1Rahmani R, 1Eaddy S, 2Stegelmann S, 1Skrobot G, 1Miller R, 1Andreshak T
1Mercy Health St. Vincent Medical Center, Toledo, OH, USA; 2Medical City Denton, Denton, TX, USA
BACKGROUND
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a potentially devastating complication after surgery. Spine surgery is associated with an increased risk of postoperative bleeding, such as spinal epidural hematomas (SEH), which complicates the use of anticoagulation. Despite this dilemma, there is a lack of consensus around perioperative VTE prophylaxis. This systematic review investigates the relationship between chemoprophylaxis and the incidence rates of VTE and SEH in the elective spine surgical population.
METHODS
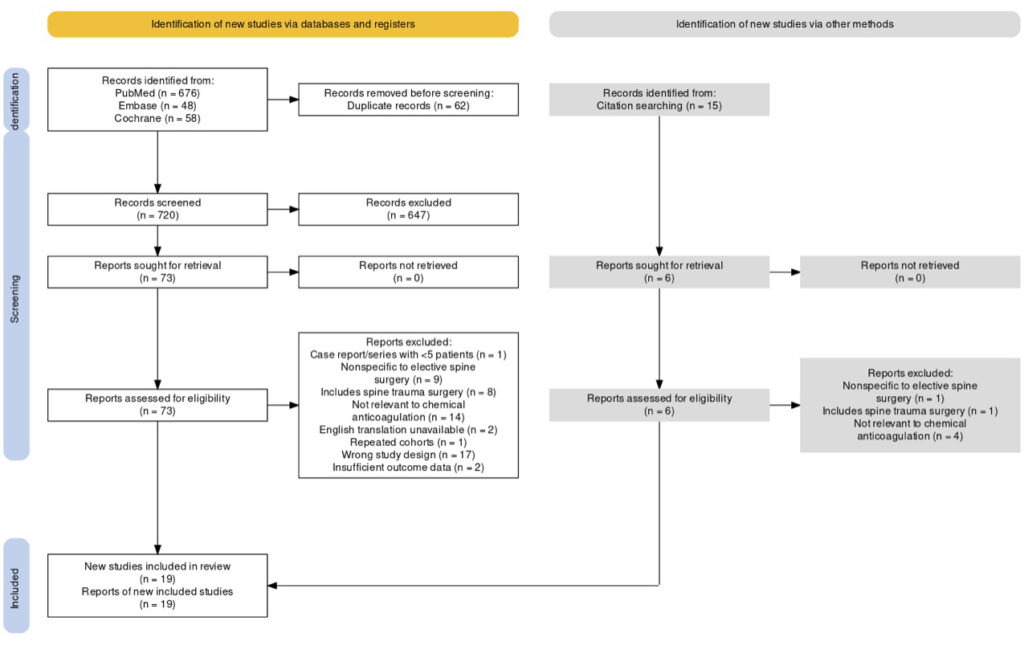
A comprehensive literature search was performed using the PubMed, Embase, and Cochrane databases to identify studies published after 2000 that compared VTE chemoprophylaxis use in elective spine surgery. Studies involving patients aged <18 years or with known trauma, cancer, or spinal cord injuries were excluded. Pooled incidence rates of VTE and SEH were calculated for all eligible studies, and meta-analyses were performed to assess the relationship between chemoprophylaxis and the incidences of VTE and SEH.
RESULTS
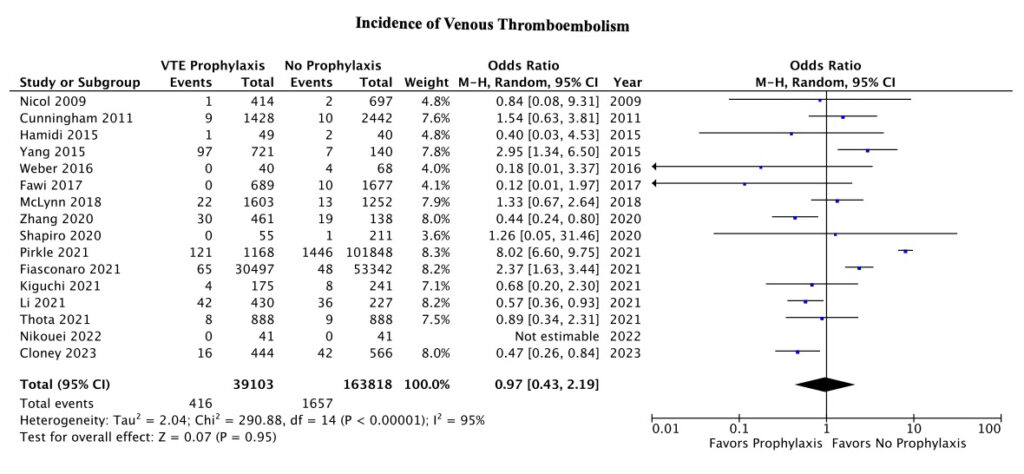
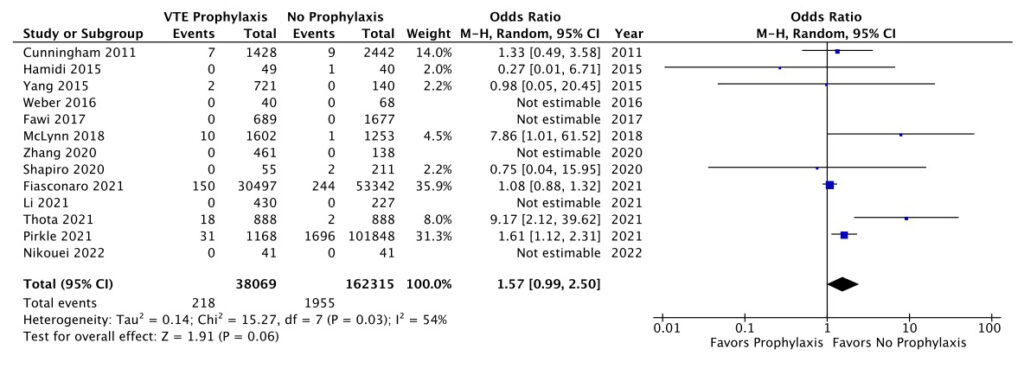
Nineteen studies met our eligibility criteria, comprising a total of 220,932 patients. The overall pooled incidence of VTE was 3.2%, including 3.3% for DVT and 0.4% for PE. A comparison of VTE incidence between patients that did and did not receive chemoprophylaxis was not statistically significant (OR 0.97, P = 0.95, 95% CI 0.43 – 2.19). The overall pooled incidence of SEH was 0.4%, and there was also no significant difference between patients that did and did not receive chemoprophylaxis (OR 1.57, P = 0.06, 95% CI 0.99 – 2.50).
CONCLUSION
The use of perioperative chemoprophylaxis may not significantly alter rates of VTE or SEH in the elective spine surgery population. This review highlights the need for additional randomized controlled trials to better define the risks and benefits of specific chemoprophylactic protocols in various subpopulations of elective spine surgery.