
Greg Colbath, MD1; Joseph Bell, DO2; Liam Ortega, DO3; Logan Druessel, DO3; Stephan Pill, MD4
1Medical Group of the Carolinas-Orthopedics-Skylyn, Spartanburg Regional Healthcare System, Spartanburg, South Carolina, USA
2Franciscan Health, Olympia Fields, Illinois, USA
3Mercy Health St. Vincent Medical Center, Toledo, Ohio, USA
4Steadman Hawkins Clinic of the Carolinas, Prisma Health, Greenville, South Carolina, USA
DOI: 10.70709/9uhhtcjhk6
Abstract
We describe the case of a 65-year-old female who presented with worsening left hip pain after a high-energy fall. Subsequent imaging demonstrated a large fluid collection in the lateral thigh consistent with a Morel-Lavallée lesion. After initial drainage and compression therapy failed to alleviate her swelling and discomfort, she was taken to the operating room for endoscopic irrigation and debridement. An incisional negative pressure dressing was used post-operatively. The patient had rapid resolution of pain and return to activities. Morel-Lavallée lesions can be successfully managed with a minimally invasive endoscopic technique. This may be less traumatic to the involved soft tissues, lower the risk for post-operative infection, and improve cosmesis compared with open debridement.
Keywords: Morel-Lavallée; degloving; endoscopy; negative pressure dressing; arthroscopic
Introduction
A Morel-Lavallée lesion (MLL) is a closed degloving injury of the soft tissue caused by post-trauma sequelae. The force shears the skin and hypodermis from the underlying fascia, creating a potential space for fluid to accumulate. Complications may occur within this space, such as formation of necrotic adipose tissue and infection.1 When the presence of MLL is suspected, diagnosis can be confirmed with ultrasound or MRI.2,3
No standardized guidelines exist for managing MLLs. While percutaneous drainage and compression are often utilized initially, surgical intervention is the definitive treatment. Open evacuation and debridement of necrotic material has traditionally been the procedure of choice; however, endoscopic debridement has also been described.4,5
This case report describes a MLL that was treated successfully with endoscopic debridement and a post-operative incisional negative pressure dressing. This reduced the patient’s hospital stay and allowed for a rapid return to activities.
Statement of Informed Consent
The patient was informed that data concerning the case would be submitted for publication, and she provided consent.
Case Presentation
Patient is a 65-year-old female who sustained an injury to her left hip after falling from a boat and experiencing a shearing force between the boat and the dock. She presented to the orthopedic office 15 days after injury complaining of pain and immense swelling of the lateral aspect of her left hip and thigh. An ultrasound-guided aspiration was performed at initial presentation, which yielded 200cc of serosanguinous fluid. A left hip MRI with and without contrast was obtained 5 days after aspiration and revealed a 20x10cm fluid-filled collection, with a thin rim, along the lateral aspect of the left iliotibial band. The synovial and hematogenous products with central re-accumulation was consistent with a MLL (Fig. 1). Repeat ultrasound-guided aspiration yielded 200cc of serosanguinous fluid one week after initial aspiration, 22 days after injury. She was afebrile with no erythema or draining sinus noted.

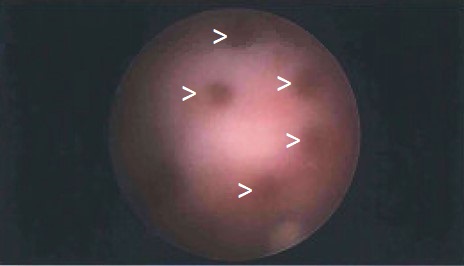
On day 31 post-injury, due to persistent swelling and discomfort, the patient underwent left hip endoscopic debridement. The patient was positioned in the right lateral decubitus position. Serosanguinous fluid (35cc) was aspirated, and no obvious infection was noted. Superolateral and distal mid-lateral portals were marked 3cm from the greater trochanter and incised. An endoscope was advanced to the hypodermis-fascial interface over the iliotibial band. Evacuation of hematoma and debridement of deep dermal tissue was performed with the endoscopic shaver. Several punctate holes were made with a arthroscopic biter, in a transportal fashion, along the entirety of the IT band to assist with seroma decompression and initiate scarring along the space (Fig. 2). Dynamic evaluation redemonstrated external snapping deep to the iliotibial band at the vastus ridge of the greater trochanter. Therefore, the iliotibial band was endoscopically released with cautery in a cruciform fashion. Liposomal bupivacaine (60cc) was injected along the portal sites and surrounding soft tissue and tranexamic acid (TXA, 1 gram in 10cc dilution) was injected along the lateral IT deep layer for additional hemostasis. A 10x40cm negative pressure wound dressing (PICO, Smith and Nephew, Memphis, TN) was placed over the lateral thigh following primary closure with nylon sutures. Compression bandages were also placed to help reduce the recurrence of dead space.
