
Rachel Keller DO1; Daniel Valdes BS1; Hannah English BS2; Nathan Jones DO1; Christopher Kester DO1
1Philadelphia College of Osteopathic Medicine
2New York Institute of Technology College of Osteopathic Medicine
Abstract
Osteochondritis dissecans (OCD) is a relatively rare disorder affecting subchondral bone and overlying cartilage. It often affects skeletally immature children and adolescents who are involved in activities that involve repetitive overhead movements or axial compression through the elbow. While most OCD lesions occur in the knee, they can also impact the elbow, particularly the capitellum of the distal humerus. The etiology of capitellar OCD is multifactorial, involving genetic predisposition, poor vascularization, and trauma. Early diagnosis, often with CT and MRI, is critical for proper staging and subsequent treatment, which generally ranges from conservative management for stable lesions to surgical intervention for unstable lesions. This article provides a comprehensive review of the anatomy, presentation, diagnosis, treatment, and complications of capitellar OCD lesions.
Key Words: osteochondritis dissecans; OCD; elbow; throwing athlete, gymnast
Introduction
Osteochondritis dissecans (OCD) is a relatively rare disorder that affects subchondral bone. This disorder causes varying degrees of resorption, fragmentation, and sclerosis, which may involve the overlying cartilage.1 While OCD is most commonly found in the knee, it can also affect the elbow, primarily involving the capitellum of the distal humerus.2,3
OCD of the elbow is typically seen in adolescents engaging in repetitive overhead or upper extremity weight-bearing activities, such as baseball, tennis, volleyball, weightlifting, and gymnastics. While the prevalence of this condition is not well established, studies of young baseball players in Japan have shown it to be anywhere from 1.4 – 3.4%.4,5
While the exact cause of capitellar OCD is unknown, its etiology is thought to be multifactorial. Genetic predisposition, poor vascularization, and trauma are all thought to be involved.6 Patients with this condition often have a history of repetitive axial or valgus compression through the radiocapitellar joint. This is supported by the two populations in which this injury is typically observed: baseball players and gymnasts. In baseball players (and other overhead athletes), throwing mechanics, specifically late cocking and early acceleration phases, place high valgus stress and significant compression and shear forces across the immature epiphysis. The impact of these forces through the radiocapitellar joint leads to subchondral flattening, and eventual breakdown and fragmentation of the subchondral bone and overlying cartilage.7,8 While gymnasts do not exhibit the same torsional force of overhead athletes, they do see repetitive, high-impact, forced axial compressions through the elbows in near-full or full extension. 9,10 Interestingly, Kajiyama et al. explored differences between baseball players and gymnasts with capitellar OCD. The authors found that due to these different mechanisms of trauma, capitellar OCD lesions in baseball players were located more anteriorly compared to those seen in gymnasts.11
A high index of suspicion is crucial in preventing a delayed diagnosis of capitellar OCD. Computed tomography (CT) scan and magnetic resonance imaging (MRI) provide the most sensitive findings, especially in the early stages of the condition.12,13 Early determination of lesion stability and integrity of the articular cartilage cap guides treatment, which could range from conservative management (generally, stable lesions) to surgery (generally, unstable lesions).14,15 The following is a current concept review of the anatomy, presentation, diagnosis, treatment, and complications of capitellar OCD lesions.
