
Hanna Brancaccio BA; Ryan St. John MS; Usmaan Al-Shehab MS; Seth Spicer MS; Timothy Gelatt BS; Noah Ivak BA; James Bailey DO
Rowan-Virtua School of Osteopathic Medicine, Futures Forward Research Institute
Abstract
Background
Extracorporeal shockwave therapy (ESWT) has been used as a novel treatment approach for trigger finger, a common condition caused by inflammation of the flexor tendons of the finger and thumb. Trigger finger can lead to significant hand dysfunction and is one of the leading causes of hand pain. ESWT is a conservative treatment modality that has been gaining popularity due to its low associated risks and high success shown in treating a variety of tendinopathies. To date, ESWT has been employed for the treatment of trigger finger, but its efficacy as a treatment option has not yet been proven.
Purpose/Hypothesis
The purpose of this study is to determine the impact of ESWT on functional outcomes and pain scores when used as a treatment for trigger finger.
Study/Design
A systematic review and meta-analysis were conducted with strict adherence to PRISMA 2020 guidelines.
Methods
Five online databases (PubMed, Web of Science, Embase, Scopus, Cochrane) were searched using MeSH key terms to identify studies. Included in the analysis were randomized controlled and non-controlled trials and retrospective cohort studies that utilized ESWT as the sole treatment for trigger finger and reported mean Quick-DASH (qDASH) or Visual Analog Scale (VAS) scores pre- and post-intervention. Two studies, evaluating 40 fingers, met the inclusion criteria for analysis of qDASH, and four studies, evaluating 108 fingers, met the inclusion criteria for analysis of VAS. qDASH scores were compared between baseline and 6 months after treatment to represent the magnitude of disability and symptoms.3 VAS scores were compared between baseline and 7±5 months after treatment to represent pain.
Results
Statistical analysis was performed using a single group meta-analysis with a random effects approach using IBM SPSS Statistics. This approach allowed for the effect sizes of individual studies to be pooled for collective evaluation of mean changes in qDASH and VAS scores between baseline and follow up. A p-value less than 0.05 was utilized to determine statistical significance. The extent of improvement in scores was represented by the pooled and individual effect size (Cohen’s d) with 95% confidence intervals (95% CI [LL, UL]). For qDASH scores, a large common effect size (Cohen’s d =-1.61 95% CI [-3.45, 0.23]) with considerable heterogeneity (I2 = 0.916) was found, suggesting a substantial treatment effect despite underlying variability in study parameters. However, the p-value was found to be 0.09, suggesting that decreases in qDASH scores 6 months after ESWT treatment (i.e., improvement in magnitude of disability and symptoms) were statistically insignificant. Statistically significant decreases in VAS scores were found (p<0.05) between baseline and 7±5 months after treatment, representing an improvement in pain. A large common effect size (Cohen’s d = -4.74 95% CI [-8.80, -0.68] with considerable heterogeneity (I2 = 0.985) was found, suggesting a large reduction in pain despite underlying variability in study parameters.
Conclusion
ESWT has demonstrated a large benefit for the treatment of pain associated with trigger finger. Although the effect on functionality (as quantified by qDASH) was statistically insignificant, future randomized controlled trials and high-quality studies are needed to reconcile these findings. A limitation in this study was the number of included studies and the sample sizes utilized to analyze ESWT effects on qDASH and VAS. A larger sample size would make the findings more generalizable and provide greater insight into the effects of ESWT on functional outcomes. An increased number of studies would allow researchers to complete regression-based statistical analyses.
Keywords: Trigger finger, ESWT, therapy, shockwave, tendinopathy
Introduction
Stenosing tenosynovitis, colloquially known as trigger finger (TF), is a common condition caused by inflammation of the A1 pulley sheaths surrounding the flexor tendons in the fingers and thumb (1). Stenosis of the pulleys leads to surrounding inflammation and potential formation of a nodular tendon that prevents gliding through the sheath upon finger extension (2). This condition can lead to significant hand dysfunction and is one of the leading causes for hand pain. Trigger finger affects 2-3% of the population and up to 10% of all diabetic patients (3).
The diagnosis is typically made based on medical history and a clinical exam, which commonly reveals a popping sound accompanied with pain during finger flexion and extension (4). Treatments include corticosteroid injections, splinting, oral NSAIDS, and physical therapy. Surgery is performed after all conservative treatment options have been exhausted (5). Extracorporeal shock wave therapy (ESWT) is an emerging treatment option for trigger finger. This therapy has the potential to alleviate the socioeconomic impacts associated with long recovery times and potential complications of surgery (6).