Post-operatively, the patient was weight-bearing with crutches for two weeks. At her three-week post-operative visit, she reported having minimal pain and resumed pre-injury activity levels. She continued to be pain-free and active without limitations at her final twenty-one-week follow-up. Her left hip showed no signs of soft tissue swelling recurrence and adequate incision healing (Fig. 3).

Discussion
Morel-Lavallée lesions most commonly occur in the pelvic and thigh region following trauma with a shearing force. There is rapid onset swelling and progressive decreased mobility in subsequent days. Tseng and Tornetta reported 1.7% of patients with a pelvic fracture had a concomitant MLL. 6 The reported incidence may be underdiagnosed due to the association with pelvic fractures.
Previous studies reported that acute and subacute (<3 weeks) MLLs that are not encapsulated may be successfully treated conservatively. Conservative treatment includes compression bandaging, US-guided aspiration, with sclerotherapy utilized when a second aspiration is needed. Conservative treatment often fails when a pseudocapsule forms and prevents fluid reabsorption.1 Nickerson et al.7 showed that >50 mL aspiration of fluid had an 83% risk of recurrence and suggested this as a surgical indication. The patient in this case had an initial aspiration of 200cc at 15 days post-injury with recurrence requiring a second 200cc aspiration seven days later.
Surgical intervention most commonly utilizes an open drainage and debridement followed by second-intention healing of the wound rather than primary-intention. Though open surgical debridement is a successful definitive treatment, there is an increased risk of morbidity and prolonged course of healing. Hak et al.8 reported an infection rate of 13% in 24 patients with pelvic MLL who were treated with open debridement. The patient in this case underwent endoscopic debridement combined with a negative pressure wound dressing applied after primary closure of portal sites with the aim to prevent secondary seroma formation. The negative pressure wound dressing was removed seven days after surgery. Compression bandages were also utilized to approximate the dermis and fascia in order to facilitate tissue healing.
TXA (1 gram in 10cc dilution) was injected along the lateral IT deep layer as a measure for additional hemostasis. The goal was to prevent recurrence of the MLL, which would likely necessitate an additional surgery for the patient. In a systematic review by Ausen et al.9, local TXA administration has been shown to drastically reduce post operative bleeding after soft tissue surgery. TXA has also been shown to reduce hematoma formation after breast surgery.10 Although there is a paucity in the literature regarding local TXA use to prevent recurrence of an MLL, these other studies have shown the effectiveness of this treatment in the prevention of serosanguinous fluid collection in dead space after soft tissue surgery in other areas of the body.
The surgical repair of MLL utilizing endoscopic techniques has only been published in five other instances. Kim et al.4 utilized endoscopic debridement and doxycycline injection with subsequent washout after 30 minutes as being effective in a 14-year-old boy with a chronic MLL of the lower leg. The drains were removed at two weeks when < 5mL of daily fluid was collected. Walls et al.5 had a patient with a large septic MLL that was not responsive to initial conservative treatment. Following the utilization of an endoscopic debridement, two drains were removed on day five and inflammatory lab values returned to normal within one-week post-operation. Koc et al.11 described endoscopic debridement with fibrin glue injection in a 33-year-old professional soccer player with a MLL of the knee after conservative management failed. Drain was removed after one week with < 20mL of daily fluid was collected. Leng et al.12 followed up on Liu et al.13, showing 38 patients that they successfully treated with endoscopic debridement and added percutaneous cutaneo-fascial sutures with elastic skin tubes to close the space without the use of sclerotherapy. The sutures were removed after 3 weeks. Kage et al.14 showed a patient that failed conservative treatment and underwent arthroscopic debridement of their MLL. Negative pressure wound therapy was used along with 2 drainage catheters removed around 3 weeks later.
