
Brenden Cutter, DO, PGY-5, Resident; Brendan J. Liakos, DO, Research Fellow; Daniel L. Lara, MD, Research Fellow; Eric G. Huish Jr, DO, Faculty; Marc A. Trzeciak DO, Faculty
Valley Consortium for Medical Education
DOI: 10.70709/87MN-5643
Abstract
Background
The digital mid-axial incision is commonly used in hand surgery. When correctly placed, the proper digital nerves should lie protected in the volar skin flap. The purpose of this study was to evaluate the distance of the digital neurovascular (NV) bundle from a mid-axial incision.
Methods
A standardized mid-axial incision along both sides of each digit was made on five fresh-frozen cadaver hands. The distance from the margin of the incision to the NV bundle was measured at the proximal interphalangeal joint (PIP) and the distal interphalangeal joint (DIP) levels on radial and ulnar sides. The same protocol was performed at the interphalangeal joint (IP) of each thumb.
Results
A total of 90 measurements were taken on five cadaveric hands. In the fingers, the average distance was 3.96 mm from the mid axial incision, with no measurement less than 2.97 mm. This distance was an average of 6.58 mm in the thumb, with no measurement less than 5.98 mm. The NV bundle on the radial side of the fingers was found to be farther from the mid axial incision than those on the ulnar side. The thumb displayed the opposite relationship, with the ulnar side having larger measurements.
Conclusions
The digital nerves of the fingers and thumb are safe during a mid-axial approach, with a safe zone of approximately 3mm in the fingers and 6mm in the thumb. Knowing these anatomic relationships will aid surgeons in safely approaching the digits while minimizing the risk of NV injury.
Keywords: Nerve; hand surgery; mid-axial; mid-lateral; approaches; digital palmar nerve; anatomy; basic science
1.1 Introduction
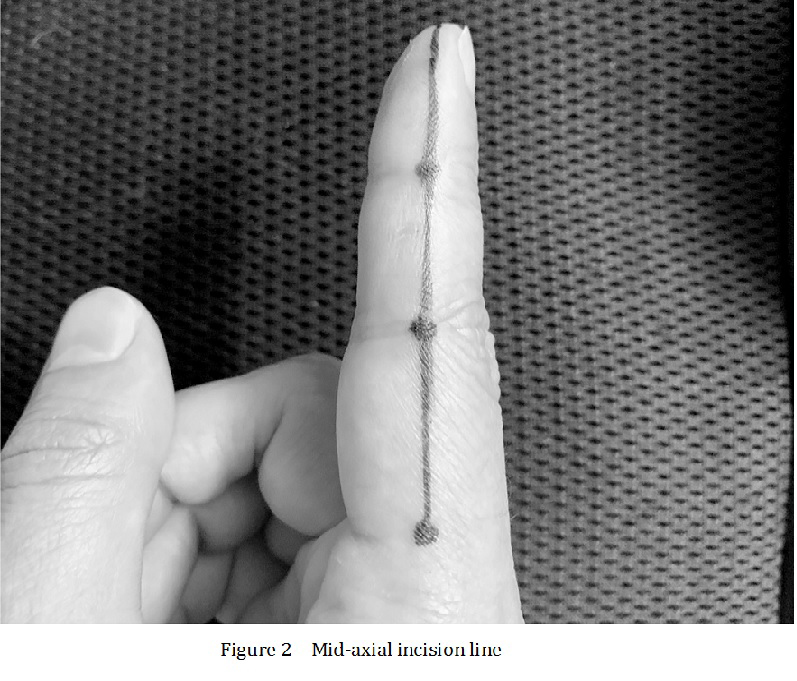
The digital mid-axial incision is a commonly used approach in hand surgery. Popularized by Boyes1, it is useful for a variety of digital pathologies including fracture care, infectious incision and drainage, tendon repair and grafting, contracture releases, and ulnar collateral ligament reconstruction in the thumb.2,3 The incision is made by first flexing the digit and marking the point at each interphalangeal joint where the flexion crease ends (Fig. 1). These points are then connected to identify the mid-axial, or mid-lateral, incision line (Figs. 2-3). Its location on the digit has very little tissue motion, allowing an extensile longitudinal approach without danger of contracture.1,2

A major risk of this approach is transection of the palmar digital neurovascular (NV) structures; however, Green’s Operative Hand Surgery states that when the incision is correctly placed, the proper digital nerves should lie protected in the volar skin flap.2 The fingers are highly specialized to perform a wide variety of tasks, and the preservation of their sensation is extremely important. Surgeons must have a thorough understanding of the anatomy and dangers of this approach, as digital nerves are the most commonly transected nerves in the body. 4
The purpose of our study is to evaluate the location of the proper palmar digital nerve in relation to a digital mid-axial incision line.
