
Manav Bains OMS IV; Zachary Husband OMS III; Aaron Lange OMS III; Benjamin Brooks PhD, MBA
Rocky Vista University College of Osteopathic Medicine
DOI: http://doi.org/10.70709/fn76ep3
Abstract
Background
The ideal surgical approach for Total Hip Arthroplasty (THA) remains debated in orthopedic joint surgery. The Direct Anterior Approach (DAA) has gained popularity due to its potential to reduce operative complications, particularly dislocation, compared to the traditional Posterior Approach (PA). However, there is still no consensus on the superiority of DAA over PA, especially when considering regional tendencies, patient-reported outcome measures (PROMs), and individual patient perceptions.
Purpose/Hypothesis
This study aims to evaluate the current literature that directly compares the DAA to the PA in THA, with a focus on PROMs. It will also highlight the limitations and complications associated with each approach. The hypothesis is that DAA and PA are comparable regarding overall patient complications, success rates, and PROMs.
Study Design
Systematic Review
Methods
The study protocol was registered with PROSPERO (ID: CRD42024538589) and conducted following PRISMA guidelines. A comprehensive search of MEDLINE and PubMed databases was performed to locate studies comparing DAA and PA in THA, with eligibility criteria including randomized controlled trials, non-randomized clinical trials, prospective and retrospective cohort studies, and case-control studies. Data were extracted systematically, capturing study demographics, PROMs, and statistically significant outcomes.
Results
A total of 38 studies were included in this systematic review. Key findings include: Nine studies reported a significantly higher rate of dislocation in the PA compared to the DAA, while seven studies found no significant difference. Ten studies analyzed infection rates with mixed results—one reported higher infection rates in the PA, while five found no significant difference. Fifteen studies discussed hip revisions, with six showing higher revision rates for the PA and five showing higher rates for the DAA. Sixteen studies specifically discussed PROMs related to satisfaction and pain; eight found no significant difference between DAA and PA, while seven reported that DAA was superior. Eleven studies discussed satisfaction and pain, with six reporting higher satisfaction scores for the DAA and four finding no significant difference. Three studies reported shorter hospital stays for the DAA.
Conclusion
The review indicates that while the DAA may offer advantages such as reduced dislocation rates and shorter hospital stays, both approaches present comparable overall complication rates, long-term outcomes, and PROMs. Surgeon preference, influenced by residency teaching and tradition, and patient-specific factors, including PROMs, remain critical in selecting the appropriate surgical approach for THA. Future research should focus on prospective, multicenter RCTs, more extended follow-up periods, and the economic implications of each approach. The debate over the ideal approach in THA continues, with current evidence suggesting that DAA and PA are viable options depending on individual patient and surgeon factors.
Keywords: Total Hip Arthroplasty, Direct Anterior Approach, Posterior Approach, Surgical Complications
Introduction
In orthopedic joint surgery, the ideal surgical approach for Total Hip Arthroplasty (THA) has long been debated. The emerging Direct Anterior Approach (DAA) has gained momentum over the past decade due to its ability to navigate the musculature efficiently and limit many operative complications associated with the Posterior Approach (PA), most notably dislocation. However, the rising popularity of the DAA within the orthopedic surgery community does not necessarily correlate with unanimous statistical and clinical evidence. Instead, the data on these trends are still in their early stages of development. In order to provide valuable information for surgeons considering a shift toward the DAA, it is essential to focus on patient-reported outcome measures (PROMs) and individual patient perceptions of the approach. These factors could significantly influence market trends and clinical decisions if they are equal or superior to the PA.
This study aims to evaluate the current body of work that directly and objectively compares the Direct Anterior approach to the Posterior Approach. In doing so, the limitations of each procedure will be highlighted and compared. The complications associated with each approach will be evaluated systematically. Many of the proponents of the Direct Anterior Approach tout the fact that the approach specifically limits the complication of posterior dislocation. Posterior dislocation is one of the most commonly associated complications with the posterior approach. However, it remains undetermined whether this complication has been statistically exploited or whether we are simply relying on tradition. This study will extrapolate whether or not these beliefs are statistically, clinically founded, and evidence based.
The limitations of the Direct Anterior Approach, although potentially less advertised, certainly exist. These include lateral femoral cutaneous nerve injury, infection, and wound complications. In Christensen et al., researchers demonstrated a significantly greater number of wound complications that required reoperation in the DAA group when compared to the PA group (p=0.007).1 In Charney et al., the DAA group had a higher risk of revision for aseptic loosening (p=0.002).2 In Wilson et al., four patients who required reoperation for wound complications were in the DAA group.3 In Zhang et al., statistically significant data was found between the DAA group and the PA group that showed the rate of nerve injury was higher in the DAA group compared to the PA group (p=0.037).4 In Hoskins et al., researchers found statistically significant data that the DAA group had a significantly higher revision rate for femoral component loosening (p<0.001).5
Understanding that the Direct Anterior Approach is potentially equivalent in its potential complications is essential to this ongoing debate. Many studies have determined that the approaches are, in fact, equivalent in their success. Watts et al., Maratt et al., Shemesh et al., Barrett et al., Pharr et al., Culliton et al., Moerenhout et al., and Bon et al. determined that there was no statistical difference in the various complications associated with each study.6-13 The body of work claiming that both approaches are equivalent is vast, and this begs whether the debate may ever truly be solved. As the debate continues, surgeon preference will continue dominating the operating room’s operative strategy.