Anatomy
The elbow serves as an important synovial trochoginglymoid (combination of hinge and pivot) joint in the upper extremity.16,17 It is formed by the articulation between three bones: the distal humerus, the proximal radius, and the proximal ulna. Medially, the ulnohumeral joint is formed by the articulation between the trochlea of the humerus and the trochlear notch, also known as the semilunar notch; on the proximal ulna.16,18 The hinging action of the elbow occurs primarily at the ulnohumeral joint, where the primary flexors, including the biceps brachii, brachialis, and brachioradialis muscles allow for flexion of the elbow. Primary extensors, including the triceps brachii, allow for extension at the elbow. Laterally, the capitellum of the humerus articulates with the proximal radial head to form the radiohumeral joint.16,18A third joint of the elbow is the proximal radioulnar joint, an articulation of the radial head with the radial notch of the ulna. The pivoting action of the elbow occurs primarily at the radiohumeral joint and the proximal radioulnar joint. Here, the primary pronators (pronator teres and pronator quadratus) allow for pronation of the forearm about the elbow, and the primary supinators (supinator and biceps brachii) allow for supination of the forearm about the elbow.16,18
In the anterolateral aspect of the distal humerus, the capitellum is an ellipsoidal-shaped protuberance that is usually directed 30 degrees anteriorly and distally about the long axis of the humerus. Its center of rotation is located 12-15 mm anteriorly to the humeral shaft axis.19-21 The anterior portion of the capitellum is covered by hyaline cartilage. Medially, the capitellum is separated from the trochlea by the trochleocapitellar groove. This groove has a slightly internally rotated orientation in relation to the humeral epicondyles, allowing for approximately 6-8 degrees of valgus tilt in relation to the humeral axis.16,22
The capitellum, as well as the lateral aspect of the trochlea, receives an extraosseous blood supply through posterior perforating vessels. These vessels include the radial recurrent, radial collateral, and interosseous recurrent arteries. Intraosseous blood supply is through posterior condylar perforating vessels.23 Notably, being the first ossification center in the elbow, the capitellum is richly vascularized prior to age 5.24 However, as the capitellum ossifies, its nucleus and growing epiphysis becomes relatively avascular. Any insult that disrupts the small end vessels that supply the capitellum can result in a lack of blood flow and predispose it to subsequent pathologies, including OCD.24
Presentation and Diagnosis
Patients with osteochondritis dissecans of the elbow typically present with insidious onset of pain localized to the lateral aspect of the elbow, often exacerbated by activities that place repetitive stress on the joint. This pain may be accompanied by swelling, stiffness, and decreased range of motion. This rare disorder commonly affects adolescents engaged in overhead or upper extremity weight-bearing sports, such as baseball, tennis, volleyball, weightlifting, and gymnastics.25
The clinical course of capitellar OCD may vary, but initial symptoms often include vague discomfort and a sense of joint instability or ‘locking’. As the condition progresses, patients may experience catching or clicking sensations within the joint, particularly during activities that involve elbow extension and forearm pronation.26 In advanced cases, loose bodies may form within the joint, leading to more pronounced mechanical symptoms and significant functional impairment.
A thorough clinical evaluation should include a detailed history of the patient’s symptoms, sports participation, and any preceding injuries or repetitive activities. The physical examination should assess joint tenderness, range of motion, and the presence of mechanical symptoms such as joint ‘locking’ or ‘clicking.’
Physical examination findings in patients with capitellar OCD may reveal tenderness to palpation over the radiocapitellar joint, joint effusion, and pain during passive range of motion testing, particularly with pronation and supination.26 The diagnosis of capitellar OCD is primarily based on a combination of clinical history, physical examination, and imaging studies. Early and accurate diagnosis is essential to guide appropriate management and prevent long-term joint damage.
Imaging plays a pivotal role in the diagnosis and staging of capitellar OCD. Initial evaluation often begins with standard anteroposterior (AP) and lateral elbow radiographs. Radiographs may reveal subchondral lucency, sclerosis, or loose bodies, indicating the presence of OCD. However, early lesions may not be apparent on plain films. The anterior-posterior radiograph of the elbow in 45 degrees of flexion (APR45 view) occasionally shows displacement of the articular fragment and widening of the gap, suggesting unstable OCD lesions.27 However, plain radiography can underestimate the degree of instability and may not show whether there is displacement of the cartilaginous articular fragment. Therefore, further imaging is necessary to reveal instability and determine the optimal treatment choice.
Coronal, sagittal, and 3D CT images can show the location of free bodies, the size and displacement of the articular fragment, the degree of gap widening, the area of underlying capitellar bone, any cyst formation, and bony spur formation. Precise imaging of OCD lesions along specific tilted planes allows accurate measurement of the articular fragment, gap, and underlying bone, enhancing diagnostic reliability.
