysis, they found no failures in the ASC setting while they reported a 65.6% failure rate of TKA and 34.5% failure rate of THA to discharge on the same day from the hospital setting.2 These findings further support the notion that the failure rate seen in the current study may be influenced by the nature of outpatient procedures performed in the hospital setting secondary to resources and pathways available for admission. Therefore, optimization of successful discharge may have a larger basis on location than previously thought.
Current investigations in same-day arthroplasty regarding reasons for failure to discharge have shown similarities in the most common culprits. While not all inclusive, the most often cited common reasons for failure to discharge after total joint arthroplasty are: patient preference, failure to clear physical therapy, dizziness/hypotension, urinary retention, and nausea/vomiting, and pain control.6-8 These common characters are echoed by this institutional experience, particularly in reinforcing the theme of postoperative mobility being a common and significant barrier to discharge.6,7 Furthermore, the significant impact of peripheral nerve blocks on successful same day discharge following total knee arthroplasty was also demonstrated in this institutional experience, supporting the same finding by Shen et al.8 Failing to pass physical therapy protocols was the most common reason for failure to discharge in this institutional experience (Table 3), as echoed by other investigations.6,8 Future iterations of this study may investigate if the threshold for ambulation postoperatively could be further optimized to allow for more successful discharge with similarly positive outcomes. Consistent with existing literature, medical issues like post-operative hypotension and nausea were also leading causes of failed discharge (Table 3).
Further categorizing this discussion to highlight nuances in the cohort of total knee arthroplasty patients, there are several categories that have proved to be interesting. Regarding the use of robotic assistance, the current literature seems to support that robotic-assisted arthroplasty is at least non-inferior to manual arthroplasty in successful same day discharge and short-term outcomes.9,10 Yet, there has been little evidence supporting improved outcomes in the community hospital setting. This study showed a trend towards more SSD patients undergoing robotic surgery (Tables 2,4, Figure 1). Interestingly, current literature suggests that robotic assistance during TKA may help limit dissection and soft tissue retraction, therefore potentially reducing post-operative pain.11,12 While the findings of this retrospective study are not meant to suggest a causative relationship, they do represent an interesting trend aimed at stimulating further discussion regarding the benefits of robotic assistance in same-day TKA. Another debated technique, use of cement, was examined and it was found that significantly more patients undergoing cementless TKA were able to successfully discharge (Table 2), but cement use was not found to be a statistically significant predictor of discharge status on regression analysis (Table 4, Figure 1). These data points further illustrate the lack of clarity on cement use in same day arthroplasty. The traditional thinking of early implant migration as described by van Hamersveld et al.13 could mean micromotion of the implant on the day of surgery, which could potentially lead to higher early postoperative pain scores. Nevertheless, this concept was not reflected in this investigation and further, preferably prospective, examination is needed. Regarding total hip arthroplasty, this review found both novel relationships and supported correlations preexisting in the literature. Interestingly, patients whose surgery was performed by a fellowship-trained surgeon were more likely to discharge than those whose surgery was performed by a non fellowship-trained surgeon (Table 2), yet fellowship training was not found to be a predictor of likelihood to discharge on multivariate analysis (Table 4, Figure1). This represents an interesting finding that underscores the recent debate in the literature examining outcomes when considering fellowship training in total joint arthroplasty.14 In a recent study, Burnett et al reported fewer post-operative complications in revision THA by fellowship trained surgeons when compared to non-fellowship trained surgeons. Future studies similar to this would benefit from subgroup analysis between SSD and FSD patients in regard to fellowship training. Furthermore, this investigation’s findings regarding spinal anesthesia and ambulation distances seem to echo a common theme in the same day total hip arthroplasty literature. Hoeffel et al