
Liam Ortega, DO1; Samuel Stegelmann, MD2; Elizabeth Simmons, DO1; Hunter Ostlie, MD1; Nathan Fogt, DO1
1Mercy St. Vincent Medical Center, Department of Orthopaedics and Sports Medicine, Toledo, Ohio, USA,
2Department of Orthopedic Surgery, Medical City Denton, Denton, Texas, USA
DOI: 10.70709/8o44ueavmo
ABSTRACT
Background
The term “black cloud” is commonly used among surgical residency programs to refer to someone who has a relative tendency to attract a disproportionate number of consults or surgeries while on call. This study aimed to evaluate whether “black clouds” exist in orthopedic surgery and assess other variables that may influence workload on a given call shift.
Methods
Information from 632 call shifts was retrospectively reviewed from an orthopedic trauma service at a Level I trauma center. Primary outcomes included the number of consults and add-on surgeries scheduled during each 24-hour shift among individual residents and attending physicians. Additionally, days of the week, seasons, weather patterns, holidays, and other superstitious variables were investigated.
Results
Individual residents or attending physicians were not associated with the number of consults (p = 0.478; p = 0.561) or add-on surgeries/shift (p = 0.436; p = 0.429). However, more consults/shift occurred during the summer (p = 0.001), on weekends (p = <0.001), on sunny days (p = 0.004), and days without rain (p = 0.013) or snow (p = 0.016). Average daily temperature was also positively correlated with both consults/shift (rs = 0.175; p = <0.001) and add-on surgeries/shift (rs = 0.118; p = 0.003).
Conclusion
The overall volume of consults and add-on surgeries was associated with several weather and calendar-related variables, but not the individual resident or attending surgeon on call in our data set. Thus, it appears more appropriate to consider a “black cloud” in the literal sense rather than a figurative one.
Keywords: black cloud, orthopedic surgery, trauma, call, consults
INTRODUCTION
The term “black cloud” is commonly used with disdain among surgical residency programs, referring to someone who has a relative proclivity to attract consults or surgeries.1 This metaphorical name is derived from weather patterns, where dark, overcast skies are typically a harbinger for an imminent storm. Medical professionals are no strangers to superstitions, especially when they relate to trauma cases presenting to the emergency department (ED). As many as 65% of residents in the ED believe that certain individuals are truly “black clouds”.2 This widespread belief is shrouded in superstition and continues to persist despite many studies showing no objective support for it.2-10
In contrast to figurative “black clouds,” weather patterns are generally acknowledged to be associated with overall trauma volume, including emergency department admissions, fractures, and road traffic accidents.11-13 Furthermore, there are various intangible factors that garner superstition, including phases of the moon, with as many as 80% of emergency medicine professionals believing that full moons are associated with higher numbers of trauma admissions.10
Previous studies have investigated “black clouds” in family medicine,6 pediatrics,3,9 apheresis medicine,7 otolaryngology,4 podiatry,5 and hand surgery.14 Yet to the best of our knowledge, no similar studies have been performed in orthopedic surgery. With the concept of “black cloud” harboring such a strong enigma among residents in surgical subspecialties, we owe it to our colleagues to provide support for or against this concept in a representative cohort. This study aims to evaluate whether “black clouds” truly exist within a single orthopedic surgery residency program at a Level I trauma center, while evaluating additional factors that may be associated with orthopedic trauma volume. Based on the findings of past research, we hypothesized that no individual “black cloud” would be identified.
METHODS
We performed a retrospective review of call schedules from October 2019 to December 2020 and December 2021 to June 2022 at an orthopedic surgery residency program located at a Level I trauma institution. This gap in the dates was due to paper copies of call shifts from this period being disposed of. There were 15 residents, including three per postgraduate year (PGY) class, and seven attending physicians included in this study. No patient-identifying information was collected, thus institutional board review approval was not obtained.
The outcomes of interest were consults/shift and add-on surgeries/shift. A consult was defined as any unscheduled orthopedic surgery consult received for a patient in the ED or on an inpatient floor that required in-person consultation by an on-call resident. At our hospital, orthopedic surgery residents are responsible for all orthopedic-related consults except for non-fracture foot trauma, which is covered by the podiatry service. Consults were attributed to shifts based on when they were received rather than when the patient presented to the hospital. Likewise, add-on surgeries were attributed to the shift in which they were scheduled, not performed. Each call shift lasted 24 hours in duration, following a 7:00 a.m.–7:00 a.m. schedule. At this residency program, one attending surgeon and two residents were assigned to each call shift, including a junior resident (either a PGY-2 or a PGY-3), who is always in-house and responds to every consult, and a PGY-5 resident, who primarily provides support as needed. For this study, shifts were only attributed to the junior resident on call. A typical monthly call schedule for each junior resident includes six shifts per month with at least one shift required to fall on a weekend. A seventh shift was added to one resident on months with 31 days. Among junior residents, PGY-3s were able to choose their call days before the PGY-2s each month.