MRI is the most sensitive imaging modality for detecting early OCD lesions and evaluating the integrity of the overlying articular cartilage. Coronal and sagittal MRI images can clearly show the three layers of OCD lesions, and fat-suppressed T2-weighted MRI is particularly useful for revealing signs of instability. These signs include separation beneath the articular fragment, fracture of the articular cartilage, widening of the gap between the articular fragment and underlying bone, displacement of the articular fragment, and any articular defects. 27,28 MRI also reveals bony edema of the capitellum and synovitis with a joint effusion. Overall, MRI is recommended as the most helpful tool to show instability, though some OCD lesions may still be underestimated regardless of the imaging modality used.
Various classification systems have been proposed to stage OCD lesions based on imaging findings and arthroscopic evaluation. One commonly used classification system categorizes capitellar OCD lesions into three types based on the integrity of the cartilage and the stability of the bony fragment seen on radiographs:25 (Table 1). Staging is crucial in determining the appropriate management strategy. Generally, stable lesions with intact cartilage may be managed conservatively, while unstable lesions with cartilage disruption or loose bodies may require surgical intervention.
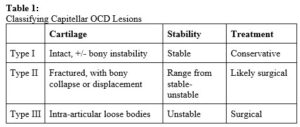
Table 1: Classifying Capitellar OCD Lesions
Treatment
There are a wide variety of treatment options for capitellar OCD. Non-operative management is generally the first-line treatment and has been shown to be more successful in those with open physis, small or stable lesions, short durations of symptoms, and compliance with activity limitations.29 For stable lesions, treatment begins with rest from the sport/activity. Common activities that can lead to development of this condition, and therefore should be avoided during rest periods, include overhead throwing, racket sports, and heavy lifting. Elbow rest for at least six months is the general recommendation for non-operative treatment.30 Non-steroidal anti-inflammatory drugs (NSAIDs) have been reported as beneficial for early symptom management. Physical therapy, starting with gentle stretching and progressing to elbow strengthening, is initiated as symptoms decrease. Some authors have recommended radiographs every six weeks to monitor healing, with repeat MRI performed after six months.30 Immobilization in the form of casting has been reported as well. Cast immobilization has a positive effect on forming firm fibrocartilaginous connections between the articular fragment and the underlying bone, which has the potential to improve healing.15
For unstable lesions or those that fail non-operative management, there are a variety of surgical options available for treatment. Indications for operative intervention include persistent pain, locking, restricted range of motion, presence of loose bodies, displacement, and an articular surface defect, among others. Traditionally, the surgical option of choice was open fragment removal with or without curettage or drilling.30 More recently, fixation of unstable or separated lesions is recommended when possible. This may be performed using pull-out wires, bone peg grafting, screw fixation or bone grafting with dynamic stapling. Though reported success rates vary, approximately 80% of patients have returned to sport at preoperative levels31 and radiographic union has been seen in 82-100% of patients.30 Fracture fixation has been shown to significantly improve outcomes compared to fragment removal alone.32
Drilling and microfracture of lesions can be utilized in both arthroscopic and open approaches. These techniques serve to partially destroy calcified tissue that may have formed, and to create openings into the subchondral bone. Intraosseous blood vessels are damaged/destroyed, causing the release of several growth factors and fibrin clot formation. This influx of growth factors leads to new blood vessel formation and causes marrow cells to aggregate in the lesion defect. Marrow aggregation will then lead to fibrocartilaginous tissue formation and healing at the lesion site.31
Osteochondral autograft transplantation (OAT) is another surgical option for advanced OCD lesions of the capitellum. During OAT procedures, unstable lesions are reconstituted with healthy subchondral bone support and hyaline cartilage taken from a donor site. Multiple donor sites have been used to harvest grafts for this treatment. These include non-weight bearing portions of the proximal lateral femoral condyle, intercondylar notch, and even costal bone and associated cartilage. Although OAT technique has shown promising results, concerns over donor site morbidity (DSM) have limited its widespread use. 31 Also, OAT has shown limited success in lesions that are extensive and those affecting the lateral/central aspect of the capitellum.32 A novel treatment option that was developed to mimic the OAT procedure without the risk of donor site morbidity has been described by Momma et al; as acellular cartilage repair with ultra purified alginate (UPAL) gel implantation. Their study showed 100% of patients demonstrating graft incorporation and normal contour of the subchondral cortex on radiographs. Eighty percent of patients demonstrated excellent functional outcomes, with the remaining 20% demonstrating good clinical results.33 Though these results are promising, further studies are needed.
