
McAninch, Chase, OMS-IV1; Dellamaggiore, Gino, MD2
1University of Pikeville, Kentucky College of Osteopathic Medicine
2VA Sierra Nevada Health Care System
DOI: 10.70709/6ms4b5j8ay
Abstract
Background
Posterior interosseous nerve neurectomy (PINN) has been reported to provide durable pain relief and preserve wrist range of motion (ROM), particularly in active patients. This case report describes a 21-year follow-up after isolated PINN for chronic wrist pain of unclear etiology in a military service member.
Case Presentation
A 50-year-old right-hand dominant male presented at age 29 with dorsal wrist pain following a training exercise while on active-duty as a Navy SEAL. At the time, conservative management—including NSAIDs, splint immobilization, and physical therapy—failed to relieve symptoms. While the working diagnosis at the time was scapholunate ligament injury, definitive diagnosis via MRI was inconclusive for scapholunate pathology. Tenderness over the scapholunate interval and clinical suspicion led to the decision for diagnostic arthroscopy and simultaneous posterior interosseous neurectomy. The decision to perform posterior interosseous neurectomy was driven by the patient’s desire to preserve wrist ROM and avoid more invasive procedures. At the 21-year follow-up, the patient reported no chronic pain, preserved function, and remained physically active in all desired activities. Physical exam and radiographs showed no signs of scapholunate instability or arthritis.
Conclusion
This case highlights the potential efficacy of posterior interosseous neurectomy in treating chronic dorsal wrist pain, even when underlying pathology is uncertain. The patient demonstrated excellent long-term pain relief and functional outcomes. Posterior interosseous neurectomy may serve as a valuable motion-preserving option in select patients with refractory wrist pain of unclear origin.
Keywords: Posterior interosseous nerve neurectomy, refractory wrist pain, wrist denervation, proprioception, military
Introduction
Chronic dorsal wrist pain presents a diagnostic and therapeutic challenge, particularly in active populations. While conditions such as scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) often underlie persistent wrist symptoms, some patients present without clear imaging or clinical findings to support a specific diagnosis. In such cases, treatment must balance pain relief with preservation of function.
The posterior interosseous nerve neurectomy procedure has been used to treat pain in degenerative wrist conditions, often as an adjunct to other procedures. However, its use as a standalone intervention in cases of uncertain etiology remains less well defined. This report details the case of a military service member with chronic dorsal wrist pain treated with isolated PINN, demonstrating excellent long-term results. Continued research on PINN has yielded promising results of improved ROM, maintained proprioception, and its use as an alternative to and/or additional procedures in more invasive wrist operations.
Case Presentation
A 50-year-old right-hand dominant male, previously an active-duty Navy SEAL, initially presented at age 29 with insidious onset of dorsal left wrist pain following a training exercise. Examination revealed localized tenderness over the scapholunate interval and reduced range of motion. Radiographs showed no evidence of fracture, instability, or arthritic change. MRI was inconclusive of local scapholunate pathology. Conservative management with NSAIDs, splint immobilization, and physical therapy was unsuccessful.
Given persistent symptoms and desire to maintain wrist function, the patient elected to undergo diagnostic wrist arthroscopy with simultaneous posterior interosseous neurectomy to address his persistent wrist pain at rest and with activity. Operative records demonstrated no definitive findings of scapholunate ligament injury, and the original etiology remained unclear. The patient denied any complications after the posterior interosseous neurectomy.
At 21-year follow-up, the patient reported complete resolution of pain, relatively preserved wrist function, and unrestricted participation in recreational activities. Physical exam demonstrated near-normal wrist motion with minor limitations. Follow-up radiographs showed no evidence of instability or osteoarthritic degenerative changes.
Treatment
Initial management included NSAIDs and wrist immobilization. After these failed, diagnostic wrist arthroscopy and posterior interosseous nerve neurectomy were pursued due to inconclusive imaging and the patient’s desire to remain physically active. The goal was pain relief while preserving wrist motion.
Observations
The original radiographs from 2001 were not available for this study. Clinical suspicion for scapholunate injury was based on tenderness over the dorsal scapholunate interval; however, imaging and arthroscopy were negative. Posterior interosseous nerve neurectomy was selected due to persistent pain, failed conservative treatment, and inconclusive diagnostics.
X-Ray Report 1/4/2001:
“Multiple views of the bilateral wrists examined without prior comparison studies demonstrated an unfused ossification center at the ulnar styloid on the left. There was no evidence of fracture, dislocation, or subluxation in the left wrist. The bone and soft tissue structures were otherwise unremarkable. Multiple views of the right wrist demonstrated no fracture, dislocation, or subluxation. Bone and soft tissues of the right wrist are unremarkable.”