ESWT is available as a low-risk treatment for a wide range of tendinopathies with a success rate ranging from 65 to 91 percent (7). The basis of ESWT is the delivery of shockwaves, which are a form of a pressure wave that consist of both positive and negative phases in their waveform. These differing waveform phases interact with different tissue types based on their densities (8). The exact mechanisms of ESWT on tissue are not completely understood; however, it appears to play a role in inducing the regeneration of tissues on a cellular level and destruction of calcification due to mechanotransduction and release of various cell mediators (9).
Focused and radial ESWT are types of ESWT that can be used for the treatment of trigger finger. Focused ESWT generates maximum pressure when the specific depth in the body tissue is achieved, targeting deeper tissues. Radial ESWT which generates a more superficial result by employing a widespread pressure field (8). Frequency is another parameter that may be altered when utilizing ESWT. Current literature shows that frequencies of up to 8 Hz are used. Changing the frequency to a lower value can help to alleviate pain felt upon receiving the treatment (9).
ESWT has shown high success in treating various tendinopathies, but there are no existing reviews that quantify its efficacy in the treatment of trigger finger. The goal of this systematic review and meta-analysis is to determine how ESWT affects pain and functional outcomes in patients with trigger finger.
Methods
A systematic review and meta-analysis were conducted with strict adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines to evaluate pain scores and functional outcomes in patients who received ESWT as a treatment for trigger finger. This review was not registered on PROSPERO and was exempt from Institutional Review Board approval.
Search Procedure
A comprehensive review of five major scientific databases was conducted in search of studies that reported on the use of ESWT for trigger finger. On February 26, 2024, PubMed, Web of Science, Embase, Scopus, and Cochrane were queried for all available articles with no limitations on the date of publication.
MeSH was utilized to identify key terms, which were subsequently applied to Boolean operators. The search string utilized was: (“shockwave” OR “extracorporeal shockwave” OR “extracorporeal shock wave therapy” OR “ESWT” OR “shockwave therapy” OR “shock wave therapy”) AND (“trigger finger” OR “trigger finger disorder” OR “trigger digits” OR “trigger digit” OR “flexor tendon entrapments” OR “flexor tendon entrapment” OR “snapping finger” OR “snapping fingers”). Google Scholar was manually searched, which yielded no novel literature. This search yielded 75 records, which were imported into Rayyan.ai to detect and remove duplicates using the 99% match “Detect Duplicates” function. There were 45 duplicates detected and removed, resulting in 30 remaining studies for screening of inclusion and exclusion criteria. Titles and abstracts were independently screened by two authors (HB and RSJ) which led to the exclusion of 24 articles. The remaining 6 articles were subjected to full-text appraisal by the same two reviewers.
Inclusion and Exclusion Criteria
Articles selected for inclusion in the analysis were randomized controlled and non-controlled trials and retrospective cohort studies that utilized ESWT as the sole treatment for trigger finger and reported mean Quick-DASH (qDASH) or Visual Analog Scale (VAS) scores pre- and post-intervention. Case reports and case series, cadaveric studies, animal studies, studies without an English translation, studies without full-text availability, and studies without full-data availability were excluded. Studies were not excluded based on country of origin, date, or language of origin. Six studies were reviewed in their entirety; one study was eliminated due to data being reported as median instead of mean and one study was eliminated due to lack of full-text availability. For the remaining four studies, two authors extracted the relevant data to be used for statistical analysis.

Risk of Bias and Certainty of Evidence Assessment
Outcomes included in analysis were appraised for certainty of evidence utilizing the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria (11). The GRADE criteria and explanation for any decisions to downgrade the quality of evidence are detailed in the summary of findings chart, which was adopted from GRADEpro GDT (Table 1, Table 2) (12).
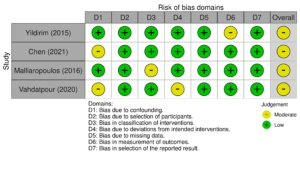
Bias in included articles was assessed using metrics designed for their specific study type. To encompass the included study designs, ROBINS-I was employed (13, 14). A description of the domains and the respective determinations for each study are included in Figures 6 and 7, which were generated using robvis (15).