Arthroscopic treatment of capitellar OCD lesions has become the standard of care for those who have failed conservative treatment. It is a minimally invasive approach that allows direct visualization and fixation of lesions, in addition to early rehab post-op. In an arthroscopic approach, the lesion is first debrided, the bone marrow is stimulated, and any loose bodies or osteophytes are removed.31 Studies have shown up to 82% of patients returned to their pre-injury level of sport with arthroscopic treatment.30 New directions in arthroscopic treatments include substances such as micronized allogeneic cartilage scaffold. This scaffolding is thought to assist in promoting hyaline cartilage formation within the defect, though no clinical studies have been undertaken to date.34
Complications
In general, the majority of patients with capitellar OCDs are eventually pain free and able to fully resume their sport or activity at a similar level to pre-injury.35 Complications of treatment most commonly include recurrent pain, disability, and progression of osteoarthritis. If non-operative treatment is chosen, patient compliance with activity restriction has been directly correlated with failure of treatment and resultant complications.29,36 Progression of arthritis may occur rapidly specifically in radiocapitellar and radioulnar joints resulting in considerable restrictions in elbow range of motion.27 One case of chondrolysis after non-operative treatment was reported in the literature for which a definitive reason was unable to be found.15 Skin irritation from prolonged immobilization with casting or bracing may also occur.
Operative complications tend to differ depending on which treatment approach was chosen; but reoperation for stiffness, recurrent pain, and recurrent loose bodies, were seen across all techniques.37-41 Stiffness requiring arthroscopic synovectomy, capsular release, and occasionally synostosis excision was most commonly encountered when initial treatment was an arthroscopic debridement.42 When osteochondral autograft is chosen, donor site morbidity must be kept in mind. Donor site morbidity (DSM) was defined in most studies as the presence of persistent symptoms after graft harvesting or in any situation where further surgery was needed to treat complications related to the donor site. Andrade et al further specified DSM as effusion, pain, instability during activity, crepitus, stiffness, or development of osteoarthritis43. Knee effusion is the most common complaint at the donor site after harvest, occurring in approximately 13% of patients, and can be effectively managed with intra-articular aspiration of hematoma.44 One study reported one case of pneumothorax after costal graft harvest,45 so extreme care must be taken to prevent this. If the OCD lesion is fixed, complications related to hardware may arise, and radial head irritation from unstable screw fixation has been reported.41 Despite the above complications reported, most patients do very well, regardless of treatment choice.
Conclusion
Capitellar OCDs are relatively rare, and require a comprehensive history and physical examination, appropriate imaging studies, and a high index of suspicion to diagnose and treat in the active adolescent with elbow pain. Conservative treatment remains first line, but a variety of options exist to address these lesions surgically with low complication rates.
Reference List
- Edmonds EW, Polousky J. A review of knowledge in osteochondritis dissecans: 123 years of minimal evolution from könig to the ROCK study group. Clin Orthop. 2013;471(4):1118-1126. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edssjs&AN=edssjs.58F49E56&site=eds-live&scope=site&custid=s6636215. doi:10.1007/s11999-012-2290-y.
- Nissen CW. Osteochondritis dissecans of the elbow. Clin Sports Med. 2014;33(2):251-265. https://www.sciencedirect.com/science/article/pii/S0278591913001269. doi:10.1016/j.csm.2013.11.002.
- Jones KJ, Wiesel BB, Sankar WN, Ganley TJ. Arthroscopic management of osteochondritis dissecans of the capitellum: Mid-term results in adolescent athletes. J Pediatr Orthop. 2010;30(1)8:13. Doi: 10.1097/BPO.0b013e3181c3be83
- Matsuura T, Hashimoto Y, Kinoshita T, et al. Donor site evaluation after osteochondral autograft transplantation for capitellar osteochondritis dissecans. Am J Sports Med. 2019;47(12):2836. doi:10.1177/0363546519871064.