X-Ray Report 11/18/2022:
“Normal bone mineralization. No acute fractures were noted. No subluxation or dislocation was observed. No significant degenerative changes were observed. Two punctate calcifications were observed in the triangular fibrocartilage complex. These could be old fracture fragments or ununited accessory ossification centers of the ulnar styloid process.”
The absence of degenerative changes or instability on radiographs at 21-year follow-up may suggest that the original pathology was less severe than initially suspected. Moreover, the patient reported the patient’s significant pain resolution and preserved function support the potential utility of PINN in select cases even when the exact etiology of wrist pain is uncertain.
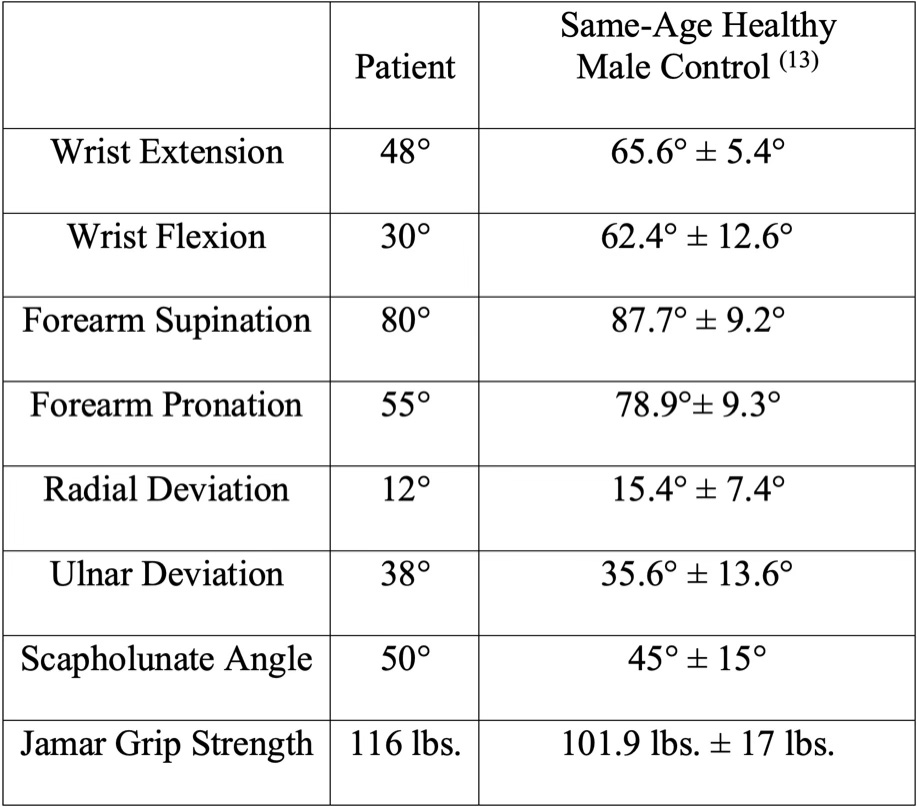
Physical examination at the 21-year follow-up on November 18, 2022, showed left wrist dorsiflexion of 48° and volar flexion of 30°. The patient was able to supinate his left wrist at 80° and pronate it at 55°. He achieved a left wrist radial deviation of 12° and ulnar deviation of 38°. He had a palpable click during range-of-motion testing. The scapholunate angle of the patient was 50°. Jamar grip strength testing revealed a right-hand grip strength of 120 lbs and left-hand grip strength of 116 lbs (See Table 1). The patient’s values compared quite similarly to that of the average healthy 50-year-old male and may suggest the efficacy of PINN in preserving ROM while also addressing chronic wrist pain in those with diagnostically unclear etiology. (13)
Discussion
In practice, a posterior interosseous nerve neurectomy is performed through a dorsal longitudinal incision proximal to the distal radioulnar joint. (2) The extensor tendons of the fourth extensor compartment are retracted to the ulnar side of the wrist. The posterior interosseous nerve is easily identified at this point in the procedure. The interosseous membrane is divided to provide access to the nerve body, where a portion or the entire nerve can be excised, depending on the procedure. (4), (16)
The posterior interosseous nerve innervates a large portion of the central wrist, including the wrist capsule, scaphoid, lunate, and dorsal and distal radius. PINN was first described in 1966 by Wilhelm, who performed dorsal wrist denervation in patients with wrist injuries. (4) He found that the procedure reduced wrist pain while maintaining wrist movement. Early studies showed that PINN was highly variable in pain reduction, with success ranging from 12-95%. (4), (15) However, a second study 11 years later showed good pain relief in 80% of patients up to 2 years after the treatment. (16)
Many studies have shown high efficacy rates of PINN in reducing pain in patients experiencing chronic wrist pain. (7), (8), (18) ROM is of greatest concern in patients with similar injuries because many of the other surgical alternatives have proven to variably decrease ROM. (3), (7), (8) PINN has been used in an isolated manner, as observed in the present case, but it can also be used in addition to other wrist procedures to reduce wrist pain.