Results
Two studies, evaluating 40 fingers, met the inclusion criteria for analysis of qDASH, and four studies, evaluating 108 fingers, met the inclusion criteria for analysis of VAS. qDASH scores were compared between baseline and 6 months after treatment to represent the magnitude of disability and symptoms. VAS scores were compared between baseline and 7±5 months after treatment to represent pain.
Statistical analysis was performed using a single group meta-analysis with a random-effects approach using IBM SPSS Statistics for Windows, version 29 (IBM Corp., Armonk, N.Y., USA). This approach allowed for the effect sizes of individual studies to be pooled for collective evaluation of mean changes in qDASH and VAS scores between baseline and follow up. A p-value less than 0.05 was utilized to determine statistical significance. The extent of improvement in scores was represented by the pooled and individual effect size (Cohen’s d) with 95% confidence intervals (95% CI [LL, UL]).
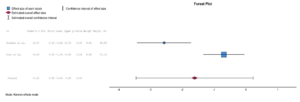
qDASH scores of 38 patients with trigger finger were analyzed across two randomized controlled trials before and after treatment with EWST under a random-effects model. Effect size pooling revealed a statistically insignificant decrease in DASH scores (Cohen’s d=-1.61, p=0.09) (Figure 2).
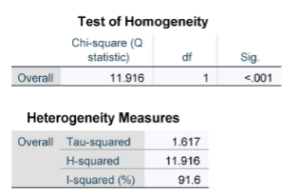
Considerable heterogeneity between the two studies was revealed by an I2 value of 91.6. Homogeneity testing also reveals the null hypothesis of homogeneity to be rejected (X2(1, N=2) =11.916, p<0.001 (Figure 3).
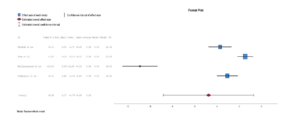
VAS scores of 106 patients before and after EWST across four randomized controlled trials were analyzed under a random-effects model. Effect size pooling demonstrated a statistically significant decrease in VAS scores after ESWT (Cohen’s d = -4.74, p=0.02) (Figure 4).
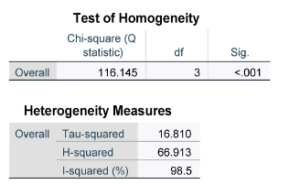
Considerable heterogeneity between the four studies was revealed by an I2 value of 98.5. Homogeneity testing also reveals the null hypothesis of homogeneity to be rejected (X2(3, N=4) =116.145, p<0.001 (Figure 5).
Risk of Bias and Certainty of Evidence Assessment
GRADE analysis revealed an overall low quality of evidence for both qDASH and VAS. High heterogeneity contributing to inconsistency and a small sample size contributing to imprecision lowered the certainty of evidence across both outcomes. Other factors that are considered for upgrading quality of evidence (i.e., large effect size, dose-response gradient, and plausible confounders that would have reduced effect size) were not applicable (Table 1, 2).


The Risk of Bias assessment revealed a moderate risk of bias in all four of the included studies that were evaluated using ROBINS-I (Figure 5, 6). Yildirim et al. was found to have moderate risk of bias in measurement of outcomes because there is no information on whether outcome assessors were aware of the intervention that participants received (16). Chen et al. was found to have moderate risk of bias due to confounding because the study allowed concomitant treatment with NSAIDs, but the frequency and dosage of NSAIDs were not recorded during patient follow-up (17). Malliaropoulos et al. was found to have moderate risk of bias in the classification of interventions because treatment sessions took place weekly until the pain subsided for each individual participant and varying bars of ESWT were used depending on individual pain tolerance (18). Vahdatpour et al. was found to have moderate risk of bias due to confounding due to varying comorbidities and deviations from the intended intervention due to no available information (19). However, the risk of bias across these domains was not enough to substantially lower confidence in the results of the study, hence the decision to score risk of bias in the GRADE analysis as “not serious.”

Discussion
This systematic review and meta-analysis provide the most up-to-date information on the use of ESWT for trigger finger and the impact this treatment modality has on functional outcomes and pain scores. As of February 2024, the efficacy of ESWT as a treatment option for trigger finger has not been proven.