An overwhelming amount of evidence promoting the Direct Anterior Approach is specifically founded on the complication of posterior dislocation in the Posterior Approach. In Charney et al., researchers discussed that the DAA group had a lower risk of dislocation compared to the PA group (p<0.001).2 In Bendich et al., researchers concluded that those in the DAA group had fewer dislocations requiring reoperation than those in the PA group (p=0.02) within one year of surgery.14 In Dion et al., there was a significantly lower mean number of dislocations per patient in the DAA compared to the PA (p=0.02).15 In Cichos et al., researchers found statistically significant data on 90-day dislocation, mechanical revision, and mortality between their DAA and PA groups. Further, it was found that the DAA was associated with a decreased risk of 90-day and one year dislocation (p=0.01 and p=0.01, respectively).16 In Metzger et al., a significantly higher rate of postoperative hip dislocations were discovered in the PA group than in the DAA group (p < 0.005).17
Methodology
The study protocol was registered with PROSPERO registration ID: CRD42024538589 and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.18 The associated PRISMA checklist is displayed in Figure 1.

Fig 1. PRISMA Checklist
Search Strategy
A comprehensive search was conducted using MEDLINE and PubMed databases to locate pertinent studies, with the search updated last on March 31, 2024. The Boolean search string employed included ((hip arthroplasty) OR (hip replacement)) AND (anterior approach) AND (posterior approach) AND (complication*).
Eligibility Criteria
This study followed the PICOS framework (population, intervention, comparison, outcomes, and study design) to establish inclusion criteria. Inclusion was restricted to studies that directly compared outcomes between the DAA and PA in Total Hip Arthroplasty, with a particular emphasis on PROMs and individual patient perceptions regarding each approach. Eligible research types included randomized controlled trials (RCTs), non-randomized clinical trials, prospective and retrospective cohort studies, and case-control studies. We considered articles published within the last ten years, since March 31, 2014, capturing the most current data reflective of advancements in DAA. There were no restrictions on follow-up duration. Studies designs excluded were reviews, research letters, conference abstracts, non-English articles, duplicates, irrelevant studies, cadaver studies, comparisons of the DAA with approaches other than the PA, and studies on revision surgeries.
Data Extraction
Studies were systematically managed using the Zotero online tool for efficient screening.41 Initial screening for duplicates was followed by a thorough review by two researchers (AL, ZH) based on titles and abstracts to verify adherence to inclusion criteria. Discrepancies were resolved by a third reviewer (MB). During the full-text review phase, data were extracted into a tailored electronic spreadsheet, capturing details pertaining to study demographics and statistically significant and non-significant data.
Results
Search Results
Following the removal of duplicates, we ascertained 208 titles from the selected databases as potentially relevant. Upon reviewing titles and abstracts, we excluded 151 publications. Subsequently, we examined the full texts of 57 publications, culminating in the inclusion of 38 studies in this systematic review. The selection process is depicted in a flowchart in Figure 2.
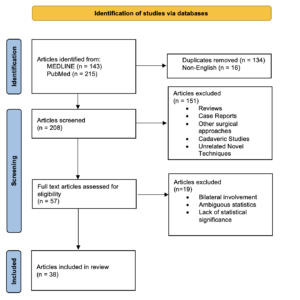
Fig 2. PRISMA Flow Chart
Study Characteristics
As seen in Table 1, the review encompasses 38 studies: 4 were randomized controlled trials (RCTs) involving 304 patients, 31 were retrospective cohort studies involving 329,702 patients, 1 was a non-randomized controlled trial involving 80 patients, 1 was a retrospective case series with 56 patients, and 1 was a prospective cohort study of 76 patients. Each study was published in English between the years 2014 and 2024. The minimum follow-up duration was two weeks, yet some papers had follow-up to 7 years post-operation. The range of sample sizes across the studies varied from 52 to 97,877.

Table 1. Study Characteristics
Hip Satisfaction
Sixteen articles specifically discussed PROMs related to satisfaction and pain, shown in Figure 3. Of these, 8 studies found no significant difference between DAA and PA, while seven studies reported that the DAA was superior with statistical significance. There were 39 individual PROM differences between DAA and PA, with 11 outcomes favoring DAA over PA. The remaining reported outcomes showed no statistical difference between the two approaches. In Loh et al., in terms of functional outcomes scores using WOMAC-pain and physical and OHS, the DAA group had better scores at 6 months and 2 years.31 Statistically significant data included pain subscale at 6 months using WOMAC that was better in the DAA group (P = 0.023) and the physical functioning subscale at 6 months and 2 years in the DAA group (P < 0.001 and P = 0.009, respectively).31 The DAA group additionally reported a better expectation score at 2 years (P = 0.043).31 In Goyal et al., the Harris hip score was better at one year in the DAA group (p = 0.001) when compared to the PA.32 The visual analog scale for hip pain was also statistically significant at 12, 25, 48, and 72 hours postoperative (p < 0.05).32 In Zhang et al., at one month post-surgery, the HHS score in the DAA group was 71.03 versus 68.39 in the PA group (p=0.014).33 In Chen et al., the HHS was statistically higher in the DAA group versus the PA group at 1, 3, and 12 months post-operation (p<0.05).34 Lastly, the visual analogue scale (VAS) was significantly lower in the DAA group when compared to the PA group at 1, 3, and 12 months post-operation (p<0.05).34 Researchers lastly showed that comprehensive satisfaction was higher in the DAA group versus the PA group (p=0.003).34 In Soza et al., there was a significantly higher postoperative HHMS at one year in DAA versus PA (p=0.015).21 In Balasubramaniam et al., researchers discovered there was a higher HHS at 12 months postoperative in the DAA group compared to the PA (p=0.02).35 Not to mention, in Graves et al., researchers concluded the DAA was associated with worse adjusted patient-reported Veterans RAND-12 Mental Component Summary score changes 1 and 3 months after surgery compared with the PA (p<0.001).36 The DAA was also associated with greater patient-reported Veterans RAND-12 Physical Component Summary score improvement at 3 months compared with the PA group (p=0.008).36