found that earlier time to ambulation and increased ambulation distances decreased the risk of failed same day discharge.15 Similarly, this study found that patients who underwent THA discharge the same day had undergone spinal anesthesia and ambulated further with physical therapy than those who failed to discharge same day. This data supports the notion that ensuring adequate pain control, using a spinal anesthetic, ensures meaningful participation with physical therapy and therefore further optimizes same day discharge likelihood. In juxtaposition, this relationship was not found in the TKA population. This does appear to suggest there may be an optimal balance, however, between pain control and the inhibition of proprioception, as a large portion of TKA patients also received an adductor canal block. In terms of surgical approach, the anterior approach showed a higher rate of same-day discharge compared to posterior approach. However, multivariate analysis did not find approach to be an independent predictor, aligning with mixed results in the current literature. This finding was supported by Dove et al who found no statistical difference in their study comparing four hip approaches.16
In examination of the current institutions data, it seems as though the best way to optimize successful same-day discharge rates is to optimize the ability to participate with PT through various modes aimed at perioperative pain control and postoperative mobility. While the results of this study may provide some insights when considering same-day total joint arthroplasty, there are limitations inherent to its retrospective nature. Furthermore, although the operative times in the successful and failed groups were similar, there were many different surgeons performing the procedures. As such, specific protocols regarding spinal anesthesia and peripheral nerve blocks varied amongst the surgeons since no standard protocol for these variables exists in our institution. However, spinal anesthesia and peripheral nerve block are widely advocated to improve same-day discharge rates. A major strength of this study is its sample size as many current studies feature small cohorts of patients in academic centers, although it was derived from a broad pool of surgeons. This study can still add value to the limited literature regarding same day perioperative parameters in the community setting. Overall, the authors feel this study aligns with prior research while adding new insights from a community hospital context, especially regarding the nuanced role of perioperative variables in SDD outcomes. While the nature of the study design does not allow for strong correlates to be drawn, the authors aim to open the conversation regarding more nuanced factors regarding operative techniques and technology use while emphasizing the need for larger, prospective studies to better define best practices for optimizing same-day arthroplasty to ensure improved cost-savings and patient outcomes.
Conclusion
Implementation of a same-day discharge protocol for total joint arthroplasty in the community requires a multidisciplinary approach to ensure satisfactory and consistent patient outcomes. Institutional experience is important for the orthopedic community as a learning tool to improve protocols and outcomes. At this institution, peripheral nerve blocks resulted in higher successful discharges. The single most important factor regarding successful discharge seemed to be ambulation in the post-operative unit, which is consistent with a predetermined institutional requirement.
References
- Mathews CG, Stambough JB, Stronach B, Siegel ER, Barnes CL, Mears SC. Successful Transition to Same Calendar Day Discharge in Total Joint Arthroplasty at an Academic Center. Arthroplasty Today. 2024 Mar 16;27:101354. doi: 10.1016/j.artd.2024.101354. PMID: 38524150; PMCID: PMC10958211.
- Lutz RW, Post ZD, Thalody HS, Czymek MM, Scaramella AYE, Ponzio DY, Orozco FR, Ong AC. Success of Same-Day Discharge Total Hip and Knee Arthroplasty: Does Location Matter? J Arthroplasty. 2024 Jan;39(1):8-12. doi: 10.1016/j.arth.2023.06.020. Epub 2023 Jun 17. PMID: 37331445.
- Gromov K, Jørgensen CC, Petersen PB, et al. Complications and readmissions following outpatient total hip and knee arthroplasty: a prospective 2-center study with matched controls. Acta Orthop. 2019; 90(3):281-285
- Mitchell BA, Cleary LM, Samuel LT, et al. An increase in same-day discharge after total joint arthroplasty during the covid-19 pandemic does not influence patient outcomes: a retrospective cohort analysis. Arthroplast Today. 2023; 20:101115.
- Basques BA, Tetreault MW, Della Valle CJ. Same-Day Discharge Compared with Inpatient Hospitalization Following Hip and Knee Arthroplasty. J Bone Joint Surg Am. 2017; 99(23):1969-1977.
