1Lin C, 2Qureshi I, 1Richardson M, 1Anil U, 1Egol K
1NYU Langone Orthopedic Hospital, New York, New York, United states; 2New York Institute of Technology College of Osteopathic Medicine, Mount Sinai, New York, United states
Introduction
Morbidity and mortality of geriatric hip fracture patients remains high. Increased time from hospital admission to hip fracture surgery is a factor that has been associated with increased risk of postoperative adverse outcomes. The purpose of this study was to identify factors associated with delays to surgery greater than 1 day in geriatric hip fracture patients. We aim to identify and compare comorbidities between patients who underwent surgery within 1 day and those who did not.
Methods
Patients over the age of 65 who underwent a surgical repair for a hip fracture from 2005 to 2019 were identified from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. Patients were grouped into those who had surgery less than 1 day after admission (n = 74,072) and those who had surgery greater than 1 day after admission (n = 21,481). Demographic data and comorbidities were collected and compared. Multivariate linear regression models were used to assess the effect of comorbidities on risk of surgery more than 1 day after admission, adjusting for confounding variables such as age, sex and BMI.
Results
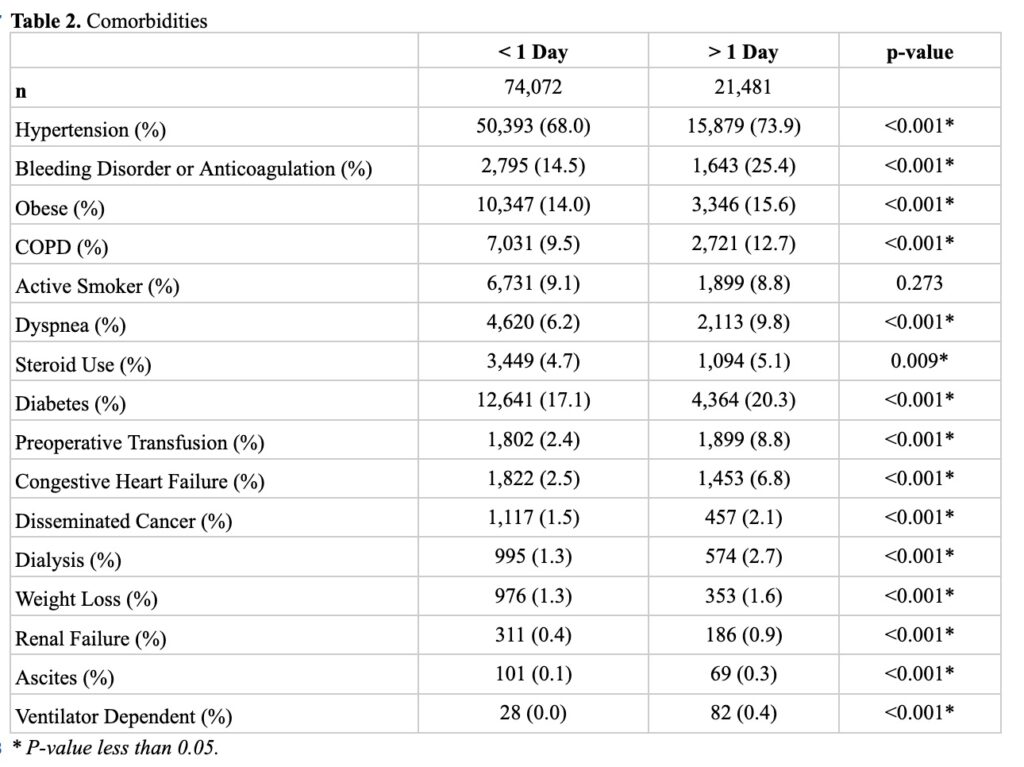
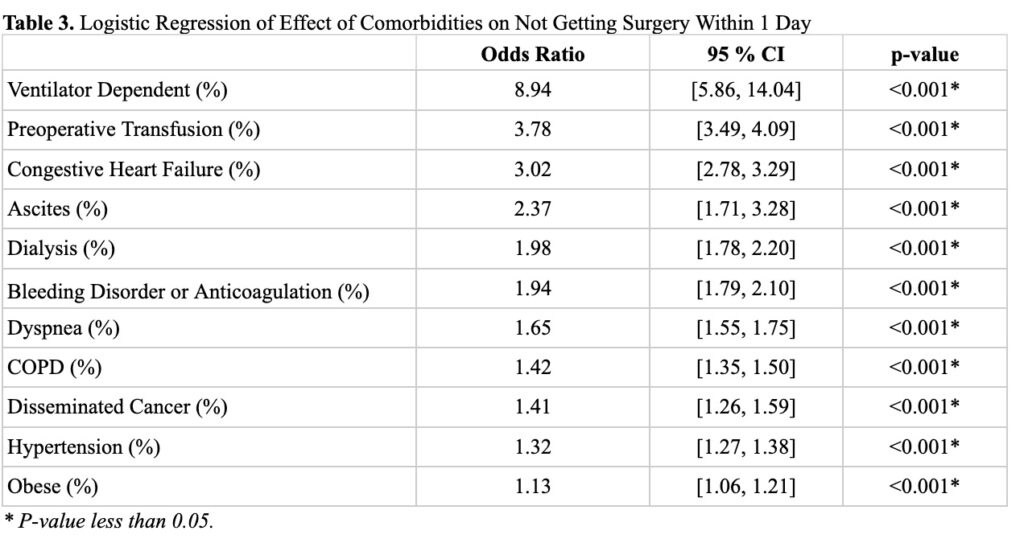
Hip fracture patients who did not get surgery within 1 day were older, more likely to be male, non-white, have lower functional status and greater ASA class (Table 1). These patients had significantly greater preoperative comorbidities such as hypertension, bleeding disorder or anticoagulated status, obesity, COPD or CHF (Table 2). Patients who were ventilator dependent (OR: 8.94; 95% CI: [5.86, 14.04], p < 0.001), had preoperative transfusions (OR: 3.78; 95% CI: [3.49, 4.09], p < 0.001) or CHF (OR: 3.02, 95% CI: [2.78, 3.29], p < 0.001) had the greatest odds of not having surgery within 1 day (Table 3).
Conclusions
There was a significant difference in preoperative comorbidity status between hip fracture patients who did and did not get surgery within 1 day. Patients with certain comorbidities such as ventilator dependence, need for preoperative transfusion and congestive heart failure have greater odds of having surgery outside of 1 day. Particular attention should be placed on patients who arrive with these risk factors and clinical pathways should be designed in order to expedite preoperative medical optimization and surgical treatment.
![]()