In Culliton et al., researchers didn’t find statistically significant data in femoral component migration and Harris Hip postoperative scores.11 In Barrett et al., researchers concluded there were no differences between the DAA and PA group in terms of HHS, UCLA activity score and Hip Disability and Osteoarthritis Outcome Score Jr.9 In Malek et al., researchers showed there were no differences between DAA and PA in mean OHS at 6 and 24 months (p=0.08 and 0.29, respectively).23 In Nambiar et al., researchers showed there was no difference in OHS and WOMAC scores across various time points ranging from 2 weeks postoperative to 5 years (p>0.05).36

Fig 3. Patient Reported Outcome Measures
HHS, Harris hip score, VAS, visual analog scale of pain, SF-12, short form 12, OHS, oxford hip score, WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index, EQ-5D-5L, EuroQol 5-Dimension 5-Level, FJS-12, Forgotten Joint Score-12, UCLA, UCLA Activity Score
Hip Dislocations
A total of nine articles discussed differences in hip dislocation between the DAA and PA approach. Of the articles that included statistically significant data, all showed that there was a significantly higher rate of dislocation in the PA versus the DAA approach. In Metzger et al., a significantly higher rate of postoperative hip dislocations was discovered in the PA group compared to those in the DAA group (p < 0.005). 17 Further, it was found in Cichos et al., that the DAA was associated with a decreased risk of 90-day and one year dislocation (p=0.01 and p=0.01, respectively).16 In Dion et al., there was a significantly lower mean number of dislocations per patient in the DAA when compared to the PA (p=0.02).15 In Bendich et al., researchers concluded that those in the DAA group had fewer dislocations requiring reoperation than those in the PA group (p=0.02) within one year of surgery.14 In Kurkis et al., researchers found a decreased rate in the DAA versus the PA for dislocations (p=0.002).19 In Charney et al., researchers discussed that the DAA group had a lower risk of dislocation compared to the PA group (p<0.001).2 In Haller et al., researchers concluded there were significantly more hip dislocations in the PA group compared to the DAA (p=0.037).20 In Soza et al., There was a significantly higher rate in hip dislocations in the PA group versus DAA (p=0.017).21 In Jungwirth-Weinberger et al., at the one-year follow-up there was found to be a significantly higher incidence of dislocations in the PA group compared to DAA (p=0.008).22
Next, there were seven articles that included no statistically significant differences of DAA versus the PA approach. Further, In Malek et al., researchers showed there were no differences between DAA and PA in dislocation (p=1.0).23 In Maratt et al., researchers showed there was no difference in the dislocation rate amongst those in the DAA versus the PA groups.7 In Cichos et al., researchers found that there were no significant differences between 90-day and 1-year postoperative dislocation rates between DAA and PA.16 In Tay et al., there was no statistically significant data to show a difference between the DAA and PA when it came to dislocations.24 In Bon et al., there was one dislocation in the DAA group and none in the PA group, showing no statistical significance, p = 1.00.13 In Wilson et al. there were no statistically significant differences in the rates of dislocations between DAA and PA (p=0.06).25 Lastly, in Shah et al., researchers concluded there were no significant differences in dislocations.26
Hip Infections
A total of eleven articles discussed rates of hip infections following THA. Three articles showed a higher rate of infections in the PA versus the DAA. Further, In Metzger et al., there was also a significantly higher rate of deep infections in PA versus DAA (p<0.005).17 In Haller et al., there were also significantly more postoperative infections in the PA group compared to DAA (p=0.001).20 In Ponzio et al., researchers showed there was a significantly lower percentage in minor systemic complication rates between DAA (6.2%) and PA (10.9%) groups (p=0.012).27 The minor complications were identified using ICD-9-CM codes that necessitated additional observational or required medical treatment, including hypotension, syncope, tachycardia, delirium, UTI, urinary retention, superficial incisional site infection, paralytic ileus, and pleural effusion.27
There were a total of two articles that showed higher rates of complications related to infection in the DAA group versus the PA group. In Kurkis et al., there was an increased risk of superficial wound complications in the DAA group versus the PA group (p=0.003).19 In Christensen et al., researchers demonstrated that there was a significantly greater number of wound complications that required reoperation in the DAA group when compared to the PA group (p=0.007).1
Indeed, there were five articles showed no difference in PA versus DAA in relation to infections. In Malek et al., researchers showed there were no differences between DAA and PA incidence of infection (p=1.0).23 In Purcell et al., researchers concluded there were no differences in deep infection rates between the DAA and PA across nonobese and obese patients.28 In Watts et al., researchers showed there was no significant difference between the DAA and PA in terms of wound complications.6 In Wilson et al., there were no statistically significant differences in the rates of deep infections and wound complications between DAA and PA (p=1.00 and p=0.09, respectively).25 Lastly, in Tay et al., there was no statistically significant data to show a difference between the DAA and PA when it came to infections.24
Finally, in Wernecke et al., researchers studied prosthetic joint infection (PJI). Researchers concluded that there was a significantly reduced 90-day PJI revision rate for the DAA group than the PA group (0.2 versus 0.6%, OR = 0.36, p<0.01).29 Researchers discussed that the finding may be explained by differences in the type of surgery performed for PJI between the 2 approaches.29
Hip Revisions
A total of fifteen articles discussed hip revisions. A total of six articles discussed various reasons for PA having a higher revision rate as compared to DAA for reasons discussed next. In Metzger et al., there was a higher revision rate observed in the PA group versus the DAA group (p<0.005).17 In Haller et al., there were also significantly more revision THA procedures in the PA group compared to DAA (p=0.037).20 Also, in Dion et al., there as a significant lower difference in those that required revision surgery in the DAA group contrasted to those in the PA group (p=0.005).15 In Ponzio et al., there was a significantly greater revision rate for the PA group (2.7%) when compared to the DA group (0.7%) (p=0.032).27 The predominant reason for revision was for dislocation.27 In Hoskins et al., the PA was associated with a higher rate of revision for infection compared to DAA (p<0.001).5 And lastly, there was a higher rate of revision in PA for dislocation compared to DAA (p<0.001).5 In Charney et al., the DAA group also had a lower all-cause revision risk (p<0.029).2 There was also a lower risk of revision for instability (p<0.001) and a lower risk of revision for periprosthetic fracture (p=0.033) in the DAA group.2 There was a lower rate of revision in Hoskins et al., for infection in the AA group as well as dislocation/instability between 0 to 3 months (p=0.001 and p=0.008, respectively).5 Finally, there was a decreased risk in Cichos et al. of mechanical revision THA in the DAA group compared to the PA group at the 90-day and one-year timeline (both p=0.01).16
