1McDermott M, 2Rebic A, 1Bayaton A, 3Barner K, 1Patel A
1Duly Health and Care, Naperville, IL, USA; 2Kettering Health Dayton, Dayton, Ohio, USA; 3KCU/ Research Medical Center, Kansas City, USA
Introduction
Restoration of sagittal alignment is understood to be a primary objective when performing lumbar fusion surgery. Lordotic cages and posterior osteotomies may be applied in various ways to achieve lordosis. Anterior Column Reconstruction (ACR) via release of the anterior longitudinal ligament (ALL) has been reported to obtain up to 30° of lordosis correction at a single intervertebral level. ACR can be combined with a Smith-Peterson osteotomy (SPO), which may cause a large sagittal correction. The primary purpose of this study is to evaluate the change in lumbar alignment after ACR with and without an SPO.
Methods
This is a retrospective review of a single center’s ACR cases from 2015-2023. All patients who had undergone a transpsoas ALL release and placement of a hyperlordotic cage were included in this study. Preoperative, immediate postoperative AP and lateral radiographs were collected and analyzed for sagittal alignment parameters and ACR segmental angle change.
Results
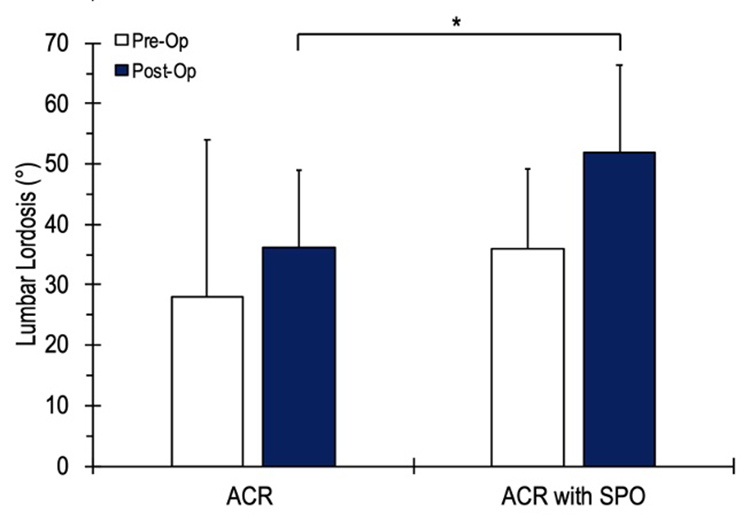
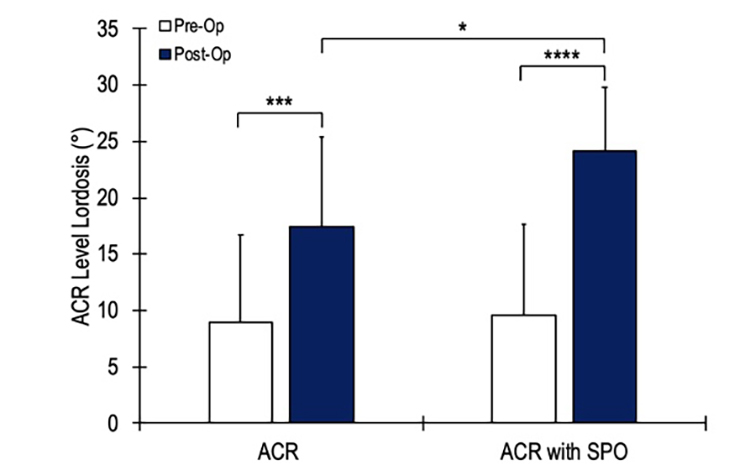
27 patients with a mean age of 68.2 ± 8.7 years were enrolled in the study. Nineteen of the patients underwent ACR alone, and eight patients underwent ACR with an SPO. The average lumbar lordosis (LL) was 30.5 ± 18.1° and the mean preoperative PI-LL mismatch was 27.2 ± 9.9°. Patients who underwent a combined ACR with SPO had an average postoperative LL of 51.8 ± 12.9°, which was significantly higher than the ACR group (36.1 ± 14.6°, p = 0.02) (figure 1). The average postoperative PI-LL mismatch for the ACR + SPO group was 10.6 ± 7.7 compared to 20.9 ± 14.6 for the ACR group (p = 0.07). The ACR + SPO group demonstrated a postoperative segmental angle change of 14.5 ± 5.0° at the ACR level, which was significantly higher than the ACR group (7.6 ± 6.3, p = 0.03) (figure 2).
Conclusion
ACR with SPO is a powerful tool for the restoration of sagittal alignment; as it has improved lumbar lordosis, PI-LL mismatch, and segmental level correction more than ACR alone.