
Ryan Arboleda, MPH, OMS 20261; Ally Spohn, OMS 20261; Benjamin Pfeiffer, MS, OMS 20261; Dean Gubler, DO, MPH2
1Rocky Vista University College of Osteopathic Medicine Englewood CO
2Rocky Vista University College of Osteopathic Medicine – Southern Utah
DOI: 10.70709/3hmz0k5td2
Abstract
Case
This case report describes a rare intraoperative discovery of a conjoined nerve root (CNR) at L4-L5 in a 74-year-old male undergoing L4-S1 TLIF for chronic lower back pain and radiculopathy. Although preoperative MRI showed stenosis and spondylolisthesis, it did not reveal the CNR, which was identified during the osteotomy when the L4 nerve root was seen merging with the L5 root across the disc space. The surgeon proceeded with caution, protecting the nerve root during cage placement, and the patient experienced complete symptom resolution postoperatively, returning to daily activities within three weeks.
Conclusion
Transforaminal lumbar interbody fusion (TLIF) is used to treat spinal cord and nerve root compression. Anatomical anomalies like CNRs can complicate spinal procedures. This case highlights the limitations of imaging in detecting CNRs and emphasizes the importance of intraoperative awareness to avoid injury to anomalous nerve roots or other anatomical variants.
Keywords: Conjoined nerve root, fusion, MR neurography, CT myelography
Introduction
A conjoined nerve root (CNR) is an anatomical variation where two adjacent nerve roots share a portion of the dural sac as they exit the spinal cord. The estimated prevalence of CNRs ranges from 0.25% to 17% on magnetic resonance imaging (MRI) and computed tomography (CT) imaging1. However, cadaveric studies suggest a prevalence as high as 30%2,3. CNRs most commonly involve the L5 and S1 nerve roots, but any nerve root can be affected and are classified into four types using the Neidre and MacNab’s Classification: (1) conjoined, (2) redundant, (3) anastomotic, and (4) fused3,4.
Not all CNRs are symptomatic, but they can present with lower extremity radiculopathy or neurogenic claudication, symptoms that overlap with conditions like disc herniations and spinal stenosis, complicating clinical diagnosis2. MRI is the most accurate and non-invasive imaging modality for detecting CNRs. CT myelography, which uses contrast dye to enhance visualization of the spinal cord and nerve roots, can be helpful when MRI findings are inconclusive3. Despite advanced imaging, CNRs are sometimes misdiagnosed as disc herniations or other compressive nerve root pathologies and are discovered intraoperatively, increasing the risk of surgical complications such as nerve root injury1–3,5.
Several cases in the literature highlight how preoperative identification of CNRs can alter surgical approach and reduce nerve injury risk. For example, in one TLIF case, a CNR at L5-S1 was safely managed by placing the cage from the contralateral side6. Another case used CT myelography to identify a CNR prior to microdiscectomy and was able to safely approach from the contralateral side5,7. However, CNRs are not always detected preoperatively. One case series outlines two Type 1A CNRs which were discovered during minimally invasive discectomy, requiring contralateral decompression for safe retraction with successful outcomes4,8.
Statement of Informed Consent: The patient in this case provided both written and oral consent to document and publish the details of their case.
Case Report
Initial Presentation
A 74-year-old male presents with chronic low back pain radiating to the buttocks and bilateral lower extremities. He also reports associated right-sided weakness and numbness. Symptoms have been present for 30 years without a known inciting event, and are worse with prolonged walking or activity and relieved by sitting. Review of systems is notable for increased nocturnal urinary frequency, which he attributes to a history of BPH. He denies incontinence, saddle anesthesia, upper extremity symptoms, or axial pain above the lumbar spine. He was previously diagnosed with L5-S1 spondylolisthesis and L5 radiculopathy, with good response to physical therapy. Over the past 5 years, symptoms have gradually worsened, and he received two epidural injections with temporary relief.