Weather patterns included the average daily temperature, the presence of sun, and the presence of rain or snow, each of which were recorded from publicly accessible weather data from the National Oceanic and Atmospheric Administration.15 The presence of sun was defined as days that were partly sunny or sunny. Seasons were classified by meteorological definitions, with spring beginning on March 1, summer beginning on June 1, fall beginning on September 1, and winter beginning on December 1. A total of seven major holidays were considered, including Thanksgiving, Christmas Eve and Day, New Year’s Eve, the Fourth of July, Labor Day, and Memorial Day.
Statistical Analysis
Normality testing was initially performed on all results using the Shapiro-Wilk test. Nonparametric data were analyzed using the Mann-Whitney U test to compare two groups and the Kruskal-Wallis test to compare multiple groups. When the Kruskal-Wallis test revealed significance, Dunn’s post hoc test for multiple comparisons was performed to identify individually significant differences. The Spearman correlation coefficient was used to determine correlations between average daily temperatures and outcome variables. The alpha level for statistical significance was set as a P value < 0.05, and all reported tests were two-sided. Statistical analysis was performed using GraphPad Prism version 9.4.1 (GraphPad Software Inc, San Diego, CA, USA).
RESULTS
Residents and Attendings
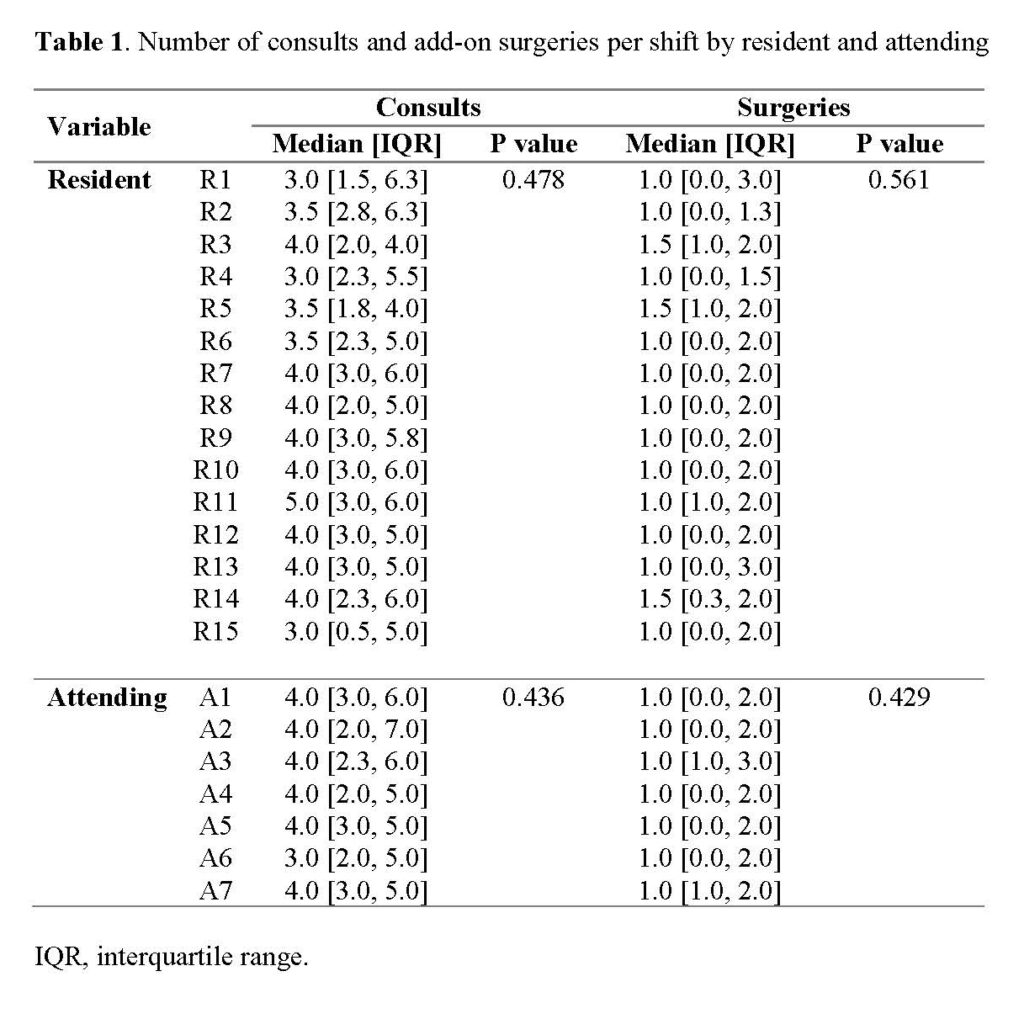
A total of 632 call shifts were included, with a total of 2539 consults and 857 add-on surgeries. Among our 15 residents and seven attending surgeons, the overall median number of consults/shift was 4.0 (IQR = 3.0, 5.25), which ranged from 0-12 overall, and the median number of add-on surgeries/shift was 1.0 (IQR = 0.0, 2.0), which ranged from 0-7. Among residents, the median number of consults/shift ranged from 3.0-4.0, while median add-on surgeries/shift ranged from 1.0-1.5. For attending surgeons, median consults/shift ranged from 3.0-4.0, while median add-on surgeries/shift was consistently 1.0. No significant associations were found between individual residents or attending physicians and the number of consults/shift (p = 0.478; p = 0.436, respectively) or add-on surgeries/shift (p = 0.561; p = 0.429) (Table 1).
