
Zach Husband OMS IV1; Ezra Levy D.O.2; Daniel LeCavalier D.O.2; Michael Janssen D.O.2
1RVUCOM
2Colorado Center for Spine and Orthopedics
DOI: 10.70709/l50pzs3wxv
 Statement of Informed Consent
Statement of Informed Consent
The patient was consented and agreed to publication of this case report.
Keywords: Spine, Revision
Introduction
Cervical total disc replacement (TDR) offers the benefit of motion preservation and reduced adjacent segment degeneration compared to anterior cervical discectomy and fusion (ACDF). TDR is indicated for single- or two-level cervical degenerative disc disease with radiculopathy or myelopathy in otherwise healthy individuals. While mid- and long-term outcomes are generally favorable, delayed hardware complications, though infrequent, can have serious consequences.
Anterior extrusion of cervical TDR components is a documented but uncommon complication. Such failures may be attributed to poor bone integration, undersizing or malpositioning of implants, or underlying biomechanical factors. In symptomatic patients, revision strategies typically include conversion to ACDF, which remains the standard approach. Typical ACDF indications aside from TDR conversion salvage include degenerative disc disease, spinal fractures from trauma, infection and tumors. Surgical Indications are dependent on the type of deformity, neurological compromise, and spinal instability.” 2 TDR failure presenting without symptoms poses a diagnostic challenge and can delay intervention.
This report presents an unusual case of asymptomatic anterior TDR extrusion into the hypopharynx, discovered incidentally, with revision managed through a hybrid construct combining retained TDR and ACDF.
Case Description
A 44-year-old female with a prior history of cervical and lumbar spine surgeries presented with bilateral sacroiliac joint pain and buttock discomfort. Her cervical history included sequential TDR procedures at C6–C7 and C7–T1 without immediate postoperative complications. One year postoperatively, she underwent lumbar spine reconstruction for hardware failure involving L4–L5 partial corpectomy and L5–S1 fixation.
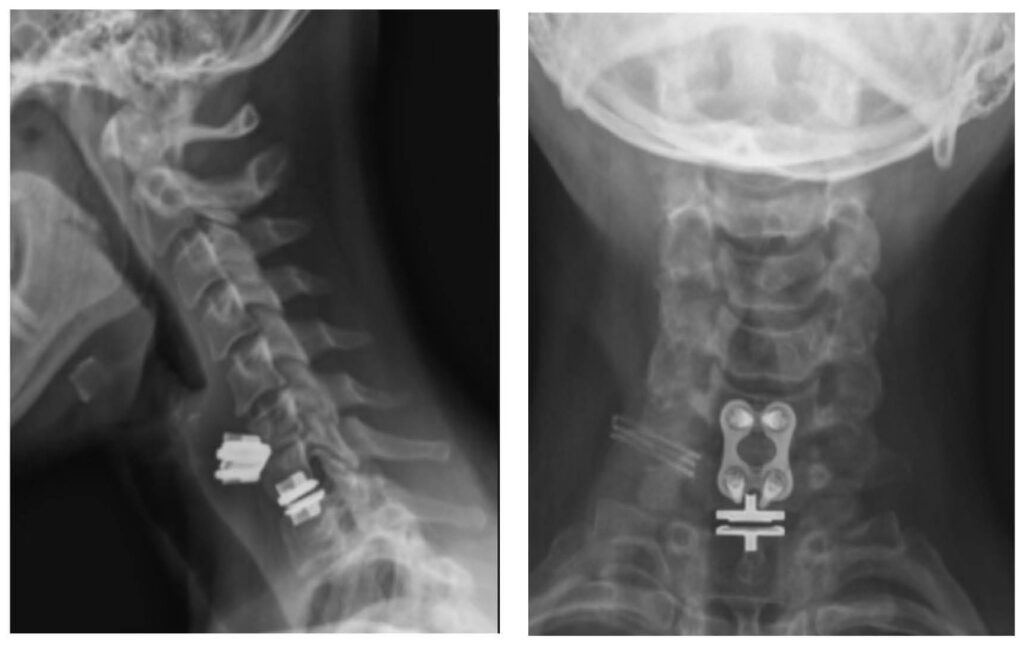
At the current visit, her symptoms were localized to the lumbar spine. She denied dysphagia, odynophagia, neck pain, or neurological deficits. Due to the absence of recent imaging, updated radiographs were obtained to assess the status of prior spinal hardware. These revealed anterior migration of the C6–C7 TDR device, now situated adjacent to the posterior pharyngeal wall. The C7–T1 TDR remained well-seated.