Physical exam of the patient reveals an antalgic gait and a non-tender lumbar spine with a step-off deformity present at L5-S1. Right-sided facet loading elicits radicular symptoms in the right lower extremity. Motor strength is 5/5 the hip flexors, abductors, adductors, quadriceps, hamstrings, extensor hallucis longus (EHL), and plantar flexors. Motor strength in the right dorsiflexors group is 4/5, compared to 5/5 on the left. Sensory examination reveals intact sensation in the L1-S1 dermatomes on the left. On the right, there is decreased subjective sensation over the anterolateral aspect of the leg and severe numbness on the dorsum of the foot and toes. The remainder of the physical exam is unremarkable.
X-rays of the lumbar spine revealed a 10 mm spondylolisthesis, secondary to a pars defect at the L5-S1 level. Flexion and extension views demonstrate a reduction in the spondylolisthesis from 10mm to 6mm in extension. Disc height loss and degenerative changes are noted from L4-S1.
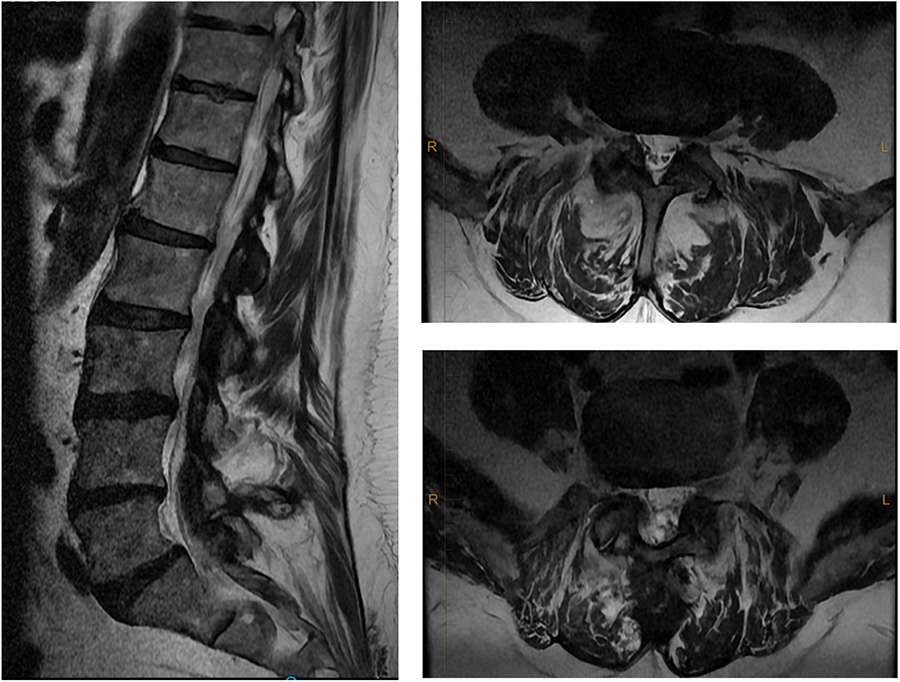
Lumbar MRI revealed annular bulging from L1-L4 without significant canal or foraminal narrowing. At L4-5, there is moderate disc space narrowing, a 5mm retrolisthesis, and a synovial cyst arising from the medial margin of the right zygapophyseal joint. Posterolateral and far lateral osteophytes are present with mild foraminal narrowing but no canal stenosis. At L5-S1, there is a 9mm anterolisthesis with bilateral pars defects, as well as bilateral foraminal and lateral recess stenosis. There is also moderate disc space narrowing and mild canal stenosis noted (Figure 1). After discussion treatment options, the patient elected to proceed with a L4-S1 TLIF.
Operative Course
The L4 and L5 spinous processes were palpated and marked. A midline incision was made, and the underlying subcutaneous tissue and erector spinae muscles were dissected from the spinous processes. After confirming the appropriate levels via fluoroscopy pedicle screws were placed bilaterally from L4-S1.