The analysis demonstrated that ESWT had an insignificant impact on qDASH scores. Individually, the two clinical trials included in the analysis demonstrated a significant improvement in qDASH scores six months after treatment with ESWT (16,17). The small number of trials included in the analysis could explain the lack of significance; however, the large effect size points to the practical effect that ESWT can have on improving functionality in patients with trigger finger. Some propose that the functional effect ESWT has on trigger finger is due to the inhibition on the thickening of the flexor tendon and pulley sheaths (20). Additionally, ESWT involves a stimulator effect, which enhances the cascade involved in cellular regeneration, neovascularization, and the release of growth hormone factor to promote the healing process (21). More randomized controlled trials are necessary to reconcile the findings of this study and determine if ESWT has a significant impact on improving functionality.
This analysis also demonstrated a significant decrease in VAS scores. A clinical trial conducted by Yildirim et al. showed that ESWT can produce similar therapeutic benefits when compared to corticosteroids, highlighting a valuable noninvasive treatment option for patients that cannot tolerate steroid injections (16). The exact etiology of trigger finger and the physiologic action of ESWT are unknown. Some suggest that ESWT modulates pain through various mechanisms: decreasing substance P release in the treated area, selectively addressing the loss of unmyelinated nerve fibers, reducing calcitonin-related peptide expression in the dorsal root ganglia, and activating the serotonergic system (22).
Variation in energy density levels and frequency could have an impact on the efficacy of ESWT. Currently, there is no definitive protocol for the administration of ESWT for the treatment of musculoskeletal disorders. The randomized controlled trial conducted by Chen et al. compared a high energy group, low energy group and a sham group to each other in the treatment of trigger finger. The high energy group showed a significant reduction in pain and qDASH scores compared to the sham group six months post-ESWT treatment (17). Another study examining the treatment of chronic heel pain showed significant results in pain reduction and functional improvements in the maximally tolerated energy density group compared to a fixed energy density group (23). Further research is required to assess how varying energy density levels affect treatment outcomes associated with ESWT.
Limitations
Overall, there were some limitations in this study. The initial search was confined to PubMed, Embase, Scopus, Cochrane Library, and Web of Science; therefore, relevant studies indexed on other scientific databases and data from gray literature may have been overlooked. The limited number of clinical trials and the small sample size used to analyze the effects of ESWT on qDASH and VAS scores were major limitations contributing to high heterogeneity, statistical insignificance, and low certainty of evidence. A larger sample size would make these findings more generalizable and improve our understanding of the effects of ESWT on functional outcomes. Moreover, the significant heterogeneity among the included studies might have influenced the aggregated results of the meta-analysis.
It is also important to note that the included studies did not follow a standardized protocol. The study designs varied in impulse frequencies, pressures, and numbers of ESWT sessions. The studies had differing criteria for which grade of trigger finger was to be included. There were other inconsistencies present, such as the use of concomitant treatment modalities and patients with comorbidities. However, this highlights an important opportunity for clinical researchers and physicians to design and implement research studies that isolate each of these variables to create a comprehensive narrative regarding ESWT and trigger finger.
Future Directions
Future research should seek to include a larger number of patients to ensure that the findings can be applied to a wider and more diverse population of patients. Additionally, more randomized controlled trials should be designed to compare qDASH scores pre- and post-ESWT treatment. Studies should also investigate the effects of different ESWT energy densities on functional outcomes and pain scores. An increased number of studies would allow researchers to complete regression-based statistical analyses
Conclusion
While ESWT has been shown to improve functional outcomes and pain scores in trigger finger, only VAS scores were statistically significant. ESWT can be an efficient noninvasive treatment option for trigger finger. More randomized controlled trials are essential to mitigate the impact of confounding variables and confirm the effects of ESWT in the treatment of trigger finger.