Next, five articles discussed various reasons why the DAA was associated with higher revision rates as compared to the PA. Further, in Meneghini et al., researchers showed that revisions due to femoral failure were more common in patients undergoing DAA than PA (50.9% versus 14.3%, respectively with p=0.001.30 In Hoskins et al., there was found to be a higher rate of major revisions in the DAA when compared to PA (p=0.001).5 These included revisions involving a change of the acetabular and/or femoral component and revision for specific diagnoses as discussed next.5 There was a higher rate of revision for femoral loosening with the anterior approach when compared to posterior (p<0.001).5 There was a higher rate of revision for fracture in the first three months in the DAA when compared to PA (p<0.001).5 In Hoskins et al., there was found to be a higher cumulative percent revision in the DAA group for femoral loosening and periprosthetic fracture compared to the PA group (p<0.001).5 However, the DAA group in Charney et al. had a higher risk of revision for aseptic loosening (p=0.002).2 The revisions involved the acetabulum (4/32), femur (22/32), and 6/32 involved both components of the anterior group.2 In Hoskins et al., researchers found statistically significant data in that the AA group in their study had a significantly higher rate of revision for femoral component loosening (p<0.001).5
Lastly, five articles showed no statistically significant differences in the DAA versus the PA for postoperative revision rates. In Malek et al., researchers showed there were no differences between DAA and PA in reoperation (p=0.21).23 In Tay et al., there was no statistically significant data to show a difference between the DAA and PA when it came to revision.24 There was also no differences between 90-days and 1-year postoperative outcomes between the DAA and PA when it came to revision surgery in Cichos et al.16 Shah et al. also discussed no differences at 90 days and one year postoperatively for reoperations.26 In Wilson et al., there were no statistically significant differences in revision rates between DAA and PA in regards to periprosthetic fractures, dislocations, or infections (p=0.32, 0.32, and 1, respectively).25
Length of Stay
There were a total of four articles that discussed length of stay as one of their parameters. Three of the four articles showed that the length of stay significantly lower in the DAA group versus the PA group. Further, in Soza et al., researchers concluded there was a significantly lower length of stay for the DAA compared to PA (4.54 versus 5.53 with p<0.001).21 In Chen et al., researchers concluded that the length of stay was statistically lower in the DAA group when compared to the PA group (p<0.05).34 In Loh et al., researchers were able to conclude that those in the DAA group had a length of stay of 2.9 days versus 5.4 in the PA group, which was statistically significant (P < 0.001).31 However, one paper showed there was no such difference. In Moerenhout et al., there were no statistically significant findings comparing DAA and PA to length of hospital stay and postoperative recovery.12
Other Parameters
There were several articles that discussed other parameters not discussed previously. Statistically significant data is highlighted below. In Chow et al., researchers were able to find statistically significant data in that those in their DAA group who had navigation software utilized during surgery versus those in the PA group without navigation had a significant difference in both anteversion and inclination (p<0.05 and p<0.05, respectively).38 In Rathod et al., researchers concluded that there were variances for cup inclination in the DAA group that were significantly lower when compared to the PA group (p<0.01).39 They also found that target inclination and anteversion were achieved better in the DAA group as compared to the PA group (p<0.01).39 In Zhang et al., statistically significant data was found between the DAA group and the PA group that showed the rate of nerve injury was higher in the DAA group compared to the PA group (p=0.037).33 They discussed that the main nerve injury was to the lateral femoral cutaneous nerve.33 In Purcell et al., researchers showed there was a higher rate of superficial wound dehiscence in the DAA group compared with the PA group across all BMIs (p=0.01).28 At one year follow-up, researchers in Cichos et al. showed there was found to be a significantly lower mortality rate in the DAA group compared to the PA group (p=0.018).16 However, researchers in Shah et al. concluded there were no significant differences in mortality at 90 days and one year postoperatively.26 Next, in Baba et al., there was found to be a significant improval in the symptoms of urinary incontinence in the DAA group and aggravated in the PA group (p=0.0057).39 In Malek et al., the rate of periprosthetic femoral fractures was significantly higher in the DAA group compared to the PA group (p=0.04).23 However, researchers in Cichos et al. found that there were no significant differences between 90-day and 1-year postoperative outcomes between DAA and PA when discussing periprosthetic fracture.16 There were also no significant differences in Wilson et al. between the DAA and the PA in regards to the all-cause rate of periprosthetic fractures (p=0.19).3 In Nambiar et al., there was no difference in implant survival between DAA and PA, with all-cause revision as an endpoint (p>0.05).37 There was also found in Cichos et al. to be a decreased risk of 90-day and one-year mortality in the DAA group when compared to the PA group (p=0.03 and p=0.02, respectively).16 Lastly, in Shemesh et al., researchers concluded that there was not a statistically significant difference in the incidence of trochanteric bursitis between the PA and DAA (p=0.47).40
Discussion
The Direct Anterior Approach (DAA) versus Posterior Approach (PA) in Total Hip Arthroplasty (THA) continues to be a well-debated topic among orthopedic surgeons. Both approaches are widely practiced in the US, and evaluating which approach is more proficient is a complicated endeavor given the numerous factors that need to be considered. This review aims to contribute to the discussion by assessing the current literature that directly compares complication rates between each approach.