- Kida Y, Morihara T, Kotoura Y, et al. Prevalence and clinical characteristics of osteochondritis dissecans of the humeral capitellum among adolescent baseball players. Am.J Sports Med. 2014;42(8):1963-1971. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=24944293&site=eds-live&scope=site&custid=s6636215. doi:10.1177/0363546514536843.
- Kenniston JA, Beredjiklian PK, Bozentka DJ. Osteochondritis dissecans of the capitellum in fraternal twins: Case report. J Hand Surg Am. 2008;33(8):1380-1383. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edm&AN=34679043&site=eds-live&scope=site&custid=s6636215. doi:10.1016/j.jhsa.2008.05.008.
- Adams JE. Injury to the throwing arm. a study of traumatic changes in the elbow joints of boy baseball players. Calif.Med. 1965;102:127-132. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselc&AN=edselc.2-52.0-76549172210&site=eds-live&scope=site&custid=s6636215.
- Jobe FW, Nuber G. Throwing injuries of the elbow. Clin.Sports Med. 1986;5(4):621-636. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=3768968&site=eds-live&scope=site&custid=s6636215.
- Bojanić I, Ivković A, Borić I. Arthroscopy and microfracture technique in the treatment of osteochondritis dissecans of the humeral capitellum: Report of three adolescent gymnasts. Knee Surg Sports Traum Arthrosc. 2006;14(5):491-496. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edssjs&AN=edssjs.15CF68FA&site=eds-live&scope=site&custid=s6636215. doi:10.1007/s00167-005-0693-y.
- Chan D, Aldridge MJ, Maffulli N, Davies AM. Chronic stress injuries of the elbow in young gymnasts. Br.J Radiol. 1991;64(768):1113-1118. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=1773270&site=eds-live&scope=site&custid=s6636215. doi: 10.1259/0007-1285-64-768-1113.
- Kajiyama S, Muroi S, Sugaya H, et al. Osteochondritis dissecans of the humeral capitellum in young athletes. Orthop J Sports Med. 2017;5(3):1-5. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=cul&AN=122407341&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/2325967117692513.
- Bauer M, Jonsson K, Josefsson PO, Lindén B. Osteochondritis dissecans of the elbow. A long-term follow-up study. Clin Orthop Relat Res. 1992(284):156-160. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=1395286&site=eds-live&scope=site&custid=s6636215.
- Dewan AK, Chhabra AB, Khanna AJ, Anderson MW, Brunton LM. MRI of the elbow: Techniques and spectrum of disease: AAOS exhibit selection. J Bone Joint Surg Am. 2013;95-A(14):e99-13. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edsovi&AN=edsovi.00004623.201307170.00013&site=eds-live&scope=site&custid=s6636215. doi: 10.2106/JBJS.L.01621.
- Kijowski R, De Smet AA. MRI findings of osteochondritis dissecans of the capitellum with surgical correlation. Am.J.Roentgenol. 2005;185(6):1453-1459. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselc&AN=edselc.2-52.0-33644829368&site=eds-live&scope=site&custid=s6636215. doi: 10.2214/AJR.04.1570.
- Takahara M, Uno T, Maruyama M, et al. Conservative treatment for stable osteochondritis dissecans of the elbow before epiphyseal closure: Effectiveness of elbow immobilization for healing. J Shoulder Elbow Surg. 2022;31(6):1231-1241. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselp&AN=S1058274622002658&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/j.jse.2022.01.148.
- Alcid JG, Ahmad CS, Lee TQ. Elbow anatomy and structural biomechanics. Clin.Sports Med. 2004;23(4):503. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=15474218&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/j.csm.2004.06.008.
- Grayson DE. The elbow: Radiographic imaging pearls and pitfalls. Semin.Roentgenol. 2005;40(3):223-247. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselc&AN=edselc.2-52.0-20444480497&site=eds-live&scope=site&custid=s6636215. doi: 10.1053/j.ro.2005.01.013.
- Aquilina AL, Grazette AJ. Clinical anatomy and assessment of the elbow. Open Orthop J. 2017;11:1347-1352. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=29290874&site=eds-live&scope=site&custid=s6636215. doi: 10.2174/1874325001711011347.
- Hoppenfeld S, deBoar P, Buckley R. Surgical Exposures in Orthopaedics: The anatomic approach. 5th ed. Philadelphia: Wolters Kluwer; 2016:Chap 2-3.
