
Maria Cecilia Madariaga D.O.; Nicholas A. O’Malley D.O.; M.S., Hannah Groff D.O.; Jeffrey Thompson, D.O.
DOI: http://doi.org/10.70709/anw635mxw
Disclosures
The authors have no conflicts of interest to disclose
Abstract
Background
Burst fractures are a sequela of high-energy spine trauma. While often treated non-operatively, surgery is indicated for neurologic deficits and deformity. Open approaches are the mainstay of treatment; however, percutaneous approaches have become popular. More evidence is needed to establish if percutaneous approaches are equally efficacious and safe compared to open treatment. Thus, the objective of this study was to determine if open or percutaneous approaches were better for treatment of thoracolumbar burst fractures.
Methods
A retrospective review of 40 operatively treated burst fractures was undertaken. Demographic data included age, gender, BMI, Carlson Comorbidity index (CCI), and racial/ethnic background. Injury characteristics collected included mechanism, additional injury, neurologic deficits, evidence of spinal cord injury, traumatic Dural sac laceration, and pre-operative ICU admission. Intra- and post-operative data were also recorded. Chi-square and t-test analyses were used to evaluate the data. Significance was set to p > 0.05.
Results
No differences were noted between open (OPSF) and percutaneous (PPSF) groups with regard to age, BMI, CCI, or racial and ethnic background. There was a higher percentage of females in the PPSF group. There were no differences with regard to injury mechanism or polytraumatic presentation between the groups. The OPSF group had a higher percentage of neurologic deficits. Estimated blood loss (EBL) was significantly lower in the PPSF cohort. No differences existed in perioperative outcomes, discharge disposition, or pain medication use.
Clinical Relevance
OPSF and PPSF have equivalent safety profiles, with PPSF having significantly lower EBL. This suggests that PPSF may be advantageous in polytrauma.
Conclusions/Level of evidence
PPSF and OPSF are equivalent for the treatment of burst fractures. The lower blood loss seen in PPSF may indicate that this approach is better for polytrauma patients. Level of Evidence: 3.
Keywords: Adolescent idiopathic scoliosis, bracing, quality of life, psychological impact
Introduction
Vertebral body burst fractures account for 21-58% of all spinal injuries with the vast majority occurring in the thoracic or lumbar spine.1–3 Thoracolumbar burst fractures occur due to a high-energy, axially-transmitted, traumatic impact to the vertebral column.3,4 Such fractures typically localize in the thoracolumbar (T12-L1) junction. Indications for surgical intervention take into account the presence of neurological symptoms or deficits on physical exam, significant bony retropulsion into the spinal canal with or without concomitant spinal cord injury, degree of injury-induced kyphosis, or disruption to the posterior ligamentous complex.2,5–7 The proportion of operatively managed burst fractures varies significantly based on treatment center and surgeon preference.
Recently, percutaneous fixation has gained popularity with potential benefits including lower blood loss in surgery, shorter surgical time, minimally invasive approach with less soft tissue disruption, reduced pain medication use, and/or accelerated recovery of patients.8–12 Implementation of the percutaneous surgical approach has been reported to maintain the advantages of open surgery (spinal realignment and stabilization) while also shortening the hospital stay and reducing morbidity and mortality.8–10,13,14 In fact, class B recommendations by the Congress of Neurological Surgeons issued in 2019 indicates that percutaneous and open approaches lead to equivalent outcomes.15 However, the literature still lacks significant data comparing open to percutaneous methods. This paper adds to the literature by retrospectively reviewing the experience of spine surgeons at a Level-1 trauma center with percutaneous versus open approaches to manage thoracolumbar burst fractures.
Methods
This study is a retrospective cohort review of patients at a large Level-1 trauma center between 2017 and 2020. Patients were included if they received surgical intervention for diagnosed vertebral compression fractures. Patients were excluded if they were below the age of 17. Baseline patient characteristics, including ethnic background, gender at birth, age and BMI were reviewed and entered into a database. In addition, injury and surgical characteristics were collected. Injury characteristics were defined as mechanism of injury, presence of other injuries, and presence of associated symptoms. Surgical characteristics included approach, estimated blood loss, operative time, post-operative complications, and post-operative analgesic requirements. Data was analyzed using IBM SPSS software. T-test and chi-square tests were used to compare cohorts. Significance was set to p<0.05.