2.1 Methods
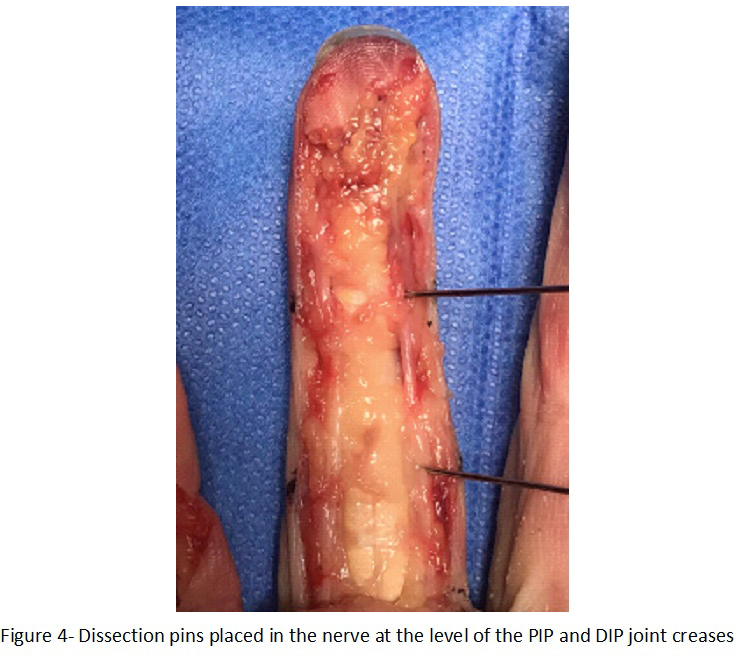
Twenty fingers and 5 thumbs from 5 fresh-frozen human cadaveric hands (3 female and 2 male specimens, without prior injury or surgery) were dissected under loupe magnification. Dissection was performed in a similar fashion to previous anatomic studies evaluating the anatomy of the digital nerves.5 A mid-axial incision was performed on both the radial and ulnar sides of each digit in full extension. The incision line was made by first flexing the digit and marking the point at each interphalangeal joint where the flexion crease ends. These points were then connected to identify the mid-axial incision line (Figures 1 and 2).1,2 The approach was initiated at the metacarpophalangeal (MCP) crease, and continued to the distal tip of each digit (Figure 3). The skin palmar to the incisions was then stripped using sharp dissection, with great care to protect the underlying connective tissue of the deeper structures. The neurovascular bundle, specifically the proper palmar digital nerve, was identified and dissection pins were carefully placed into the nerve at the level of the PIP and DIP joints (Figure 4). A digital caliper (Electronix Express, New Jersey), with accuracy to 0.01 mm, was used to measure the distance from the margin of the incision to the digital nerve at the level of each interphalangeal joint. After initial measurements, we performed a more thorough dissection dorsal to the neurovascular bundle starting from the MCP flexion crease, to evaluate if and where the dorsal branch of the digital nerve crosses the incision. As the thumb is structurally different from the other digits, it was studied separately with the interphalangeal joint (IP) crease as the point of reference.

2.2 Statistical Analysis
Statistical analysis was performed with SPSS version 25 (IBM, Armonk, NY). Distance measurements from the mid-axial incision margin to the neurovascular bundle were evaluated for normality with the Shapiro-Wilk test. Comparison between finger types (thumb, index, long, ring, small) was performed with the Kruskal-Wallis test using the Dunn-Bonferroni method for post-hoc testing. Comparisons of measured distance based on finger side (radial vs. ulnar) and location (PIP vs. DIP) were performed using the Mann-Whitney U test. Statistical significance was set at p < 0.05.
3.1 Results
A total of 80 measurements were taken on the 20 included index, long, ring, and small fingers. The measured distance from the mid-axial incision to the NV bundle was non-parametrically distributed with a median (IQR) distance of 3.96 (3.47 – 4.49) mm. The smallest distance measured at any point was 2.97 mm and the largest was 5.68 mm. An additional 10 measurements were taken on the included thumbs, which displayed a median distance of 6.58 (6.00 – 7.19) mm. The smallest and largest measurements were 5.98 mm and 7.35 mm respectively.
Measured distance from the incision margin to the NV bundle were significantly different between finger types (p < 0.001). Post-hoc analysis showed that the thumb measurements were significantly larger than the index (p = 0.034), long (p = 0.004), ring (p < 0.001), and small (p < 0.001) fingers.