This review also examined various studies assessing hip satisfaction and functional outcomes in Total Hip Arthroplasty, comparing the Direct Anterior Approach (DAA) and the Posterior Approach (PA). Sixteen focused on these parameters, with the majority indicating better outcomes for the DAA group. Specifically, studies reported higher scores in the DAA group across various metrics, such as pain levels, physical functioning, and overall hip satisfaction at different postoperative intervals. For example, Loh et al. found that the DAA group had better WOMAC pain and physical functioning scores at six months and two years post-surgery.31 Similarly, Goyal et al. and Chen et al. reported higher Harris hip scores and lower pain scores in the DAA group at various time points post-operation.32,34
HHS was the most reported PROM with 5 of 12 study outcomes favoring DAA over PA with less functional deficits post- operation. There was no statistically significant difference reported in the 7 remaining study outcomes. Despite these positive findings, few studies mentioned PROMs without significant differences between the DAA and PA regarding postoperative functional outcomes and hip satisfaction. Studies like Culliton et al., Barrett et al., and Malek et al. showed no notable variance in outcomes such as femoral component migration, Harris Hip Scores, and the Oxford Hip Score between the two approaches.9,16,23
Hip dislocation was evidenced as one of the most prominent complications in the vast body of work that exists on the topic. Historically, posterior dislocations have a high association with the PA approach. The studies that were included in this review also follow this concept. Fifteen studies assessed hip dislocation rates between the direct anterior and posterior approaches. Ten studies reported a statistically significant increase in dislocation rates associated with the PA, and five found no statistically significant difference between approaches. The studies that reported significant differences were large cohort studies, suggesting more robust results. For instance, Metzger et al. reviewed 2,452 surgeries performed by a single surgeon who transitioned to the DAA after 455 PA surgeries. They found statistically significant differences in the overall complication rate between approaches (0.25% vs 1.57%) and the first 1,000 DAA surgeries versus all PA surgeries (p=0.017).17
Similarly, Bendich et al. matched 2,348 DAA cases to 2,348 PA cases from 2016 to 2019 based on patient characteristics, including age, gender, and BMI, across 29 surgeons. They reported an increased PA association with dislocation at one year compared to the DAA.14 Charney et al. assessed 38,399 THA, with 6,428 DAA, completed by 193 surgeons across 43 hospitals from 2009 to 2017 and determined a lower risk of dislocation associated with the DAA (HR=0.39, 95% CI=0.34-0.96) after adjusting for covariates.2 Bendich et al. and Charney et al. reported the most substantial evidence of included studies that the DAA is associated with a lower risk of hip dislocation than the PA. The studies that found no difference in hip dislocation rates between the DAA and the PA consisted of smaller sample sizes and were typically completed by single surgeons or at one center, suggesting lower external validity.
Numerous studies in this review also included analysis of superficial and deep postoperative infection rates. Ten studies included in this review analyzed infection occurrence rate, with four finding no difference between the DAA and the PA and six finding a difference in comparisons. Metzger et al. retrospectively assessed surgeons transitioning from the PA to the DAA, with significantly more DAA cases included than PA cases.17 Surgeon experience may have played a role in the approaches chosen for the retrospective cases explored by the study. Previous literature has reported increased infection rates associated with the DAA. This finding was not supported by the body of work explored in this study and may reflect improved protocols or decreased operation time as the DAA has become more widely used by orthopedic surgeons
Several studies assessed the rates of secondary revisions in DAA versus PA cases in Total Hip Arthroplasty, highlighting the trends found in complication rates for each respective approach. Research findings showed higher revision rates due to deep infections and dislocations in the PA group, indicating specific vulnerabilities associated with this technique. Conversely, the DAA group exhibited lower revision rates for instability and periprosthetic fractures, suggesting some inherent advantages regarding long-term complications. Despite these trends, other studies pointed out increased revision rates in the DAA group for complications such as femoral loosening and fractures. However, multiple studies concluded that there were no significant differences in revision rates between the two approaches.
The review also explored the length of hospital stay as a parameter in four articles. Three of these four studies found that patients in the DAA group experienced shorter hospital stays than those in the PA group. Specifically, research by Soza et al. and Chen et al. supported this conclusion, indicating that the DAA was associated with a reduced length of stay. Loh et al. further supported these findings, noting a notably shorter stay for the DAA group.31 In contrast, the study conducted by Moerenhout et al. did not find any statistically significant differences in hospital stay duration between the DAA and PA groups, suggesting variability in outcomes dependent on specific study conditions or methodologies.12 This review highlights the potential for expedited recovery time associated with the DAA, though results may vary across different research settings.
The review further analyzed several additional parameters addressed in several studies, with significant findings reported in various aspects of surgical outcomes. The Direct Anterior Approach (DAA), particularly when augmented with navigation technology, demonstrated enhanced surgical precision and more accurate component placement. However, it was also associated with higher risks of nerve injuries and superficial wound dehiscence, which may complicate wound healing and nerve integrity. Despite these risks, the DAA showed potential benefits, including lower mortality rates at one-year follow-ups and improved urinary incontinence, suggesting better long-term patient outcomes and recovery. On the other hand, it was linked to a higher incidence of periprosthetic femoral fractures. The incidence of trochanteric bursitis showed no significant differences between the approaches, highlighting that the choice of surgical technique may not influence specific complications.