Results
Baseline patient characteristics
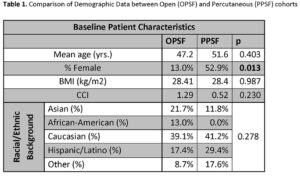
A total of 110 patients with thoracolumbar burst fractures noted on CT were identified. 40 patients met inclusion, having burst fractures managed with either percutaneous surgical fixation (PPSF) or open surgical fixation (OPSF). Overall, there were 28 (70.0 %) males and 12 (30.0%) females with a mean age of 49.7 years. With regard to racial/ethnic background, the total cohort contained 4 (9.8%) African-Americans, 16 (39%) Caucasians, 9 (22.0%) Hispanic/Latinos, 7 (17.1%) Asians, and 4 (9.8%) Other, with no significant differences noted between ethnic groups in the PPSF or OPSF cohorts (p= 0.278). There was a greater percentage of females in the PPSF cohort as compared to the OPSF cohort (52.9% female vs. 13.0%, p= 0.013). No significant differences were noted between the PPSF and OPSF cohorts with regard to mean age (PPSF: 51.6 yrs.; OPSF: 47.2 yrs., p = 0.403), BMI (PPSF: 28.4 kg/m2; OPSF: 28.41 kg/m2, p = 0.987), or CCI (PPSF: 1.29; OPSF: 0.52, p = 0.230). (Table 1)
Injury characteristics
Overall, the mechanisms of injury included 15 (36.6%) motor vehicle accidents, 6 (14.6%) falls, 12 (29.3%) high falls, 7 (17.1%) pedestrian strikes, and 1 (2.4%) other mechanism (Table 2). No significant difference was noted between the proportion of mechanisms between the PPSF and OPSF cohorts. In addition, no significant differences were noted between PPSF and OPSF with regard to polytraumatic presentation. There were no differences in percentage with additional spine injury (PPSF: 41.1% ; OSPF: 21.7%, p= 0.296), percentage with additional orthopedic injury (PPSF: 47.1% ; OSPF: 60.9%, p= 0.523), or percentage with additional non-orthopedic injury (PPSF: 35.3%; OSPF: 56.5%, p= 0.216).
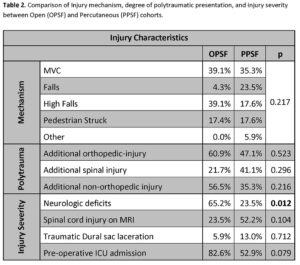
On presentation, patients undergoing OPSF demonstrated a significantly higher proportion of neurologic deficits (OPSF: 65.2%; PPSF: 23.5%, p=0.012). No significant difference was demonstrated between the OPSF and PPSF cohorts with regard to spinal cord injury on MRI (23.5% vs. 76.5%, p= 0.104), or traumatic dural sac lacerations (5.9% vs. 13.0%, p= 0.712). Those with multi-level burst injury (n=15) were treated in equal proportion with OPSF and PPSF (55.5% vs 44.4%, p = 0.608). Those in the OPSF group had a higher proportion of ICU admissions compared to their counterparts in the PPSF group, though this trend was insignificant (82.6% vs. 52.9%, p= 0.079).
Surgical characteristics and Post-operative Outcomes
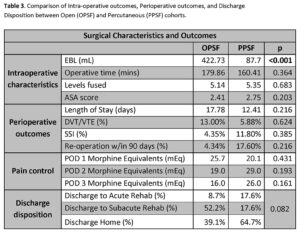
When comparing the PPSF and OPSF cohorts, a significant difference was noted with regard to estimated blood loss, with patients in the PPSF group having lower mean EBL than those in the OPSF cohort (87.7 mL vs. 422.73 mL, p < 0.001). Neither operative time (160.41 mins vs. 179.86, p=0.364), nor number of levels fused (5.35 levels vs. 5.14 levels, p=0.683) significantly differed between the PPSF and OPSF cohorts, respectively. Patients in both groups had a similar mean pre-operative ASA score (2.41 vs. 2.75, p = 0.203).
With regard to post-operative outcomes, the two cohorts remained similar. While statistically insignificant, a higher proportion of patients in the OPSF cohort (52.2%) were discharged to subacute rehab when compared with the PPSF cohort (17.6%)(p=0.082). Additionally, 39.1% of the OPSF cohort and 64.7% of the PPSF cohort were discharged home, and 8.70% of the OPSF cohort and 17.6% of the PPSF cohort were discharged to acute rehab. No significant differences were noted between OPSF and PPSF, respectively, when comparing LOS (17.78 days vs. 12.41 days, p=0.216), in-hospital rates of DVT (13.0 vs. 5.88%, p=0.624), SSI (4.35% vs. 11.8%, p=0.385), or re-operation within 90 days (4.34% vs. 17.6%, p=0.126). No in-hospital mortality was noted in either group.
