
1Orthopedic Surgery, Kettering Health Grandview, Dayton, Ohio
Abstract
Giant cell tumors of the tendon sheath (GCTTS) typically present as discrete, solitary nodules along a tendon near the joints in the fingers and toes. Multifocal GCTTS along a single tendon is a rare entity in which only a handful of cases have been described. In this article, we present a case of GCTTS in which four separate lesions along the flexor digitorum profundus (FDP) were surgically removed and then recurred fifteen weeks later on the fifth finger of the same hand. This report characterizes the presentation of a GCTTS, the surgical removal, and the post-operative course for this patient.
Keywords: Multifocal; giant; cell; tumor; tendon; sheath; GCTTS; recurrent
Introduction
Giant cell tumor of the tendon sheath (GCTTS) is the second most common tumor of the hand after ganglion cysts. (1) GCTTS is also the most common form of giant cell tumor1. It is a slow-growing tumor that typically affects individuals between the 3rd and 5th decade of life and is more common in women. (2) Monaghan et al. reported that these most commonly occur on the right over the left, affecting the first, second, and third finger more commonly than the fourth and fifth finger. (3) These present as a painless, subcutaneous swelling, which, if they grow large enough, can cause mass effects on adjacent structures. GCTTS is usually found as a solitary nodule, but there have been a few reported cases of multifocal tumors along the same tendon sheath. (4) This report highlights a patient with recurrent multifocal giant cell tumors along the FDP tendon of the fifth finger.
Case Report
Presentation
A 44-year-old, right-hand dominant woman presented with insidious onset, painless swellings on the volar aspect of the left fifth finger and left forearm. The swelling had appeared two weeks prior to presentation and had been slowly enlarging, with no evidence of infection, no erythema, no edema, and no ecchymosis. She had also begun having numbness in an ulnar distribution of the left hand. There was no history of trauma to the finger or forearm.
On physical examination, there was a 2 cm x 2 cm soft and mobile mass on the volar aspect of the wrist. There was decreased sensation in the ulnar distribution. She had no instability, with 5/5 strength in her hand and wrist with full range of motion. Magnetic resonance imaging (MRI) of the left wrist revealed a cluster of four round, homogeneously enhancing soft tissue masses along the volar and ulnar aspect of the fifth flexor tendon and tendon sheath (Figure 1). Three of the masses appeared in the volar aspect of the proximal wrist, while one was found more distal. The largest of the masses measured 1.6 x 1.1 x 1.5 cm and the smallest measured 0.6 x 0.5 x 0.6 cm. Each mass appeared encapsulated and smooth, lying along the ulnar margin of the fifth flexor tendon sheaths. After a thorough conversation, the patient consented to undergo surgical excision of the masses.
Surgical Removal of GCTTS
A Brunner style incision was made over the mass while identifying and retracting the neurovascular bundles. The mass was noted to be adhered to the flexor tendon sheath (Figure 2). It measured about 1 mm x 1 mm x 1mm in size and was removed along with a small portion of the flexor tendon sheath. Attention was then turned to the forearm masses. Dissection was taken down to the mass through a standard FCR approach. The mass was encountered between the FDS and FDP tendons, with care taken to protect the neurovascular structures. The entirety of the mass was removed and found to be roughly a 4.5 cm x 1 cm x 1 cm oblong, lobulated mass with a yellowish hue. The masses were sent for histopathology, which confirmed the diagnosis of tenosynovial giant cell tumor.
Initial Postoperative Period
Postoperatively, the patient was given a wrist brace to help with the mild postoperative wrist pain. By her two-week follow-up, she had demonstrated a decrease in wrist pain, with her only complaint being some numbness in an ulnar nerve distribution. At her six-week follow-up, the patient presented with increased swelling, pain, and numbness in the ulnar nerve distribution. To treat this conservatively, the patient was enrolled in an occupational therapy program. At 21 weeks postoperation, the patient presented with increased swelling over the middle phalanx of her left fifth finger, and there was concern for a possible recurrence of the GCTTS. MRI at this time revealed a mass measuring 0.4 x 0.7 x 1.0 cm, deep to the flexor tendons of the fifth digit at the level of the mid to distal fifth proximal phalanx; most consistent with a recurrence of GCTTS (Figure 3). After a thorough conversation, the patient consented to undergo surgical excision of the mass.