Despite the absence of symptoms, otolaryngology and general surgery consultations were obtained. Given the proximity of the displaced implant to the esophagus and pharynx, surgical intervention was deemed necessary to prevent delayed complications.
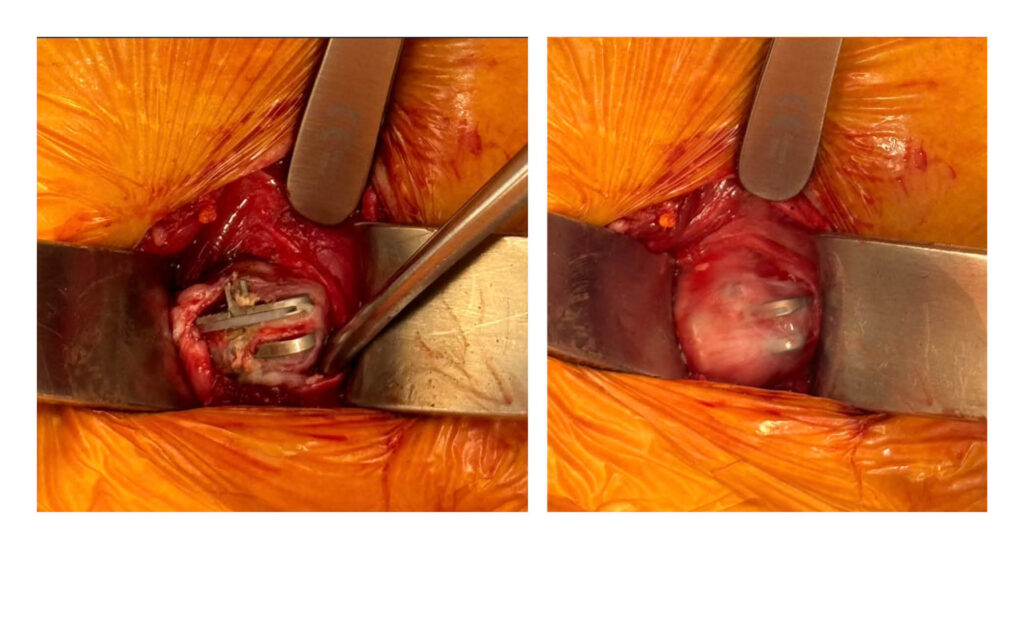
The revision surgery involved anterior exposure through a prior incision. Blunt dissection revealed the extruded disc within fibrous tissue beneath the pharynx. The implant and surrounding mass were excised in two parts. Intraoperative esophagoscopy confirmed no perforation or mucosal breach. The exposed disc space at C6–C7 was reconstructed with a lordotic interbody graft and anterior cervical plating, extending from C6 to C7. The C7–T1 TDR was retained due to its stability and integration.
Postoperative recovery was uneventful. The patient remained asymptomatic, and imaging confirmed successful hardware placement and alignment.

Discussion
Cervical total disc replacement (TDR) is a motion-preserving alternative to anterior cervical discectomy and fusion (ACDF) in appropriately selected patients. TDR has been shown to reduce adjacent segment degeneration and improve early postoperative mobility.1,3 However, implant-related complications—including subsidence, loosening, migration, and, more rarely, complete extrusion—remain significant concerns as TDR procedures become more widespread.
In this case, anterior extrusion of a cervical TDR device into the hypopharynx occurred approximately one year after implantation, with no associated symptoms. While posterior migration into the spinal canal has been described, anterior migration into soft tissue structures such as the pharynx is unusual and poses unique diagnostic and surgical challenges.4,5 The asymptomatic nature of this case highlights the importance of routine surveillance imaging in patients with a history of spinal instrumentation, especially when evaluating unrelated complaints.