A left pars osteotomy was performed to allow for cage placement from the left side. Shortly after this, a low-lying L4 nerve root was identified crossing over the disc space to the level of L5. After adequate visualization was obtained, the anomaly appeared to be most consistent with a type 1A CNR, which the surgeon or radiologist did not note on available pre-operative imaging. This could have complicated cage placement, due to the risk of nerve injury. However, the decision was made to proceed with cage placement from the left. The pars osteotomy was already performed on the left side, and the cage being used was a 10mm 5-module VTI cage. This system contains 5 individual modules that are placed sequentially and interlock to form one larger cage. Each module was placed while protecting the nerve root with a Penfield 1 instrument. Because of the smaller profile of each module, the interbody cage was placed without causing excessive traction on the anomalous nerve root.
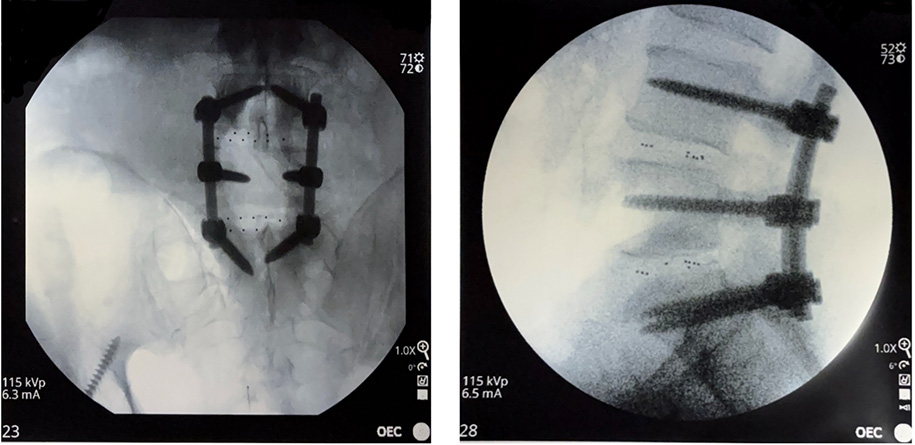
Next, an L5-S1 Gill laminectomy revealed a significant amount of fibrous tissue compressing the L5 nerve root bilaterally, secondary to the pars defect. The nerve roots were traced into the extra-pedicular zone, and a far-lateral decompression was performed bilaterally. A 10 mm, 5-module VTI cage was placed from left to right at L5-S1. After placement of both cages, rods were contoured to the lumbar segment and secured to the pedicle screws. Final intraoperative x-rays confirmed satisfactory placement of the hardware and correction of the spondylolisthesis (Figure 2).
The wound was irrigated, and bone graft soaked in bone marrow aspirate were placed in the intertransverse and facet joints. The sacrum was osteotomized to ensure adequate fusion. Finally, vancomycin powder and antibiotic beads were applied to the surgical site, and a multilayered closure was performed, with a deep drain in place.
Post-operative Course
The patient tolerated the procedure well, with no immediate complications. In the hospital, laboratory values remained within normal limits, and the surgical incision remained intact. The drain was removed on postoperative day 2, and the patient was discharged. At 3-weeks postoperatively, the patient reported near-complete resolution of right-sided numbness and demonstrated full (5/5) strength in all lower extremity muscle groups. By 3 months, the patient reported complete resolution of symptoms and had returned to normal activity.
Discussion
CNRs present a unique surgical challenge due to their aberrant path and increased vulnerability to iatrogenic injury2,7,8. When CNRs are detected preoperatively, alternate fusion approaches, including anterior lumbar interbody fusion (ALIF) or extreme lateral interbody fusion (XLIF), may be considered to avoid excessive nerve root manipulation9,10. TLIF, a widely used interbody fusion technique, offers the advantage of direct decompression through a posterior approach but poses increased risks in CNR cases due to the need for nerve retraction6,11. Minimally invasive techniques are less disruptive to surrounding tissues, but may not be ideal for visualizing anomalous roots2,5,7. If a CNR is discovered intraoperatively and visualization remains inadequate, it may be necessary to use an alternative approach to avoid nerve injury10.