References
- Jeanmonod R, Harberger S, Tiwari V, et al. Trigger Finger. [Updated 2024 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459310/
- Merry SP, O’Grady JS, Boswell CL. Trigger Finger? Just Shoot!. J Prim Care Community Health. 2020;11:2150132720943345. doi:10.1177/2150132720943345
- Johnson E, Stelzer J, Romero AB, Werntz JR. Recognizing and treating trigger finger. J Fam Pract. 2021;70(7):334-340. doi:10.12788/jfp.0239
- Vasiliadis AV, Itsiopoulos I. Trigger Finger: An Atraumatic Medical Phenomenon. J Hand Surg Asian Pac Vol. 2017;22(2):188-193. doi:10.1142/S021881041750023X
- Matthews, Amber PA-C, MPAM; Smith, Kristen PA-C, MPAM; Read, Laura PA-C; Nicholas, Joyce PhD; Schmidt, Eric PhD. Trigger finger: An overview of the treatment options. Journal of the American Academy of Physician Assistants 32(1):p 17-21, January 2019. | DOI: 10.1097/01.JAA.0000550281.42592.97
- Ferrara PE, Codazza S, Maccauro G, Zirio G, Ferriero G, Ronconi G. Physical therapies for the conservative treatment of the trigger finger: a narrative review. Orthop Rev (Pavia). 2020;12(Suppl 1):8680. Published 2020 Jun 26. doi:10.4081/or.2020.8680
- Wang, CJ. Extracorporeal shockwave therapy in musculoskeletal disorders. J Orthop Surg Res 7, 11 (2012). https://doi.org/10.1186/1749-799X-7-11
- van der Worp H, van den Akker-Scheek I, van Schie H, Zwerver J. ESWT for tendinopathy: technology and clinical implications. Knee Surg Sports Traumatol Arthrosc. 2013;21(6):1451-1458. doi:10.1007/s00167-012-2009-3
- Schroeder, Allison N. MD1; Tenforde, Adam S. MD2; Jelsing, Elena J. MD3. Extracorporeal Shockwave Therapy in the Management of Sports Medicine Injuries. Current Sports Medicine Reports 20(6):p 298-305, June 2021. | DOI: 10.1249/JSR.0000000000000851
- Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: An R package and Shiny app for producing PRISMA 2020‐compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Systematic Reviews. 2022;18(2). doi:https://doi.org/10.1002/cl2.1230
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from guidelinedevelopment.org/handbook.
- GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University and Evidence Prime, 2024. Available from gradepro.org
- Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan AW, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JPT. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016; 355; i4919; doi: 10.1136/bmj.i4919.
- Littell JH, Gorman DM, Valentine JC, Pigott TD. PROTOCOL: Assessment of outcome reporting bias in studies included in Campbell systematic reviews. Campbell Syst Rev. 2023;19(2):e1332. Published 2023 May 25. doi:10.1002/cl2.1332
- McGuinness, LA, Higgins, JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Syn Meth. 2020; 1- 7. https://doi.org/10.1002/jrsm.1411
- Yildirim P, Gultekin A, Yildirim A, Karahan AY, Tok F. Extracorporeal shock wave therapy versus corticosteroid injection in the treatment of trigger finger: a randomized controlled study. J Hand Surg Eur Vol. 2016;41(9):977-983. doi:10.1177/1753193415622733
- Chen YP, Lin CY, Kuo YJ, Lee OK. Extracorporeal Shockwave Therapy in the Treatment of Trigger Finger: A Randomized Controlled Study. Arch Phys Med Rehabil. 2021;102(11):2083-2090.e1. doi:10.1016/j.apmr.2021.04.015
- Malliaropoulos N, Jury R, Pyne D, et al. Radial extracorporeal shockwave therapy for the treatment of finger tenosynovitis (trigger digit). Open Access J Sports Med. 2016;7:143-151. Published 2016 Oct 31. doi:10.2147/OAJSM.S108126
- Vahdatpour B, Momeni F, Tahmasebi A, Taheri P. The Effect of Extracorporeal Shock Wave Therapy in the Treatment of Patients with Trigger Finger. Open Access J Sports Med. 2020;11:85-91. Published 2020 Mar 9. doi:10.2147/OAJSM.S232727
- Dogru M, Erduran M, Narin S. The Effect of Radial Extracorporeal Shock Wave Therapy in the Treatment of Trigger Finger. Cureus. 2020;12(6):e8385. Published 2020 Jun 1. doi:10.7759/cureus.8385
- Wang CJ, Wang FS, Yang KD, et al. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J Orthop Res. 2003;21(6):984-989. doi:10.1016/S0736-0266(03)00104-9
- De la Corte-Rodríguez H, Román-Belmonte JM, Rodríguez-Damiani BA, Vázquez-Sasot A, Rodríguez-Merchán EC. Extracorporeal Shock Wave Therapy for the Treatment of Musculoskeletal Pain: A Narrative Review. Healthcare (Basel). 2023;11(21):2830. Published 2023 Oct 26. doi:10.3390/healthcare11212830
- Chow IH, Cheing GL. Comparison of different energy densities of extracorporeal shock wave therapy (ESWT) for the management of chronic heel pain. Clin Rehabil. 2007;21(2):131-141. doi:10.1177/0269215506069244