The use of post-operative pain medication was quantified in morphine equivalents. There were no significant differences noted in mean morphine equivalents between PPSF and OPSF on postoperative day (POD) 1 (25.7 mEq vs. 20.1 mEq, p=0.431), POD 2(29.0 vs. 19.0 mEq, p=0.193), or POD 3(26.0 mEq vs. 16.0 mEq, p=0.161).
Discussion
The treatment of thoracolumbar burst fractures with either open or percutaneous fixation remains a debated subject. Traditional management of unstable burst fractures consists of either an open anterior or posterior approach.6,16 The benefits of an anterior approach include maximal canal decompression and optimal resistance against kyphotic progression. However, an anterior approach in elderly patients or those with multiple medical comorbidities often results in significantly higher morbidity and mortality than in a posterior approach, especially in the lower lumbar levels. Thus, a posterior approach may be preferred for its lower surgical complications. Although a posterior approach raises challenges for complete neural decompression and the risk for kyphotic progression requires a larger fusion, overall outcomes remain similar to an anterior approach.6
Recently, percutaneous techniques have become more popular. Proponents of percutaneous fusion cite reduced blood loss, less disruption of traumatized soft tissue, and decreased post-operative pain and length of stay.17 Authors supporting an open approach often cite ideal kyphotic alignment and VBH. Both open and minimally invasive techniques, however, can achieve adequate fusion, vertebral body height and kyphosis restoration.18,19
Despite the limitations in the amount of literature, our data demonstrates that percutaneous fixation appears to be at least equally efficacious in the treatment of burst fractures. The relatively reduced operative time and significantly reduced blood loss associated with percutaneous fixation are significant advantages in patients with polytrauma. This assertion is further supported by the equal distribution of injury mechanism, neurologic injury, and polytrauma seen in our study’s population. Additionally, PPSF was that fewer patients in this cohort were discharged to rehabilitation facilities, with the majority discharged home. However, this result cannot be considered a true benefit of PPSF as it is likely confounded by the higher rate of neurologic injury observed in the OPSF cohort.
This study has several limitations. First, it is limited by its retrospective nature. In addition, it is limited by its small number of participants. However, when compared to the current literature, this study has a similar number of subjects. This is likely due to the fact that the incidence of burst fractures is quite low.20,21 Despite this, future studies should seek to include a larger number of subjects to ensure a more broadly generalizable sample. A final weakness of this study is its limited follow-up. Thus, while this study demonstrates an important proof-of-concept, studies with long term follow-up are needed to validate our findings. Future studies should include a longer follow-up period to quantify more definitively the differences between PPSH and OPSF.
Conclusions
Thoracolumbar burst fractures are a rare but neurologically threatening sequela of high-energy trauma. When these fractures are operatively indicated, traditional management has included open anterior or posterior approaches. However, minimally invasive techniques have become increasingly popular. Our data suggests that PPSF is equally as safe and efficacious as open procedures, with significantly less blood loss. Thus, it is possible that PPSF is better for polytrauma patients. More research should be done to assess long-term outcomes in these cohorts.
References:
- Tanasansomboon T, Kittipibul T, Limthongkul W, Yingsakmongkol W, Kotheeranurak V, Singhatanadgige W. Thoracolumbar Burst Fracture without Neurological Deficit: Review of Controversies and Current Evidence of Treatment. World Neurosurg. 2022;162:29-35. doi:10.1016/j.wneu.2022.03.061
- Gertzbein SD. Scoliosis Research Society. Multicenter spine fracture study. Spine. 1992;17(5):528-540. doi:10.1097/00007632-199205000-00010
- Bensch FV, Koivikko MP, Kiuru MJ, Koskinen SK. The incidence and distribution of burst fractures. Emerg Radiol. 2006;12(3):124-129. doi:10.1007/s0010140-005-0457-5
- Holmes JF, Miller PQ, Panacek EA, Lin S, Horne NS, Mower WR. Epidemiology of Thoracolumbar Spine Injury in Blunt Trauma. Acad Emerg Med. 2001;8(9):866-872. doi:10.1111/j.1553-2712.2001.tb01146.x
- Abudou M, Chen X, Kong X, Wu T. Surgical versus non-surgical treatment for thoracolumbar burst fractures without neurological deficit. Cochrane Database Syst Rev. 2013;(6):CD005079. doi:10.1002/14651858.CD005079.pub3
- Heary RF, Kumar S. Decision-making in burst fractures of the thoracolumbar and lumbar spine. Indian J Orthop. 2007;41(4):268-276. doi:10.4103/0019-5413.36986
- McAfee PC, Yuan HA, Lasda NA. The unstable burst fracture. Spine. 1982;7(4):365-373. doi:10.1097/00007632-198207000-00007
- Yang WE, Ng ZX, Koh KMR, et al. Percutaneous pedicle screw fixation for thoracolumbar burst fracture: a Singapore experience. Singapore Med J. 2012;53(9):577-581.