The inherent limitations of this study must be acknowledged to understand the context and scope of its findings fully. Firstly, most of the included studies relied on retrospective data, which, although extensive, could be susceptible to selection and reporting bias. This potential influence might affect the comparability and generalizability of the results across different populations and surgical settings. Additionally, variability in follow-up duration among studies could affect the consistency of the outcomes measured, particularly regarding long-term complications and revisions. Another limitation was the lack of standardized criteria for surgical proficiency and experience across studies, which might significantly impact the outcomes of the Direct Anterior Approach (DAA) versus the Posterior Approach (PA). Such differences could obscure whether discrepancies in outcomes were due to the surgical approach or the surgeon’s skill level.
Additional limitations to the study include the numerous studies that include other approaches besides PA and DAA. There were numerous articles that compared DAA and PA as well as Posterior Lateral, and Superior approaches. These studies were not included because of the additional confounding data and variables that adding additional approaches would have created. The purpose of this study was to determine which approach was more efficient between PA and DAA only, and so all of the other current approaches that are being used were not included. Although this serves the conclusions of the study well, it is not to say that these other approaches are not viable and will not be included in future research and discussions on the topic.
The clinical relevance of comparing the DAA to the PA in Total Hip Arthroplasty (THA) lies in the potential to optimize surgical outcomes and minimize complications. The study underscores the DAA’s potential advantages, such as a reduced risk of hip dislocation and possibly shorter hospital stays. These benefits are pivotal in improving patient recovery times and reducing healthcare costs. However, the findings also suggest that both approaches are comparable in terms of overall complication rates and long-term revisions. This equivalence underscores the importance of a nuanced understanding of patient selection, where specific patient anatomy and comorbidities might favor one approach over the other. Thus, the decision on the surgical approach should be tailored to individual patient profiles, taking into account the surgeon’s familiarity and expertise with the respective techniques.
Future research in THA should strive to build upon the foundation laid by current studies. This can be achieved by incorporating more prospective, multicenter randomized controlled trials (RCTs) that can provide higher quality evidence with minimized bias. These studies should aim for longer follow-up periods to capture more comprehensive data on long-term outcomes and revisions. It would also be beneficial to include more granular data on surgeon experience and standardized surgical techniques to better assess the impact of these factors on patient outcomes. Additionally, future research should delve into the economic implications of each surgical approach, considering both direct medical costs and indirect costs such as time off work and rehabilitation needs. Given the advancements in surgical technology, such as robotic-assisted THA, integrating these technological enhancements into comparative studies could provide valuable insights into further optimizing surgical outcomes between the DAA and PA.
Ideally, future research will also provide more specific insights into determining the number of orthopedic surgeons currently utilizing each approach. Although this topic was limited in the current body of work, discovering the current number of orthopedic surgeons utilizing each technique is imperative to the discussion and would be extremely revealing as to which approach has been determined to be more effective by the surgery community.
Conclusion
THA is one of modern orthopedic medicine’s most prevalent and successful surgeries. The two main approaches, DAA and PA, each have their benefits and risks, and a comprehensive assessment of each approach may be essential to determine which is more advantageous for specific patients. Considerations may include patient characteristics, surgeon preference, and possible complications. After analyzing patient-reported outcomes and the complications associated with each approach, the current body of work supports that stigmas associated with each approach are evidenced. The body of evidence regarding regional tendencies for the use of DAA over PA is emerging, and future work on this topic will ideally bear statistical evidence and preferences for the use of DAA vs. PA regionally. Historical complications associated with the PA, such as posterior dislocation, persist. However, this review indicates that these complication rates may be less profound than expected. Many well-cited articles support that there may be insignificant differences between complications associated with each procedure, suggesting that there may not be an “ideal approach” to THA and that surgeon preference, influenced by residency teaching and tradition, will remain the most critical determining factor for the method of approach chosen. While the DAA has been increasingly supported as the “best method” by the orthopedic community, it continues to be associated with numerous complications, most notably infection and cutaneous nerve pathology.
This review adds to the existing discussion on THA by summarizing current literature that directly compares the DAA and PA complication rates. Doing so may help current orthopedic surgeons with clinical decision-making, persuade surgeons to switch from the PA to the DAA, or indicate important educational points as surgeons train in performing THA, thus providing patients with improved health outcomes. The comparison between the Direct Anterior Approach and the Posterior approach is an age-old discussion, and as more retrospective case data is uncovered, the complications of the DAA will become more evident, and greater comparisons can be made between the two approaches. The current literature argues that there is no clear distinction as to whether DAA is definitively a more ideal approach to THA than the Posterior Approach and that more DAA surgeries will have to be performed in order to draw definitive conclusions between the success of the Direct Anterior Approach vs. the Posterior Approach.
References
- Christensen CP, Karthikeyan T, Jacobs CA. Greater prevalence of wound complications requiring reoperation with direct anterior approach total hip arthroplasty. J Arthroplasty. 2014;29(9):1839-1841. doi:10.1016/j.arth.2014.04.036
- Charney M, Paxton EW, Stradiotto R, et al. A Comparison of Risk of Dislocation and Cause-Specific Revision Between Direct Anterior and Posterior Approach Following Elective Cementless Total Hip Arthroplasty. J Arthroplasty. 2020;35(6):1651-1657. doi:10.1016/j.arth.2020.01.033
- Wilson TJ, Kleiber GM, Nunley RM, Mackinnon SE, Spinner RJ. Distal peroneal nerve decompression after sciatic nerve injury secondary to total hip arthroplasty. J Neurosurg. 2018;130(1):179-183. doi:10.3171/2017.8.JNS171260
- Zhang D, Pan L, Maimaitijuma T, Liu H, Wu H. Imaging Analysis of Prosthesis Angle after Hip Replacement with Direct Anterior Approach in Lateral Position [retracted in: J Healthc Eng. 2023 Oct 11;2023:9829547. doi: 10.1155/2023/9829547]. J Healthc Eng. 2021;2021:5540834. Published 2021 Feb 17. doi:10.1155/2021/5540834
- Hoskins W, Bingham R, Lorimer M, Hatton A, de Steiger RN. Early Rate of Revision of Total Hip Arthroplasty Related to Surgical Approach: An Analysis of 122,345 Primary Total Hip Arthroplasties. J Bone Joint Surg Am. 2020;102(21):1874-1882. doi:10.2106/JBJS.19.01289
- Watts CD, Houdek MT, Wyles CC, Sierra RJ, Trousdale RT, Taunton MJ. Direct Anterior Versus Posterior Simultaneous Bilateral Total Hip Arthroplasties: No Major Differences at 90 Days. Am J Orthop (Belle Mead NJ). 2016;45(6):E373-E378.