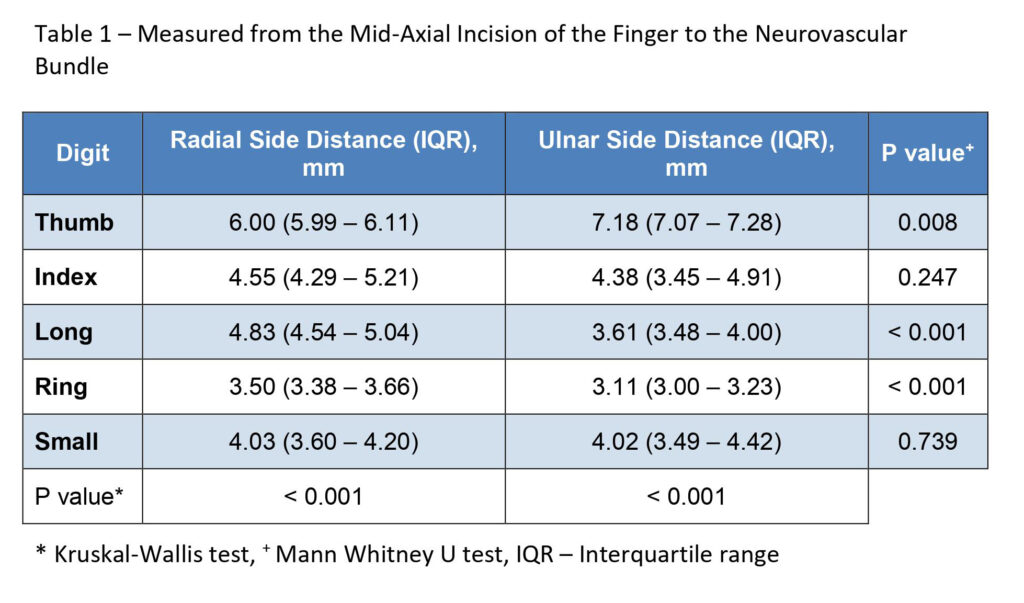
When comparing the location where the measurements were taken in the index, long, ring and small fingers, there were no differences found between measurements at the PIP (4.23 (3.50 – 4.58) mm) vs. the DIP joint creases (3.72 (3.43 – 4.29) mm, p = 0.123). However, measurements taken on the radial side of the fingers were significantly larger than those taken on the ulnar side of the fingers (4.24 (3.63 – 4.66) mm vs. 3.51 (3.17 – 4.33) mm, p = 0.002). Subgroup analysis showed these differences to be present in the long and ring fingers with no differences seen in the index or small fingers. This differed from the thumb, where the ulnar sided measurements (7.18 (7.07 – 7.28) mm) were larger than the radial side (6.00 (5.99 – 6.11) mm, p = 0.008) (Table 1).
The dorsal sensory nerve branched off of the proper digital nerve proximal to the MCP joint flexion crease in all specimens. It did not cross the incision in any of the digits dissected.
4.1 Discussion
The mid-axial incision is a commonly used approach during hand surgery. Basic anatomy of nerves of the hand has been described in textbooks and atlases.2,6-9 Multiple studies have shown this anatomy to be consistent, with the neurovascular bundles being held in place by Cleland’s ligaments dorsally and Grayson’s ligaments palmarly.10,11 According to Wheeless, the digital nerve and artery lie approximately 2 mm volar to the margin of the mid-axial incision, however, we are unaware of any studies that support this claim.12
Our study confirmed that the neurovascular bundle, specifically the proper palmar digital nerve, is safe during a mid-axial incision of the fingers and thumb. All of our measured values were greater than the cited 2mm. The average distance from the mid-axial incision to the NV bundle in the fingers was found to be 3.96mm, with only one recorded value less than 3mm (2.97mm). In regard to the digital nerve of the fingers, the safe zone from the mid-axial incision appears to be approximately 3mm or less.
The thumb was studied separately, where an average distance of 6.58 mm was measured at the IP joint crease, with only one recorded value under 6mm (5.98mm). In regard to the location of the proper palmar digital nerve of the thumb, the safe zone appears to be approximately 6mm or less from the mid-axial incision line.
We chose to record values at the levels of the interphalangeal joint creases because these points were the most reproducible. In addition, multiple authors have stated that the underlying structures are at most risk at these locations, where protective fat is least plentiful.2,13 Our study found no statistical difference in measurements at the PIP and DIP flexion creases. We chose not to measure distances at the level of the MCP flexion crease, as this point cannot be reliably created within the interweb spaces of the digits.
Multiple studies have compared the anatomy of the digital neurovascular bundle of the radial versus ulnar sides.5,6 Zenn et al found no differences between the radial and ulnar sides in regard to the location and degree of branching of the digital nerves.5 Interestingly, our study found a significant difference between the ulnar and radial digital nerves of the middle finger and ring finger, with the ulnar sided digital nerves being closer to the incision than the radial. It is possible that the lumbricals, which run and insert along the radial side of the digits, could play a role in displacing the neurovascular bundle more palmar on this side. Similar to the fingers, there was a significant difference between the distance along the radial and ulnar sides of the thumb. However, this differed in that the radial sided nerves were closer to the incision than those of the ulnar side.