The increasing recognition of conjoined nerve roots (CNRs) underscores the importance of thorough preoperative imaging in surgical decision-making. Although advanced imaging modalities, such as oblique lumbar MRI and MR neurography, have shown promise in detecting CNRs, their routine integration into preoperative workflows remains limited due to issues of accessibility and cost1,11,12. Further research is needed to establish standardized imaging protocols for CNR detection and to identify the most effective surgical strategies for managing this anatomical variation5,7.
When selecting a surgical approach for lumbar fusion in patients with CNRs, preoperative imaging, particularly oblique MRI and MR neurography, plays a critical role in identifying anomalous nerve trajectories and guiding technique and hardware selection preoperatively. However, if a CNR is encountered intraoperatively, modifications to the planned technique may be required to avoid nerve injury. The ability to tailor the surgical approach based on the presence and location of the CNR is fundamental in reducing perioperative complications and optimizing patient outcomes.
References
- Trimba R, Spivak JM, Bendo JA. Conjoined nerve roots of the lumbar spine. Spine J. 2012;12(6):515-524. doi:10.1016/j.spinee.2012.06.004
- Lotan R, Al-Rashdi A, Yee A, Finkelstein J. Clinical features of conjoined lumbosacral nerve roots versus lumbar intervertebral disc herniations. Eur Spine J. 2010;19(7):1094-1098. doi:10.1007/s00586-010-1329-6
- Schubert R, Campos A, Sharma R. Conjoined nerve root. In: Radiopaedia.Org. Radiopaedia.org; 2011. doi:10.53347/rID-16025
- Abdeldjalil B, Knipe H, Alhusseiny K. Lumbar nerve root anomaly classification. In: Radiopaedia.Org. Radiopaedia.org; 2023. doi:10.53347/rID-160490
- Takagi Y, Yamada H, Ebara H, et al. Conjoined lumbosacral nerve root: a case report. J Med Case Reports. 2024;18(1):91. doi:10.1186/s13256-024-04415-4
- Drossopoulos PN, Ononogbu-uche FC, Tabarestani TQ, et al. Evolution of the Transforaminal Lumbar Interbody Fusion (TLIF): From Open to Percutaneous to Patient-Specific. J Clin Med. 2024;13(8):2271. doi:10.3390/jcm13082271
- Kuroki H, Nagai T. Conjoined nerve root in a patient with lumbar disc herniation accompanied by a lumbosacral spine anomaly: a case report. J Med Case Reports. 2023;17(1):82. doi:10.1186/s13256-022-03749-1
- Sharma A, Singh V, Agrawal R, et al. Conjoint Nerve Root an Intraoperative Challenge in Minimally Invasive Tubular Discectomy. Asian Spine J. 2021;15(4):545-549. doi:10.31616/asj.2020.0250
- Yaman O, Ozer A. Novel L5-S1 interbody fusion technique for root anomalies or abnormal root configurations of L5-S1 foramens. J Craniovertebral Junction Spine. 2018;9(3):163. doi:10.4103/jcvjs.JCVJS_33_18
- Lightsey HM, Xiong GX, Schoenfeld AJ, Simpson AK. Microendoscopic decompression of conjoined lumbosacral nerve roots. BMJ Case Rep. 2022;15(3):e248680. doi:10.1136/bcr-2021-248680
- Heo DH, Kim SW, Chang HH, Park CK. Usefulness of Oblique Lumbar Magnetic Resonance Imaging for Nerve Root Anomalies and Extraforaminal Entrapment Lesions. Asian Spine J. 2018;12(3):423-427. doi:10.4184/asj.2018.12.3.423
- Zickler CL, Martinez Elejalde J, Landa-Galindez A. An Incidental Diagnosis of Conjoined Nerve Root After a Work-Related Back Injury: A Case Report. Cureus. Published online September 2, 2024. doi:10.7759/cureus.68436
