
Ji Young Chung, D.O.; Frederick Korpi, D.O.; Ericka Glass, M.D.; Jeffrey Cochran, D.O.
Aultman Hospital
DOI: 10.70709/qsjlob7g2x
Abstract
Case
We present a case of a closed, farm-related orthopedic injury that was complicated by C. perfringens infection. With staged surgical procedures and intravenous antibiotics, the infection was successfully eradicated, and the fracture went onto successful union.
Conclusion
Clostridium perfringens is a Gram-positive, anaerobic, spore-forming bacteria that is ubiquitous in the environment. C. Perfringens infections usually manifest as necrotizing fasciitis in orthopedic settings, but it may also lead to post-traumatic soft tissue and bony infections after closed fractures. This case demonstrates that delayed anaerobic infections should not be overlooked in the agricultural patient population even in closed fractures.
Keywords: Clostridium perfringens, infection, closed fracture, farm injury, fracture blister
Introduction
Clostridium perfringens is a well-known cause of gas gangrene, a rapidly progressive and life threatening myonecrosis characterized by the production of foul-smelling gas. Clostridium species is a Gram-positive, anaerobic, spore-forming bacilli commonly found in soil, animal intestines, marine sediments, and sewage[1]. As such, clostridial infections occur with deep contaminated penetrating open injuries [2] and mainly affect soft tissue. C. perfringens-induced diseases are often complicated by rapid bacterial overgrowth, gas production, and toxin production[3].
Common microorganisms that lead to wound infections include Staphylococcus aureus, Staphylococcus pyogenes, Enterococci species, and Pseudomonas aeruginosa [4]. There are limited reports of C. perfringens in the setting of bony traumas. In this report, we present a unique case of a patient whose closed tibial shaft fracture was complicated by C. perfringens infection.
Statement of Informed Consent
Informed consent for publication was obtained from the patient.
Case Report
Patient is a 68-year-old male dairy farmer who sustained a closed displaced distal third tibial shaft fracture with associated proximal third fibular shaft fracture after 15 bales of hay fell onto his right leg (Fig. 1). CT was obtained in the emergency department, which redemonstrated the fracture without subcutaneous gas. There was no involvement of the ankle joint. Patient underwent tibial intramedullary nailing the following day (Fig. 2).


Reduction was obtained with closed manipulation of the fracture without the use of percutaneous reduction clamps, and Stryker T2 Alpha intramedullary tibial nail was inserted using standard suprapatellar approach. Two proximal and two distal interlocking screws were placed percutaneously. Patient was discharged home in stable condition on post-operative day 1 after finishing 24 hours of peri-operative IV antibiotics (cefazolin 2g IV q8hr). Patient was placed in a bulky jones splint and was instructed to remain non-weightbearing on the operative leg until his incisions were healed. He was prescribed oral cephalexin 500mg QID for 7 days at discharge as the operating surgeon had concerns for significant swelling and tenuous skin integrity at the end of the case.
Patient was scheduled to be seen in clinic 1 week later for skin checks, but he did not show. At his first follow up 3 weeks post-operatively, circumferential fracture blisters were noted with the most significant one on his anterior lower leg. The fracture blisters did not encompass the distal interlocking screw incisions. Patient was prescribed oral doxycycline and wounds were treated with dry sterile dressing changes. At subsequent weekly follow-ups, the fracture blisters evolved to eschars and then into a draining wound. Another course of oral doxycycline was prescribed. Of note, patient admitted that he had not been adhering to non-weightbearing orders and had begun working around his farm.
Approximately 3 months post-operatively, patient had an episode of increased right lower extremity pain and sudden inability to bear weight. Subsequently, he presented to the ED with fever (38.2∞C), hypoxia, tachycardia, and purulent drainage from the wound. Blood cultures were positive for C. perfringens, and wound culture was positive for C. perfringens and E. faecalis. Radiographs demonstrated minimal callus formation of the tibia (Fig. 3).