In Green’s Operative Hand Surgery, it is noted that the dorsal sensory branch of the digital nerves can be jeopardized by the mid-lateral approach.2 After initial measurements in the fingers, we performed a more thorough dissection dorsal to the neurovascular bundle in search of the dorsal branch of the digital nerve. We did not find the dorsal sensory branch to cross the incision in any of the specimens. This is consistent with several other studies, which have found the dorsal sensory branch to divide much more proximal than previously believed.14,15 Bas et al found that in 62% of their finger dissections, the dorsal branch divided off the digital nerve at or proximal to the A1 pulley.14 Our study supports that when making a mid-axial approach of the finger, the dorsal sensory branch is not in significant danger.
4.2 Strengths and Limitations
Our study had several limitations. First, the study is limited by a relatively small sample size. Although only five cadavers were dissected, we were able to examine 25 digits with ninety measurements. Second, it is possible that our dissection along the palmar side of the digits may have disrupted the location of the NV bundle. We attempted to minimize this through careful dissection without disturbing the surrounding connective tissue attachments. In addition, all dissections and measurements were made with the digits in full extension, which not only mimicked clinical conditions of making the incision but also held the bundles in a more fixed location.
4.3 Conclusion
Our study confirmed that the digital nerves of the fingers and thumb are safe during a mid-axial approach, with an average distance from the incision of 3.96mm and 6.58mm, respectively. Our findings support a safe zone of approximately 3 mm in the fingers and 6 mm in the thumb. There was no difference between values taken at the PIP and DIP levels. We found a significant difference when comparing sides of the fingers, with the nerves being farther from the incision along the radial side. The thumb also displayed a difference, with the ulnar side having increased distance from the approach. Lastly, we did not find the dorsal sensory branch of the digital nerve to cross the incision in any of the specimens.
5.1 Disclosures
5.2 Conflict of Interest
The authors declare that they have no conflict of interest.
5.3 Funding
No external funding was received for the completion of this study.
5.4 Institutional Ethics Committee Approval
Not-applicable
6.1 References
- Boyes JH. Incisions in the hand. Am J Orthop. 1962 Dec;4:308-11.
- Wolfe S, Hotchkiss R, Pederson W, Kozin S, Cohen M. Green’s operative hand surgery. 7th ed. 2016, Amsterdam, NL: Elsevier; 42.
- Bruser P, Poss T, Larkin G: Results of proximal interphalangeal joint release for flexion contractures: Midlateral versus volar incision. J Hand Surg [Am] 1999, 24:288– 294.
- Buncke HJ. Digital nerve repairs. Surg. Clin. North Am. 1972; 52:1267–85.
- Zenn M. R., Hoffman L., Latrenta G., Hotchkiss R. Variations in digital nerve anatomy. The Journal of Hand Surgery, (1992), 17(6), 1033–1036.
- Wallace WA, Coupland RE. Variations in the nerves of the thumb and index finger. J Bone Joint Surg 1975; 57B:491-4.
- Warwick R, Williams PL. Gray’s anatomy. 35th ed. Philadelphia: WB Saunders, 1973:1040 –1045.
- Tountas CP, Bergman RA. Anatomic variations of the upper extremity. New York: Churchill Livingstone, 1993: 227–241.
- Wilgis EFS, Maxwell P. Distal digital nerve grafts: clinical and anatomic studies. J Hand Surg. 1979; 4:439-43.
- Zwanenburg RL, McGrouther DA, Werker PMN. Grayson ligament: a revised description of its anatomy and function. J Hand Surg Am. 2019 Apr;44(4):341.e1-341.e6.
- Zwanenburg RL, Werker PM, McGrouther DA. The anatomy and function of Cleland’s ligaments. J Hand Surg Eur Vol. 2014 Jun;39(5):482-90.
- Wheeless C. Finger and hand incisions. Wheeless’ Textbook of Orthopaedics. http://www.wheelessonline.com/ortho/finger_and_hand_incisions. Published August 13, 2012. Accessed May 17, 2020.
- Hall RF Jr, Vliegenthart DH. A modified midlateral incision for volar approach to the digit. J Hand Surg Br 1986 Jun;11(2):195-7.
- Bas H, Kleinert JM. Anatomic variations in sensory innervation of the hand and digits. J Hand Surg Am 1999;24:1171-84
- Tellioğlu AT, Ŝensöz Ö. The dorsal branch of the digital nerve: an anatomic study and clinical applications. Annals of Plastic Surgery. 1998;40(2):145-148.