- Maratt JD, Gagnier JJ, Butler PD, Hallstrom BR, Urquhart AG, Roberts KC. No Difference in Dislocation Seen in Anterior Vs Posterior Approach Total Hip Arthroplasty. J Arthroplasty. 2016;31(9 Suppl):127-130. doi:10.1016/j.arth.2016.02.071
- Shemesh SS, Moucha CS, Keswani A, Maher NA, Chen D, Bronson MJ. Trochanteric Bursitis Following Primary Total Hip Arthroplasty: Incidence, Predictors, and Treatment. J Arthroplasty. 2018;33(4):1205-1209. doi:10.1016/j.arth.2017.11.016
- Barrett WP, Turner SE, Murphy JA, Flener JL, Alton TB. Prospective, Randomized Study of Direct Anterior Approach vs Posterolateral Approach Total Hip Arthroplasty: A Concise 5-Year Follow-Up Evaluation. J Arthroplasty. 2019;34(6):1139-1142. doi:10.1016/j.arth.2019.01.060
- Pharr ZK, Rider CM, Bell JW, Wilde JH, Westbrooks TJ, Toy PC. Outpatient Hip Safety in an Ambulatory Surgery Center Is Independent of Approach [published correction appears in J Arthroplasty. 2021 Sep;36(9):3351. doi: 10.1016/j.arth.2021.06.011]. J Arthroplasty. 2021;36(1):231-235. doi:10.1016/j.arth.2020.07.068
- Culliton K, Louati H, Sandoval E, et al. Early femoral component migration: comparing the anterior and posterior approach to the hip. Hip Int. 2020;30(2):160-166. doi:10.1177/1120700019848103
- Moerenhout K, Derome P, Laflamme GY, Leduc S, Gaspard HS, Benoit B. Direct anterior versus posterior approach for total hip arthroplasty: a multicentre, prospective, randomized clinical trial. Can J Surg. 2020;63(5):E412-E417. doi:10.1503/cjs.012019
- Bon G, Kacem EB, Lepretre PM, et al. Does the direct anterior approach allow earlier recovery of walking following total hip arthroplasty? A randomized prospective trial using accelerometry. Orthop Traumatol Surg Res. 2019;105(3):445-452. doi:10.1016/j.otsr.2019.02.008
- Bendich I, Landy DC, Do H, et al. Intraoperative Complications and Early Return to the Operating Room in Total Hip Arthroplasty Performed Through the Direct Anterior and Posterior Approaches. An Institutional Experience of Surgeons After Their Learning Curve. J Arthroplasty. 2021;36(8):2829-2835. doi:10.1016/j.arth.2021.03.046
- Dion CA, Schmidt-Braekling T, Falsetto A, Kreviazuk C, Beaulé PE, Grammatopoulos G. Does Surgical Approach Influence the Natural History of the Unstable Total Hip Arthroplasty?. J Arthroplasty. 2022;37(4):787-794. doi:10.1016/j.arth.2021.12.012
- Cichos KH, Mabry SE, Spitler CA, McGwin G Jr, Quade JH, Ghanem ES. Comparison Between the Direct Anterior and Posterior Approaches for Total Hip Arthroplasty Performed for Femoral Neck Fracture. J Orthop Trauma. 2021;35(1):41-48. doi:10.1097/BOT.0000000000001883
- Metzger CM, Farooq H, Hur JO, Hur J. Transitioning from the Posterior Approach to the Direct Anterior Approach for Total Hip Arthroplasty. Hip Pelvis. 2022;34(4):203-210. doi:10.5371/hp.2022.34.4.203
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Published 2021 Mar 29. doi:10.1136/bmj.n71
- Kurkis GM, Chihab S, Farley KX, Anastasio AT, Bradbury TL, Guild GN. Anterior Revision Hip Arthroplasty is Associated With Higher Wound Complications but Fewer Dislocations Compared to Posterior Revision Hip Surgery. J Arthroplasty. 2021;36(1):250-254. doi:10.1016/j.arth.2020.07.030
- Haller JM, Working ZM, Ross HL, Gililland JM, Kubiak EN. Fewer Hip Dislocations With Anterior Total Hip Arthroplasty for Displaced Femoral Neck Fracture. Orthopedics. 2021;44(2):e248-e252. doi:10.3928/01477447-20210104-02
- Soza D, Pujol O, Lara Y, Castellanos S, Hernández A, Barro V. A comparative of a single novice surgeon’s direct anterior approach and posterior approach learning curves in total hip arthroplasty: a retrospective cohort study. Eur J Orthop Surg Traumatol. 2022;32(4):767-774. doi:10.1007/s00590-021-03039-4
- Jungwirth-Weinberger A, Schmidt-Braekling T, Rueckl K, Springer B, Boettner F. Anterior hip replacement: lower dislocation rates despite less restrictions?. Arch Orthop Trauma Surg. 2022;142(10):2413-2417. doi:10.1007/s00402-021-03849-5
- Malek IA, Royce G, Bhatti SU, et al. A comparison between the direct anterior and posterior approaches for total hip arthroplasty: the role of an ‘Enhanced Recovery’ pathway. Bone Joint J. 2016;98-B(6):754-760. doi:10.1302/0301-620X.98B6.36608