Five studies involving 135 patients with an average follow-up period of 51 months showed promising results in terms of positive outcomes after PINN. The studies collectively found improved flexion and extension ranging from 20°, 40°, to 60° and radial and ulnar deviation up to 10°. (1), (2), (15) Of the 135 patients included in these studies, 88.4% subjectively reported improved proprioception. (1), (2) Furthermore, these studies found that 88.9% of patients returned to work following posterior interosseous nerve neurectomy. Most notably, these studies found that 96% of patients experienced an increase in ROM after PINN. (12) Furthermore, a study of 23 patients found that after 2.5 years, 80% of the patients reported a decrease in pain, 73% returned to work, and 90% would recommend the procedure. (11)
Another important measure of outcomes after PINN is proprioception. Conscious proprioception is transmitted via the posterior column-medial lemniscus pathway to the cerebrum (9), (10), whereas unconscious proprioception is conveyed along the dorsal spinocerebellar pathway to the cerebellum. (9), (10) Overall, proprioception provides the relative ability to gauge the position of the body in space. Patterson compared the proprioception of the surgical wrists of 23 patients who had undergone PINN with their nonsurgical wrists and against the wrists of 23 healthy volunteers. (9) This study found no statistically significant differences in wrist proprioception, except at 40° of extension. (10), (12)
Moreover, this study found that PINN does not appear to be associated with decreased proprioception when compared to healthy volunteers. (9) Unlike patients with Charcot arthropathy due to diabetes mellitus, patients who underwent posterior interosseous neurectomy showed little disruption of proprioception. (9), (10) Altogether, patients who had undergone a PINN and control patients showed an overall similarity in their conscious awareness of their wrists in space, and thus similar proprioceptive sensation. (10)
Although a PINN may be sufficient as a stand-alone treatment, it is not without complications. Two studies that followed a total of 51 patients collectively reported that 13/51 (25.5 %) patients had a recurrence of wrist pain at an average of 12.3 months. (5), (6) These two studies also concluded that an average of 13.5% of patients required reoperation after a PINN. (5), (6) Recurrence of wrist pain and reoperation were statistically the most prevalent complications, but two other studies showed a prevalence of 1/113 patients or 0.9% of complications (excluding pain recurrence) after the PINN procedure. (16), (17) These complications were originally discussed with this patient, and the patient decided that the benefits outweighed the harms of a posterior interosseous nerve neurectomy procedure versus the possibility of more severe complications from no intervention, such as osteoarthritis.
Similarly, a study of 95 military members who underwent PINN in combination with other surgical wrist treatments analyzed the patient outcomes and possible complications. The study found that greater than 75% of the 95 military members experienced pain resolution. (9) Due to the demands of the physical and recreational activities of the patient in this study, PINN was decided as the best course of action. In this case, the patient was able to return and complete his career in the Navy SEALs, play the banjo and guitar, participate in physically demanding recreational activities, and did not have any complaints of chronic wrist pain or loss of proprioception at the last follow-up.
Initial clinical suspicion was directed toward a scapholunate ligament injury according to inconclusive MRI and negative arthroscopic findings. However, this case raises important considerations about the role of PINN in the management of chronic dorsal wrist pain with unclear etiology. The long-term absence of radiographic evidence of instability, osteoarthritic, or degenerative change supports the value of PINN in appropriately selected patients. This report underscores the importance of considering PINN in patients who prioritize motion preservation and fail conservative management, even when the underlying diagnosis remains uncertain.
Conclusion
In this case, a highly active patient with chronic dorsal wrist pain of unclear etiology achieved long-term resolution of symptoms and preserved function following posterior interosseous nerve neurectomy. Despite diagnostic uncertainty, the procedure has provided long-lasting relief and allowed the patient to maintain a physically demanding lifestyle. This report supports consideration of isolated PINN in select patients with refractory wrist pain where traditional reconstructive options may be excessive or undesirable. This report adds to the limited literature supporting PINN as a stand-alone, motion-preserving intervention for chronic dorsal wrist pain of uncertain etiology. Further research is warranted to clarify the role of posterior interosseous nerve neurectomy in similar clinical scenarios.