Surgical Removal of Recurrent GCTTS
Removal of the recurrent GCTTS took place 28 weeks after the initial procedure and was performed in a similar fashion. A Brunner style incision made over the volar aspect of the fifth finger on the left side. The flexor digitorum superficialis (FDS) was vestigial and adherent to the mass, which was approximately 2 x 2 cm. The mass was excised along with the FDS, and the mass was sent off to pathology, which later confirmed a recurrent tenosynovial giant cell tumor.
Second Postoperative Period
The patient progressed well in the early postoperative period with no complaints beyond the expected post-surgical pain. Ten weeks after the second operation, the patient had developed a contracture of the left fifth proximal interphalangeal joint (PIP) and was prescribed therapy to work on improving her range of motion. Eighteen weeks after the second operation, the patient had failed conservative management of her PIP joint contracture and had not seen any progress with her cubital tunnel syndrome from the therapy. At this time, she underwent a left fifth finger PIP joint capsulotomy with a release of the volar plate, and simultaneous cubital tunnel release of the left elbow with neurolysis of the ulnar nerve. The patient’s symptoms improved by her four-week postoperative visit, reporting only mild pain. The patient’s most recent follow-up was 70 weeks after the initial tumor removal and 42 weeks after the surgical excision of the recurrent tumor. Currently, the patient is doing well with no signs of recurrent GCTTS.
Discussion
It is rare to have multifocal GCTTS arising from a single tendon, however there have been other case reports on the entity.(1-12) Novick et al. most recently reported a case in 2023 in which a 34-year-old male presented with two nodules on the flexor pollicis longus tendon (FPL). (5) Park et al. reported a case in which an individual had two separate lesions appear on the FPL tendon seven months apart. (6) Singh et al. reported on a case where five lesions were found intraoperatively. (7) Altaykan et al. reported a case in which two separate lesions were found on the FDS of the fifth finger. (8) Hwang et al. found the most unusual case to date when they found seven separate lesions in the flexor digitorum superficialis tendon of the third finger in a nine-year-old child. (9) Of these reported cases, a majority saw successful excision of the GCTTS, with only a handful of studies reporting any recurrence. (1-12) Current strategies to prevent recurrence include complete excision of the mass, with incomplete excision possibly leading to recurrence. Recurrence can result from mitotic activity within histology, proximity to a joint that is arthritic, and osseous pressure erosion. (10) There was a case reported in 2020 in which a 22-year-old female experienced a recurrence of a GCTTS of the hand via the tendon sheath. In this case, it only took eight months for a mass to reappear, and it continued to grow and become painful. (10) Lesions that appear at separate times and are labeled a recurrence of an isolated GCTTS may represent multifocal etiology to the tumors. One study by Zeinstra et al. demonstrated that multifocal GCTTS can recur after excision. (11) Their patient had multifocal GCTTS of the flexor digitorum superficialis of the third finger at the level of the distal interphalangeal joint and proximal to the wrist that recurred after excision of the primary tumor. (11) Similarly, our case also observed a reoccurrence at 21 weeks postoperation.
The genesis and causes of GCTTS are not fully understood. Still, some explanations include the synovial lining of the joint and tendon sheath producing a reactive overgrowth, an inflammatory response initiated by extensive exposure to antigens or a monocyte/macrophage-producing lesion. (7) GCTTS is characterized by rearrangements of CSF1, a macrophage colony-stimulating factor, which promotes the growth and recruitment of non-neoplastic mononuclear and multinucleated inflammatory cells. (13) This and the shared synovial fluid along a single tendon sheath suggest that these tumor cells could be trapped at multiple points, leading to a multifocal presentation. Once one of these abnormal cells enters the synovial fluid, this can be a nidus to form these tumors. The fact that the tumors form at the narrowest points along the tendon further supports this conjecture. In our case, the patient only noticed the proximal mass on the volar aspect of her wrist but was also found to have masses distally. This may represent the abnormal tumor cells traveling distally from the original mass.
Conclusion
|Multifocal GCTTS along a single tendon is a rare entity, with few cases reported in the literature. When a single tumor is found, further imaging of the entire hand and wrist may reveal other lesions amenable to excision. When possible, complete excision of these tumors should be recommended, with follow-up to assess for recurrence.