- Tay K, Tang A, Fary C, Patten S, Steele R, de Steiger R. The effect of surgical approach on early complications of total hip arthroplasty. Arthroplasty. 2019;1(1):5. Published 2019 Sep 3. doi:10.1186/s42836-019-0008-2
- Wilson TJ, Kleiber GM, Nunley RM, Mackinnon SE, Spinner RJ. Distal peroneal nerve decompression after sciatic nerve injury secondary to total hip arthroplasty. J Neurosurg. 2018;130(1):179-183. doi:10.3171/2017.8.JNS171260
- Shah ID, Piple AS, Schlauch AM, et al. Direct Anterior Versus Posterior Approach for Total Hip Arthroplasty Performed for Displaced Femoral Neck Fractures. J Orthop Trauma. 2023;37(11):539-546. doi:10.1097/BOT.0000000000002650
- Ponzio DY, Poultsides LA, Salvatore A, Lee YY, Memtsoudis SG, Alexiades MM. In-Hospital Morbidity and Postoperative Revisions After Direct Anterior vs Posterior Total Hip Arthroplasty. J Arthroplasty. 2018;33(5):1421-1425.e1. doi:10.1016/j.arth.2017.11.053
- Purcell RL, Parks NL, Cody JP, Hamilton WG. Comparison of Wound Complications and Deep Infections With Direct Anterior and Posterior Approaches in Obese Hip Arthroplasty Patients. J Arthroplasty. 2018;33(1):220-223. doi:10.1016/j.arth.2017.07.047
- Wernecke GC, Jin XZ, Lin JL, Harris IA. The Impact of Surgical Approach on 90-Day Prosthetic Joint Infection After Total Hip Replacement – A Population-Based, Propensity Score-Matched Cohort Study. J Arthroplasty. 2024;39(1):151-156. doi:10.1016/j.arth.2023.06.033
- Meneghini RM, Elston AS, Chen AF, Kheir MM, Fehring TK, Springer BD. Direct Anterior Approach: Risk Factor for Early Femoral Failure of Cementless Total Hip Arthroplasty: A Multicenter Study. J Bone Joint Surg Am. 2017;99(2):99-105. doi:10.2106/JBJS.16.00060
- Loh B, Padki A, Yew A, Pang HN. Functional outcome of direct anterior versus posterior approach in total hip arthroplasty: a propensity-matched Asian study. Singapore Med J. Published online February 16, 2024. doi:10.4103/singaporemedj.SMJ-2021-125
- Goyal T, Choudhury AK, Paul S, Das L, Gupta T. The direct anterior approach without traction table: How does it compare with the posterior approach? – A prospective non-randomised trial. J Clin Orthop Trauma. 2022;31:101924. Published 2022 Jun 21. doi:10.1016/j.jcot.2022.101924
- Zhang B, Liu S, Liu Z, et al. Clinical and radiologic outcomes in patients undergoing primary total hip arthroplasty with Collum Femoris Preserving stems: a comparison between the direct anterior approach and the posterior approach. BMC Musculoskelet Disord. 2022;23(1):77. Published 2022 Jan 22. doi:10.1186/s12891-022-05040-2
- Chen MJ, Wadhwa H, Bellino MJ. Sequential ilioinguinal or anterior intrapelvic approach with anterior approach to the hip during combined internal fixation and total hip arthroplasty for acetabular fractures. Eur J Orthop Surg Traumatol. 2021;31(4):635-641. doi:10.1007/s00590-020-02810-3
- Balasubramaniam U, Dowsey M, Ma F, Dunin A, Choong P. Functional and clinical outcomes following anterior hip replacement: a 5-year comparative study versus posterior approach. ANZ J Surg. 2016;86(7-8):589-593. doi:10.1111/ans.13598
- Graves SC, Dropkin BM, Keeney BJ, Lurie JD, Tomek IM. Does Surgical Approach Affect Patient-reported Function After Primary THA?. Clin Orthop Relat Res. 2016;474(4):971-981. doi:10.1007/s11999-015-4639-5
- Nambiar M, Cheng TE, Onggo JR, et al. No Difference in Functional, Radiographic, and Survivorship Outcomes Between Direct Anterior or Posterior Approach THA: 5-Year Results of a Randomized Trial. Clin Orthop Relat Res. 2021;479(12):2621-2629. doi:10.1097/CORR.0000000000001855
- Chow J, Pearce S, Cho KK, Walter W. Direct Anterior Approach Using Navigation Improves Accuracy of Cup Position Compared to Conventional Posterior Approach. Cureus. 2017;9(7):e1482. Published 2017 Jul 17. doi:10.7759/cureus.1482
- Baba T, Homma Y, Takazawa N, et al. Is urinary incontinence the hidden secret complications after total hip arthroplasty?. Eur J Orthop Surg Traumatol. 2014;24(8):1455-1460. doi:10.1007/s00590-014-1413-4
- Shemesh SS, Moucha CS, Keswani A, Maher NA, Chen D, Bronson MJ. Trochanteric Bursitis Following Primary Total Hip Arthroplasty: Incidence, Predictors, and Treatment. J Arthroplasty. 2018;33(4):1205-1209. doi:10.1016/j.arth.2017.11.016
- Zotero | Your personal research assistant. www.zotero.org. https://www.zotero.org