- Grant J, Basmajian J. Grant’s Method of Anatomy: A Clinical Problem Solving Approach. 11th ed. Baltimore: Lippincott Williams & Wilkins; 1989:387-406.
- Sabo MT, McDonald CP, Ng J, Ferreira LM, Johnson JA, King GJW. A morphological analysis of the humeral capitellum with an interest in prosthesis design. J Shoulder Elbow Surg. 2011;20(6):880-884. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselp&AN=S1058274611000085&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/j.jse.2011.01.007.
- Suenghwan J, Morrey BF. 46 – distal humerus fractures: Isolated fracture of the capitellum. Morrey’s The Elbow and Its Disorders. 2018:458-465. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselp&AN=B9780323341691000462&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/B978-0-323-34169-1.00046-2.
- Yamaguchi K, Sweet FA, Bindra R, Morrey BF, Gelberman RH. The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am. 1997;79-A(11):1653-1662. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edsovi&AN=edsovi.00004623.199711000.00007&site=eds-live&scope=site&custid=s6636215.
- Eygendaal D, Bain G, Pederzini L, Poehling G. Osteochondritis dissecans of the elbow: State of the art. J ISAKOS. 2017;2(1):47-57. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselp&AN=S2059775421001917&site=eds-live&scope=site&custid=s6636215. doi: 10.1136/jisakos-2015-000008.
- Bruns J, Werner M, Habermann CR. Osteochondritis dissecans of smaller joints: The elbow. Cartilage. 2021;12(4):407-417. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=31113206&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/1947603519847735.
- Maruyama M, Takahara M, Satake H. Diagnosis and treatment of osteochondritis dissecans of the humeral capitellum. J.Orthop.Sci. 2018;23(2):213-219. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=29276039&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/j.jos.2017.11.013.
- Takahara M. Osteochondritis dissecans of the elbow: Recent evolution of pathogenesis, imaging, and treatment modalities. J Shoulder Elbow Surg Int. 2024;8(3):588. doi: 10.1016/j.jseint.2023.09.010.
- Kohyama S, Hara Y, Yamazaki M, Ogawa T, Mamizuka N. A magnetic resonance Imaging–Based staging system for osteochondritis dissecans of the elbow: A validation study against the international cartilage repair society classification. Orthop J Sports Med. 2018;6(9):1-7. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselc&AN=edselc.2-52.0-85054469503&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/2325967118794620.
- Mihara K, Tsutsui H, Nishinaka N, Yamaguchi K. Nonoperative treatment for osteochondritis dissecans of the capitellum. Am.J.Sports Med. 2009;37(2):298-304. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edsovi&AN=edsovi.00000475.200902000.00009&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/0363546508324970.
- Baker III CL, Romeo AA. Osteochondritis dissecans of the capitellum. Am.J.Sports Med. 2010;38(9):1917-1928. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=s3h&AN=60094984&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/0363546509354969.
- Van Bergen CJ, Van Den Ende KI, Ten Brinke B, Eygendaal D. Osteochondritis dissecans of the capitellum in adolescents. WJO. 2016;7(2). doi: 10.5312/wjo.v7.i2.102.
- Takahara M, Mura N, Sasaki J, Harada M, Ogino T. Classification, treatment, and outcome of osteochondritis dissecans of the humeral capitellum: Surgical technique. J Bone Joint Surg Am. 2008;90-A Suppl 2:47-62. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edsovi&AN=edsovi.00004623.200803002.00005&site=eds-live&scope=site&custid=s6636215. doi: 10.2106/JBJS.G.01135.
- Momma D, Onodera T, Kawamura D, et al. Acellular cartilage repair technique based on ultrapurified alginate gel implantation for advanced capitellar osteochondritis dissecans. Orthop J Sports Med. 2021;9(3):1-9. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=cul&AN=149767813&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/2325967121989676.
- Caldwell PI, Auerbach B, DO, Pearson S. Arthroscopic treatment of capitellum osteochondritis dissecans with micronized allogeneic cartilage scaffold. Arthrosc Tech. 2017;6(3):e815-e820. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edsdoj&AN=edsdoj.5b2d9509e1a4dc4a8533a15d5ae479b&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/j.eats.2017.04.007.