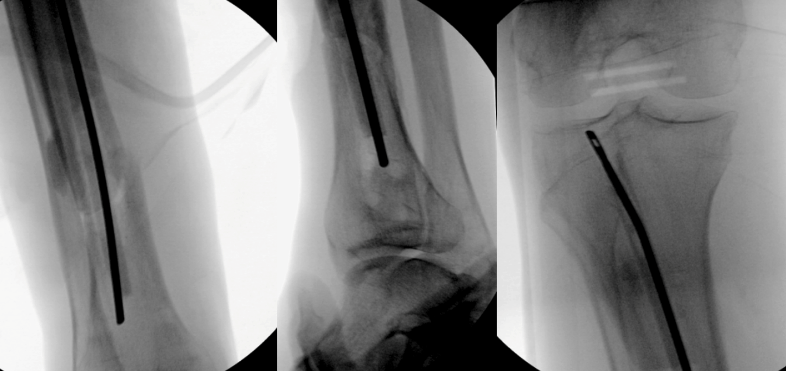
On CT, there was subcutaneous gas at the level of the wound, but no drainable fluid collection was noted. Patient began IV daptomycin, piperacillin/tazobactam, and clindamycin therapy per culture and susceptibility report. Patient was admitted for surgical intervention of his infection. During the first irrigation and debridement, it was noted that the anterior leg wound communicated with the initial fracture site. Intraoperative cultures were obtained, and they were also positive for C. perfringens and E. faecalis. Repeat irrigation and debridement was performed on post-operative day 4. A PICC line was placed the next day. Eight days after admission, patient underwent tibial nail removal, and repeat I&D. Interestingly, a foul-smelling odor was appreciated during the nail extraction. An antibiotic spacer was assembled using an Ender’s nail, bone cement, tobramycin, vancomycin and methylene blue. This was placed in the intramedullary canal and across the fracture site, and adequate fracture reduction was verified on fluoroscopy (Fig. 4). A negative pressure wound dressing was placed on the anterior leg wound for 6 weeks. Final antibiotics were adjusted to clindamycin and meropenem due to patient’s adverse reaction to penicillin G.
Six weeks later, patient underwent removal of the antibiotic nail and placement of tibial intramedullary nail coated with tobramycin infused cement. During this final procedure, no foul-odor was appreciated. Tibial reamings were sent for culture, which was positive for rare E. faecium, but negative for C. perfringens. At his subsequent post-operative visits, anterior leg wound had healed uneventfully. Final follow up was at approximately 2 years post-operatively, and radiographs demonstrated successful fracture union (Fig. 5).

Discussion
There is a paucity of literature regarding Clostridium perfringens osteoarticular infection. These studies are limited to contaminated open fractures or prosthetic joint infections. To our knowledge, this is the first report of a C. perfringens infection identified in a closed fracture of a surgery-naïve extremity.
In 2012, Baker et al. reported a case of total hip periprosthetic fracture fixation complicated by C. perfringens [5]. Thirteen days status post open reduction and internal fixation of total hip periprosthetic fracture, authors noticed surgical site infection and subcutaneous gas on plain radiographs. Patient was treated with aggressive irrigation and debridement without removal of implants and 7 days of IV metronidazole and piperacillin/tazobactam followed by 4 weeks of oral metronidazole.
In their retrospective review, Ibnoulkhatib et al. analyzed 12 cases of open fractures that were infected with Clostridium spp. [6]. These patients sustained high-energy trauma with soil contamination and significant soft tissue damage. As they were open fractures with environmental contaminants, microbiological studies revealed polymicrobial infection, and only one case involved C. perfringens. These injuries often presented with post-operative skin necrosis, delayed wound healing, and purulent discharge. Appropriate initial IV antibiotics administration was futile, as it is ineffective against Clostridium spores. Nearly all patients required secondary surgeries such as two-stage Masquelet procedure, decortication with bone grafting, and delayed fixation. Tremp et al. reported two cases of clostridial osteomyelitis following open ankle fracture dislocations [7]. Both cases were treated with extensive and serial bony debridement and eventual ankle arthrodesis.
Other than heavily contaminated open fractures and history of biliary sepsis [8, 9], there is no known risk factor for bony C. perfringens infection. Our patient is a hard-working dairy farmer who admitted to noncompliance with weightbearing orders and returning to work sooner than instructed. Anaerobic soft and bony infections are more commonly associated with agricultural injuries than non-agricultural trauma[10]. Clostridium spp. is ubiquitous in the environment [1], and with his early return to the field, our patient likely was exposed to C. perfringens spores. We suspect that his infection began at the fracture blister. It likely extended deeper into subcutaneous tissue and eventually communicated with his fracture site. Clostridium spores may have extended into the medullary canal and persisted in poorly vascularized bone [6].