Mechanisms of Arthroplasty Failure
Several mechanisms may contribute to TDR failure. Subsidence and endplate violation can result from inadequate implant sizing, poor bone quality, or improper placement.6 Specifically, Lee et al. found that oversized implants relative to preoperative disc height significantly increased subsidence risk. About 23% of patients showed subsidence, with a critical threshold being a pre-op height > 4.5 mm.6
Anterior extrusion may occur if the implant lacks adequate osteointegration, or if excessive motion, distraction, or micromotion prevents stable fusion 3,5 In this case, no dynamic imaging or flexion-extension studies had been performed before implant migration was noted; however, given the implant’s final location, it is likely that early loosening and poor integration played a role.
The Bryan disc, used in this patient, is a semi-constrained device with a polyurethane nucleus between two titanium endplates. While its design facilitates motion and shock absorption, its anterior profile may not provide robust protection against anterior migration once fixation is compromised.3,6 This case adds to existing literature on the limitations of current TDR designs, particularly in segments prone to motion or anatomical challenges such as C6–C7.
Surgical Management and Literature Support
Conversion of a failed TDR to ACDF is well supported in the literature and represents the standard approach for hardware-related complications.2,5 In Carrera et al.’s study of 42 TDR failures, 31 underwent successful conversion to ACDF, reinforcing its utility as a salvage procedure.5 Hybrid constructs, combining retained arthroplasty with adjacent fusion, have also been described in appropriately selected cases and were applied here due to the stability of the C7–T1 TDR.
Intraoperative esophagoscopy and assistance from general surgery were key components of the surgical strategy, given the implant’s location in proximity to the hypopharynx. Fortunately, no mucosal breach was observed, and the procedure was completed without complication. This multidisciplinary approach reflects best practices in managing complex anterior cervical cases with adjacent visceral involvement.
Clinical Significance
Although the case is not unique in terms of surgical approach, it underscores the potential for severe hardware complications to occur silently. The absence of symptoms in the setting of significant implant migration reinforces the need for vigilance, even in asymptomatic patients. As Leven et al. state, clinical significance is best determined by symptomatic pathology, but radiographic findings like those seen here should not be disregarded.3
Conclusion
This case demonstrates the delayed anterior extrusion of cervical TDR hardware into the hypopharynx in an asymptomatic patient, identified incidentally on routine imaging. The revision, performed via conversion to ACDF with retention of a stable adjacent TDR, aligns with current best practices in managing TDR failure. While not a novel surgical construct, this case serves as a reminder of the importance of routine imaging surveillance, careful patient selection for TDR, and awareness of the full spectrum of implant-related complications.
References
- Kim KR, Chin DK, Kim KS, et al. Revision Surgery for a Failed Artificial Disc. Yonsei Med J. 2021;62(3):240. doi:10.3349/ymj.2021.62.3.240
- Verla T, Xu DS, Davis MJ, et al. Failure in Cervical Spinal Fusion and Current Management Modalities. Semin Plast Surg. 2021;35(01):010-013. doi:10.1055/s-0041-1722853
- Leven D, Meaike J, Radcliff K, Qureshi S. Cervical disc replacement surgery: indications, technique, and technical pearls. Curr Rev Musculoskelet Med. 2017;10(2):160-169. doi:10.1007/s12178-017-9398-3
- Carrera DA, Ricks CB. Catastrophic delayed cervical arthroplasty failure: illustrative case. J Neurosurg Case Lessons. 2022;3(11):CASE21731. doi:10.3171/CASE21731
- Blumenthal SL, Ohnmeiss DD, Courtois E, Guyer RD, Zigler JE, Shellock JL. 20. Strategies for addressing failed cervical total disc replacement: a series of 42 patients. North Am Spine Soc J NASSJ. 2024;18:100358. doi:10.1016/j.xnsj.2024.100358
- Lee CY, Tung KK, Tsou HK, et al. Risk Factors for Cervical Disc Arthroplasty Subsidence with Bryan Disc—A Retrospective Observational Analysis. J Clin Med. 2024;13(6):1589. doi:10.3390/jcm13061589
- Mayer R, Rivera J, Chou D, Benzel EC. Indications. In: Revision Lumbar Spine Surgery. Elsevier; 2022:36-43. doi:10.1016/B978-0-323-71201-9.00004-4
- Song KJ, Choi BW, Ham DH, Kim HJ. Prognosis of Hardware-Related Problems in Anterior Cervical Discectomy and Fusion with Cage and Plate Constructs. World Neurosurg. 2020;134:e249-e255. doi:10.1016/j.wneu.2019.10.042