- Leal J, Hones KM, Hao KA, Slaton PT, Roach RP. Arthroscopy and microfracture for osteochondritis dissecans of the capitellum in adolescent athletes shows favorable return to sport: A systematic review. Arthroscopy. 2024;40(4):1325. doi: 10.1016/j.arthro.2023.08.075.
- Funakoshi T, Furushima K, Miyamoto A, Kusano H, Horiuchi Y, Itoh Y. Predictors of unsuccessful nonoperative management of capitellar osteochondritis dissecans. Am.J.Sports Med. 2019;47(11):2691-2698. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=31348868&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/0363546519863349.
- Logli AL, Leland DP, Bernard CD, et al. Capitellar osteochondritis dissecans lesions of the elbow: A systematic review of osteochondral graft reconstruction options. Arthroscopy. 2020;36(6):1747. doi: 10.1016/j.arthro.2020.01.037.
- Bexkens R, van den Ende KIM, Ogink PT, van Bergen CJA, van den Bekerom MPJ, Eygendaal D. Clinical outcome after arthroscopic debridement and microfracture for osteochondritis dissecans of the capitellum. Am.J.Sports Med. 2017;45(10):2312-2318. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=mdl&AN=28520461&site=eds-live&scope=site&custid=s6636215. doi: 10.1177/0363546517704842.
- Bae DS, Ingall EM, Miller PE, Eisenberg K. Early results of single-plug autologous osteochondral grafting for osteochondritis dissecans of the capitellum in adolescents. J Pediatr Orthop. 2020;40(2):78-85. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselc&AN=edselc.2-52.0-85040660393&site=eds-live&scope=site&custid=s6636215. doi: 10.1097/BPO.0000000000001114.
- Lewine EB, Miller PE, Micheli LJ, Waters PM, Bae DS. Early results of drilling and/or microfracture for grade IV osteochondritis dissecans of the capitellum. J Pediatr Orthop. 2016;36(8):803-809. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselc&AN=edselc.2-52.0-84996538505&site=eds-live&scope=site&custid=s6636215. doi: 10.1097/BPO.0000000000000575.
- Nishinaka N, Yamaguchi K, Uehara T, Nagai S, Atsumi T, Tsutsui H. Costal osteochondral autograft for reconstruction of advanced-stage osteochondritis dissecans of the capitellum. J Shoulder Elbow Surg. 2014;23(12):1888-1897. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselc&AN=edselc.2-52.0-84926677163&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/j.jse.2014.06.047.
- Mclaughlin RJ, Leland DP, Bernard CD, et al. Both debridement and microfracture produce excellent results for osteochondritis dissecans lesions of the capitellum: A systematic review. Arthroscopy, Sports Medicine, and Rehabilitation. 2021;3(2):e593. doi: 10.1016/j.asmr.2020.10.002.
- Andrade R, Vasta S, Pereira R, et al. Knee donor-site morbidity after mosaicplasty – a systematic review. J Exp Orthop. 2016;3(1):1-17. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edssjs&AN=edssjs.5C7DF7A3&site=eds-live&scope=site&custid=s6636215. doi: 10.1186/s40634-016-0066-0.
- Yamagami N, Yamamoto S, Aoki A, Ito S, Uchio Y. Outcomes of surgical treatment for osteochondritis dissecans of the elbow: Evaluation by lesion location. J Shoulder Elbow Surg. 2018;27(12):2262-2270. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edselp&AN=S1058274618306062&site=eds-live&scope=site&custid=s6636215. doi: 10.1016/j.jse.2018.08.011.
- Shimada K, Tanaka H, Matsumoto T, et al. Cylindrical costal osteochondral autograft for reconstruction of large defects of the capitellum due to osteochondritis dissecans. J Bone Joint Surg Am. 2012;94-A(11):992-1002. https://search.ebscohost.com/login.aspx?direct=true&AuthType=sso&db=edsovi&AN=edsovi.00004623.201206060.00006&site=eds-live&scope=site&custid=s6636215. doi: 10.2106/JBJS.J.00228.