- Yanh H, Han D, Li X. Endoscopic Decompression Combined with Percutaneous Pedicle Screw Fixation for Treating Thoracolumbar Burst Fractures with Neurological Deficits: Technical Note and Early Outcomes. World Neurosurg. 2023;173. doi:10.1016/j.wneu.2023.02.088
- Proietti L, Scaramuzzo L, Schirò GR, Sessa S, D’Aurizio G, Tamburrelli FC. Posterior percutaneous reduction and fixation of thoraco-lumbar burst fractures. Orthop Traumatol Surg Res OTSR. 2014;100(5):455-460. doi:10.1016/j.otsr.2014.06.003
- Dhall SS, Wadhwa R, Wang MY, Tien-Smith A, Mummaneni PV. Traumatic thoracolumbar spinal injury: an algorithm for minimally invasive surgical management. Neurosurg Focus. 2014;37(1):E9. doi:10.3171/2014.5.FOCUS14108
- Huang Z, Hu C, Tong Y, et al. Percutaneous pedicle screw fixation combined with transforaminal endoscopic spinal canal decompression for the treatment of thoracolumbar burst fracture with severe neurologic deficit: A case report. Medicine (Baltimore). 2020;99(21):e20276. doi:10.1097/MD.0000000000020276
- Alvine GF, Swain JM, Asher MA, Burton DC. Treatment of thoracolumbar burst fractures with variable screw placement or Isola instrumentation and arthrodesis: case series and literature review. J Spinal Disord Tech. 2004;17(4):251-264. doi:10.1097/01.bsd.0000095827.98982.88
- Trungu S, Ricciardi L, Forcato S, et al. Percutaneous pedicle screw fixation without arthrodesis of 368 thoracolumbar fractures: long-term clinical and radiological outcomes in a single institution. Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc. 2023;32(1). doi:10.1007/s00586-022-07339-z
- Anderson PA, Raksin PB, Arnold PM, et al. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Evaluation and Treatment of Patients with Thoracolumbar Spine Trauma: Surgical Approaches. Neurosurgery. 2019;84(1):E56. doi:10.1093/neuros/nyy363
- Mulcahy MJ, Dower A, Tait M. Orthosis versus no orthosis for the treatment of thoracolumbar burst fractures: A systematic review. J Clin Neurosci. 2021;85:49-56. doi:10.1016/j.jocn.2020.11.044
- McAnany SJ, Overley SC, Kim JS, Baird EO, Qureshi SA, Anderson PA. Open Versus Minimally Invasive Fixation Techniques for Thoracolumbar Trauma: A Meta-Analysis. Glob Spine J. 2016;6(2):186-194. doi:10.1055/s-0035-1554777
- Kocis J, Kelbl M, Kocis T, Návrat T. Percutaneous versus open pedicle screw fixation for treatment of type A thoracolumbar fractures. Eur J Trauma Emerg Surg Off Publ Eur Trauma Soc. 2020;46(1):147-152. doi:10.1007/s00068-018-0998-4
- Chung WH, Eu WC, Chiu CK, Chan CYW, Kwan MK. Minimally invasive reduction of thoracolumbar burst fracture using monoaxial percutaneous pedicle screws: Surgical technique and report of radiological outcome. J Orthop Surg Hong Kong. 2020;28(1):2309499019888977. doi:10.1177/2309499019888977
- Fernández-de Thomas RJ, De Jesus O. Thoracolumbar Spine Fracture. In: StatPearls. StatPearls Publishing; 2023. Accessed January 11, 2024. http://www.ncbi.nlm.nih.gov/books/NBK562204/
- Katsuura Y, Osborn JM, Cason GW. The epidemiology of thoracolumbar trauma: A meta-analysis. J Orthop. 2016;13(4):383-388. doi:10.1016/j.jor.2016.06.019