Our patient underwent multiple unsuccessful sessions of oral antibiotic therapy for the fracture blister infection. Post-operative prophylactic cephalexin 500mg QID for 5 to 7 days is commonly used amongst lower extremity orthopedists under the surgeons’ discretion [11]. Although there was no frank fracture blister at the time of the initial surgery, there was a concern for fracture blisters due to the soft tissue swelling and poor skin integrity of his distal leg. Thus, our surgeon decided to prescribe oral antibiotics on discharge [12]. Doxycycline was chosen in outpatient setting for its MRSA coverage, and as it is a recommended treatment option for purulent skin and soft tissue infections according to the Infectious Diseases Society of America [13]. Our patient underwent two superficial irrigation and debridement of the anterior leg wound when the infection was noted to communicate with fracture site. He was ultimately treated with long-term IV antibiotics treatment, removal of hardware, I&D, placement of intramedullary antibiotic spacer for 5 weeks, and final placement of antibiotic coated tibial intramedullary nail. Fortunately, only minimal amount of bone at fracture edges had to be resected during this process.
This unique case demonstrates the importance of close monitoring of soft tissue defects even in closed fractures, especially after farming-related injuries. Anaerobic orthopedic infections almost exclusively occur in agricultural injuries. Thus, there should be a high index of suspicion for atypical soft tissue and bony infection such as with Clostridium perfringens in this patient population.
Abbreviations
- I&D: irrigation and debridement
- IV: intravenous
References
- Matches, J.R., J. Liston, and D. Curran, Clostridium perfringens in the environment. Appl Microbiol, 1974. 28(4): p. 655-60.
- Leiblein, M., et al., Clostridial Gas Gangrene – A Rare but Deadly Infection: Case series and Comparison to Other Necrotizing Soft Tissue Infections. Orthop Surg, 2020. 12(6): p. 1733-1747.
- Fu, Y., T. Alenezi, and X. Sun, Clostridium perfringens-Induced Necrotic Diseases: An Overview. Immuno, 2022. 2(2): p. 387-407.
- Khandia, R., et al., Wound Infection with Multi-Drug Resistant Clostridium Perfringens: A Case Study. Arch Razi Inst, 2021. 76(5): p. 1565-1573.
- Baker, J.F., M.H. Vioreanu, and J.A. Harty, Clostridium perfringens infection complicating periprosthetic fracture fixation about the hip: successful treatment with early aggressive debridement. Hip Int, 2012. 22(1): p. 122-5.
- Ibnoulkhatib, A., et al., Post-traumatic bone and/or joint limb infections due to Clostridium spp. Orthop Traumatol Surg Res, 2012. 98(6): p. 696-705.
- Tremp, M., et al., Clostridial Infection After Open Fractures of the Lower Extremity – Report of Two Cases and Discussion of Pathomechanism and Treatment. In Vivo, 2020. 34(1): p. 291-298.
- Wilde, A.H., R.S. Sweeney, and L.S. Borden, Hematogenously acquired infection of a total knee arthroplasty by Clostridium perfringens. Clin Orthop Relat Res, 1988(229): p. 228-31.
- Vogely, H.C., et al., Hematogenous infection of a total hip prosthesis due to Clostridium perfringens. Clin Infect Dis, 1999. 28(1): p. 157-8.
- Wynn, M., et al., Agricultural Trauma Causing Open Fractures: Is Antibiotic Coverage Against Anaerobic Organisms Indicated? J Orthop Trauma, 2022. 36(2): p. e51-e55.
- Ruta, D.J., A.R. Kadakia, and T.A. Irwin, What are the patterns of prophylactic postoperative oral antibiotic use after foot and ankle surgery? Clin Orthop Relat Res, 2014. 472(10): p. 3204-13.
- Sinha, S., et al., The Current Consensus on the Management of Post-traumatic Blisters Among Orthopaedic Surgeons. Indian J Orthop, 2022. 56(6): p. 1011-1017.
- Stevens, D.L., et al., Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis, 2014. 59(2): p. e10-52.