References
- Abdelaziz AM, Aldahshan W, El-Sherief FAH, Wahd YESH, Soliman HAG. Posterior interosseous neurectomy alternative for treating chronic wrist pain. J Wrist Surg. 2019;8(2):142-148. doi:10.1055/s-0038-1677507
- Braga-Silva J, Román JA, Padoin AV. Wrist denervation for painful conditions of the wrist. J Hand Surg Am. 2011;36(6):961-966. doi:10.1016/j.jhsa.2011.03.004
- Chen R, Calfee RP, Stepan J, Osei DA. Outcomes of acute versus subacute scapholunate ligament repair. J Hand Surg Am. 2015;40(9):1809-1815. doi:10.1016/j.jhsa.2015.06.055
- Chin KW, Engelsman AF, van Gulik TM, Strackee SD. Selective denervation of the wrist for chronic pain: a systematic literature review. J Hand Surg Eur Vol. 2020;45(3):265-272. doi:10.1177/1753193419886777
- Dellon AL, Mackinnon SE, Daneshvar A. Terminal branch of anterior interosseous nerve as source of wrist pain. J Hand Surg Br. 1984;9(3):316-322. doi:10.1016/0266-7681(84)90051-2
- Ferreres A, Suso S, Foucher G, Ordi J, Llusa M, Ruano D. Wrist denervation: surgical considerations. J Hand Surg Br. 1995;20(6):769-772. doi:10.1016/S0266-7681(95)80044-1
- Fuchsberger T, Boesch CE, Tonagel F, Fischborn T, Schaller HE, Gonser P. Patient-rated long-term results after complete denervation of the wrist. J Plast Reconstr Aesthet Surg. 2018;71(1):57-61. doi:10.1016/j.bjps.2017.08.014
- Hofmeister EP, Moran SL, Shin AY. Anterior and posterior interosseous neurectomy for the treatment of chronic dynamic instability of the wrist. Hand (N Y). 2006;1(2):63-70. doi:10.1007/s11552-006-9003-5
- Johnson EO, Babis GC, Soultanis KC, Soucacos PN. Functional neuroanatomy of proprioception. J Surg Orthop Adv. 2008;17(3):159-164.
- Patterson RW, Van Niel M, Shimko P, Pace C, Seitz WH Jr. Proprioception of the wrist following posterior interosseous sensory neurectomy. J Hand Surg Am. 2010;35(1):52-56. doi:10.1016/j.jhsa.2009.10.014
- Sgromolo NM, Cho MS, Gower JT, Rhee PC. Partial wrist denervation for idiopathic dorsal wrist pain in an active-duty military population. J Hand Surg Am. 2018;43(12):1108-1112. doi:10.1016/j.jhsa.2018.05.018
- Shim JW, Kim JW, Park MJ. Comparative study between open and arthroscopic techniques for scaphoid excision and four-corner arthrodesis. J Hand Surg Eur Vol. 2020;45(9):952-958. doi:10.1177/1753193420908820
- Soucie JM, Wang C, Forsyth A, et al. Range of motion measurements: reference values and a database for comparison studies. Haemophilia. 2011;17(3):500-507. doi:10.1111/j.1365-2516.2010.02399.x
- Trail IA, Murali R, Stanley JK, et al. The long-term outcome of four-corner fusion. J Wrist Surg. 2015;4(2):128-133. doi:10.1055/s-0035-1549277
- Trumble TE, Rafijah G, Alexander H, Waitayawinyu T. Scaphoidectomy and capsulodesis for SNAC or SLAC stage II. J Wrist Surg. 2012;1(2):129-134. doi:10.1055/s-0032-1329615
- Vanden Berge DJ, Kusnezov NA, Rubin S, et al. Outcomes following isolated posterior interosseous nerve neurectomy: a systematic review. Hand (N Y). 2017;12(6):535-540. doi:10.1177/1558944717692093
- Watson HK, Ryu J. Evolution of arthritis of the wrist. Clin Orthop Relat Res. 1986;(202):57-67.
- Wu CH, Strauch RJ. Wrist denervation: techniques and outcomes. Orthop Clin North Am. 2019;50(3):345-356. doi:10.1016/j.ocl.2019.03.002