In this case, we shared the commonality with the previous cases of endoscopic debridement. Additionally, punctate micro-trauma was created in the subcutaneous fascia and IT band to stimulate natural tissue healing that was minimally invasive and avoided the potential adverse effects of sclerotherapy. The use of the incisional wound vac created an active suction that prevented fluid from reaccumulating within the potential space and was discontinued after a total of seven days. Our case is unique in that we used an incisional wound vac, without the additional use of drains, to assist with wound closure. Each case that utilized the endoscopic debridement technique shared the definitive resolution of MLL without recurrence.
Conclusion
The endoscopic management of MLL of the lateral hip is a potential alternative to open surgery when conservative treatment fails. The patient in our case had minimal post-operative pain, an excellent outcome, low morbidity, and a rapid return to her prior activity levels. This is the first time we have reported endoscopic debridement using punctate decompression method and incisional wound vac.
References
- Greenhill D, Haydel C, Rehman S. Management of the Morel-Lavallee Lesion. Orthop Clin North Am. 2016;47(1):115-125.
- Mukherjee K, Perrin SM, Hughes PM. Morel-Lavallee lesion in an adolescent with ultrasound and MRI correlation. Skeletal Radiol. 2007;36 Suppl 1:S43-45.
- Neal C, Jacobson JA, Brandon C, Kalume-Brigido M, Morag Y, Girish G. Sonography of Morel-Lavallee lesions. J Ultrasound Med. 2008;27(7):1077-1081.
- Kim S. Endoscopic treatment of Morel-Lavallee lesion. Injury. 2016;47(5):1064-1066.
- Walls A, McMahon SE, MacDonald J, Bunn J. Endoscopic surgical management of a large Morel-Lavallee lesion. BMJ Case Rep. 2017;2017.
- Tseng S, Tornetta P, 3rd. Percutaneous management of Morel-Lavallee lesions. The Journal of bone and joint surgery. American volume. 2006;88(1):92-96.
- Nickerson TP, Zielinski MD, Jenkins DH, Schiller HJ. The Mayo Clinic experience with Morel-Lavallee lesions: establishment of a practice management guideline. J Trauma Acute Care Surg. 2014;76(2):493-497.
- Hak DJ, Olson SA, Matta JM. Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: the Morel-Lavallee lesion. J Trauma. 1997;42(6):1046-1051.
- Ausen K, Fossmark R, Spigset O, Pleym H. Safety and Efficacy of Local Tranexamic Acid for the Prevention of Surgical Bleeding in Soft-Tissue Surgery: A Review of the Literature and Recommendations for Plastic Surgery. Plast Reconstr Surg. 2022;149(3):774-787.
- Calpin GG, McAnena PF, Davey MG, et al. The role of tranexamic acid in reducing post-operative bleeding and seroma formation in breast surgery: A meta-analysis. Surgeon. 2023;21(4):e183-e194.
- Koc BB, Somorjai N, E PMK, et al. Endoscopic debridement and fibrin glue injection of a chronic Morel-Lavallee lesion of the knee in a professional soccer player: A case report and literature review. Knee. 2017;24(1):144-148.
- Leng P, Zhu Y, Dong Y, et al. Mid-term prognosis of endoscopic debridement combined with percutaneous cutaneo-fascial suture for the treatment of Morel-Lavallee lesion: a minimum 3-year follow-up study. Injury. 2024;55(7):111552.
- Liu M, Liu L, Zhou X, et al. A Novel Surgical Technique for treatment of Morel-Lavallee Lesion: Endoscopic debridement combined with percutaneous cutaneo-fascial suture. Injury. 2018;49(8):1630-1633.
- Kage T, Hirota J, Yamamoto N, et al. Arthroscopic treatment for Morel-Lavallee lesion of the thigh: A case report and literature review. Int J Surg Case Rep. 2021;78:58-61.