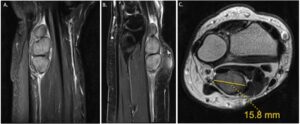
Figure 1: T2 weighted images showing (a) sagittal, (b) coronal and (c) axial views of the masses.

Figure 2: Intraoperative photos showing the multiloculated mass adherent to the FDP tendon in the distal forearm (A-B) with subsequent complete excision (C), and a smaller single mass adherent to the FDP tendon at the level of the proximal phalanx (D)

Figure 3: T2 weighted images showing (a) sagittal, (b) coronal, and (c) axial views of the recurrent mass on the middle phalanx of the fifth finger.
References
- Ozben H, Coskun T. Giant cell tumor of tendon sheath in the hand: analysis of risk factors for recurrence in 50 cases. BMC Musculoskelet Disord. 2019;20(1):457. Published 2019 Oct 21. doi:10.1186/s12891-019-2866-8
- Di Grazia S, Succi G, Fragetta F, Perrotta RE. Giant cell tumor of tendon sheath: study of 64 cases and review of literature. G Chir. 2013;34(5-6):149-152. doi:10.11138/gchir/2013.34.5.149
- Monaghan H, Salter DM, Al-Nafussi A. Giant cell tumour of tendon sheath (localised nodular tenosynovitis): clinicopathological features of 71 cases. J Clin Pathol. 2001 May;54(5):404-7. doi: 10.1136/jcp.54.5.404. PMID: 11328844; PMCID: PMC1731411.
- Ansari MT, Mridha AR, Janardhanan R. Multifocal giant cell tumors of tendon sheath along a single tendon: A case report with review of literature. J Clin Orthop Trauma. 2020;11(4):690-693. doi:10.1016/j.jcot.2020.05.034
- Novick SD, Kahlon P, Berhanu M, Patel P, Uderani M, Saleem F. Multi-Focal Giant Cell Tumor of A Single Tendon Sheath: A Rare Case Report. Cureus. 2023 Apr 15;15(4):e37600. doi: 10.7759/cureus.37600. PMID: 37197098; PMCID: PMC10183790.
- Park JW. Multiple separated giant cell tumors of the tendon sheath in a thumb. J Am Acad Dermatol. 2006;54(3):540-542. doi:10.1016/j.jaad.2005.06.024
- Singh T, Noor S, Simons AW. Multiple localized giant cell tumor of the tendon sheath (GCTTS) affecting a single tendon: a very rare case report and review of recent cases. Hand Surg. 2011;16(3):367-369. doi:10.1142/S0218810411005710
- Altaykan A, Yildiz K, Hapa O, Cukur S. Multifocal giant cell tumor of the tendon sheath occuring at different localizations of the same tendon of a finger: a case report and review of the literature. Eklem Hastalik Cerrahisi. 2009;20(2):119-123.
- Hwang JS, Fitzhugh VA, Gibson PD, Didesch J, Ahmed I. Multiple Giant Cell Tumors of Tendon Sheath Found within a Single Digit of a 9-Year-Old. Case Rep Orthop. 2016;2016:1834740. doi:10.1155/2016/1834740
- Parikh KN, Shah SB. A Multifocal Recurrent Large Giant Cell Tumor of the Tendon Sheath of Flexor Tendon: A Rare Case in the Hand of 22-year-old Female. J Orthop Case Rep. 2020 Aug-Sep;10(5):34-36. doi: 10.13107/jocr.2020.v10.i05.1828. PMID: 33312976; PMCID: PMC7706439.
- Zeinstra JS, Kwee RM, Kavanagh EC, van Hemert WL, Adriaensen ME. Multifocal giant cell tumor of the tendon sheath: case report and literature review. Skeletal Radiol. 2013;42(3):447-450. doi:10.1007/s00256-012-1552-9
- Hitora T, Yamamoto T, Akisue T, et al. Multicentric localized giant cell tumour of the tendon sheath: two separate lesions at different sites in a finger. Br J Dermatol. 2002;147(2):403-405. doi:10.1046/j.1365-2133.2002.484115.x
- Ho J, Peters T, Dickson BC, et al. Detection of CSF1 rearrangements deleting the 3’ UTR in tenosynovial giant cell tumors. Genes Chromosomes Cancer. 2020;59(2):96-105. doi:10.1002/gcc.22807