- Fraser JF, Danoff JR, Manrique J, Reynolds MJ, Hozack WJ. Identifying Reasons for Failed Same-Day Discharge Following Primary Total Hip Arthroplasty. J Arthroplasty. 2018;33(12):3624-3628. doi:10.1016/j.arth.2018.08.003
- Gong MF, McElroy MJ, Li WT, et al. Reasons and Risk Factors for Failed Same-Day Discharge After Total Joint Arthroplasty. J Arthroplasty. 2024;39(6):1468-1473. doi:10.1016/j.arth.2023.11.032
- Shen TS, Rodriguez S, LeBrun DG, et al. Reasons and Risk Factors for Failed Same-Day Discharge After Primary Total Knee Arthroplasty. J Arthroplasty. 2023;38(4):668-672. doi:10.1016/j.arth.2022.10.044
- Clement ND, Galloway S, Baron YJ, Smith K, Weir DJ, Deehan DJ. Robotic Arm-assisted versus Manual (ROAM) total knee arthroplasty: a randomized controlled trial. Bone Joint J. 2023 Sep 1;105-B(9):961-970. doi: 10.1302/0301-620X.105B9.BJJ-2023-0006.R3. Erratum in: Bone Joint J. 2023 Oct 1;105-B(10):1132. doi: 10.1302/0301-620X.105B10.BJJ-2023-00036. PMID: 37652449.
- Eason T, Mihalko W, Toy PC. Robotic-Assisted Total Knee Arthroplasty is Safe in the Ambulatory Surgery Center Setting. Orthop Clin North Am. 2023 Apr;54(2):153-159. doi: 10.1016/j.ocl.2022.11.001. PMID: 36894288.
- Khlopas A, Sodhi N, Sultan AA, Chughtai M, Molloy RM, Mont MA. Robotic Arm-Assisted Total Knee Arthroplasty. J Arthroplasty. 2018;33(7):2002-2006. doi:10.1016/j.arth.2018.01.060
- Fozo ZA, Ghazal AH, Hesham Gamal M, Matar SG, Kamal I, Ragab KM. A Systematic Review and Meta-Analysis of Conventional Versus Robotic-Assisted Total Knee Arthroplasty. Cureus. 2023;15(10):e46845. Published 2023 Oct 11. doi:10.7759/cureus.46845
- van Hamersveld KT, Marang-van de Mheen PJ, Tsonaka R, Valstar ER, Toksvig-Larsen S. Fixation and clinical outcome of uncemented peri-apatite-coated versus cemented total knee arthroplasty : five-year follow-up of a randomised controlled trial using radiostereometric analysis (RSA). Bone Joint J. 2017 Nov;99-B(11):1467-1476. doi: 10.1302/0301-620X.99B11.BJJ-2016-1347.R3. PMID: 29092985.
- Burnett RA, Dobson CB, Amr Turkmani, Sporer SM, Levine BR, Della CJ. Revision Hip Arthroplasty Performed by Fellowship-Trained Versus Non-Fellowship-Trained Surgeons: A Comparison of Perioperative Management and Complications. The Journal of Arthroplasty. 2024;39(9):S161-S165. doi:https://doi.org/10.1016/j.arth.2024.06.029
- Hoeffel, Daniel P. MD; Daly, Peter J. MD; Kelly, Brandon J. MD; Giveans, M. Russell PhD. Outcomes of the first 1,000 total hip and total knee arthroplasties at a same-day surgery center using a rapid-recovery protocol. JAAOS: Global Research and Reviews. 2019;3(3):022.
- Dove J, Laperche J, Kutschke M, Painter D, Antoci V, and Cohen E. The effect of surgical approach on the outcomes of same-day discharge outpatient total hip arthroplasty at a single ambulatory surgery center. The Journal of Arthroplasty. 2024;39(2):398-401.