Seasons, Months, and Days of the Week
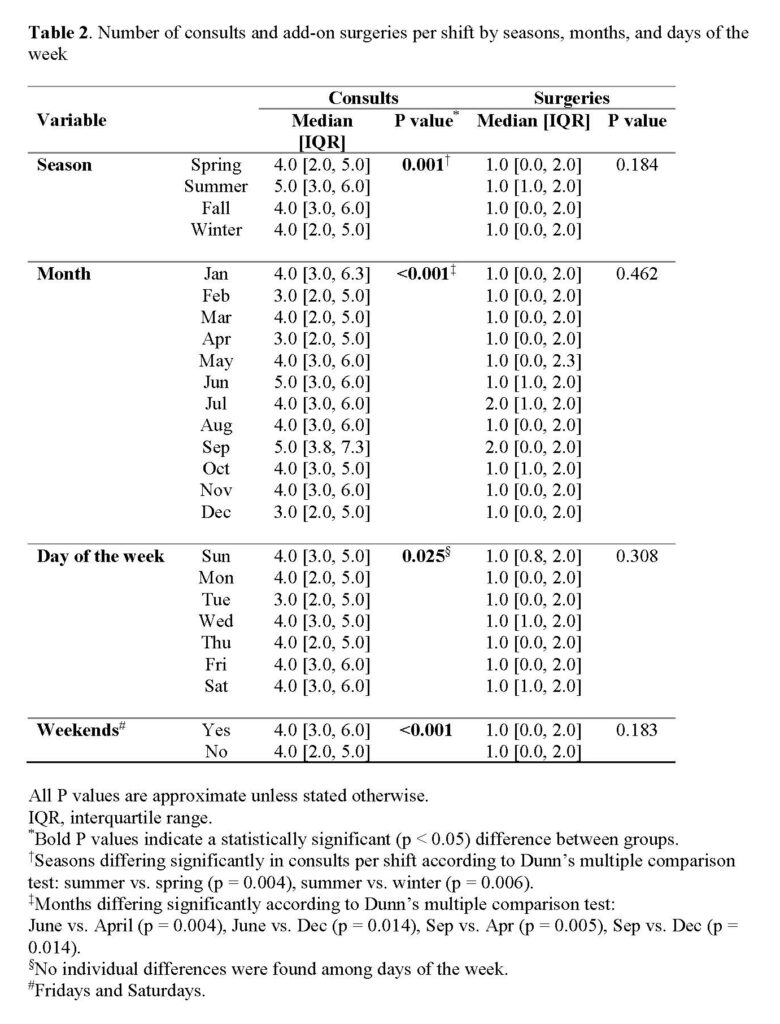
Seasons and months were both significantly associated with the number of consults/shift (p = 0.001; p = <0.001), but not the number of add-on surgeries/shift (p = 0.184; p = 0.462) (Table 2). The summer season had the highest number of consults/shift (5.0 [3.0, 6.0]), which was significantly higher than both spring (4.0 [2.0, 5.0]; p = 0. 004) and winter (4.0 [2.0, 5.0]; p = 0.006) according to post-hoc testing for individual differences. Among specific months, June and September were each associated with more consults/shift compared to both April and December. Day of the week was also associated with the number of consults/shift (p = 0.025), but not add-on surgeries/shift (p = 0.308). However, post-hoc analysis did not reveal any individual differences between days for either outcome. When grouping Fridays and Saturdays as weekends, these days had a significantly higher number of consults/shift compared to weekdays (4.0 [3.0-6.0] vs. 4.0 [2.0-5.0]; p = <0.001). Add-on surgeries/shift did not differ between weekends and weekdays (1.0 [0.0, 2.0] vs. 1.0 [0.0, 2.0]; p = 0.183).
Weather
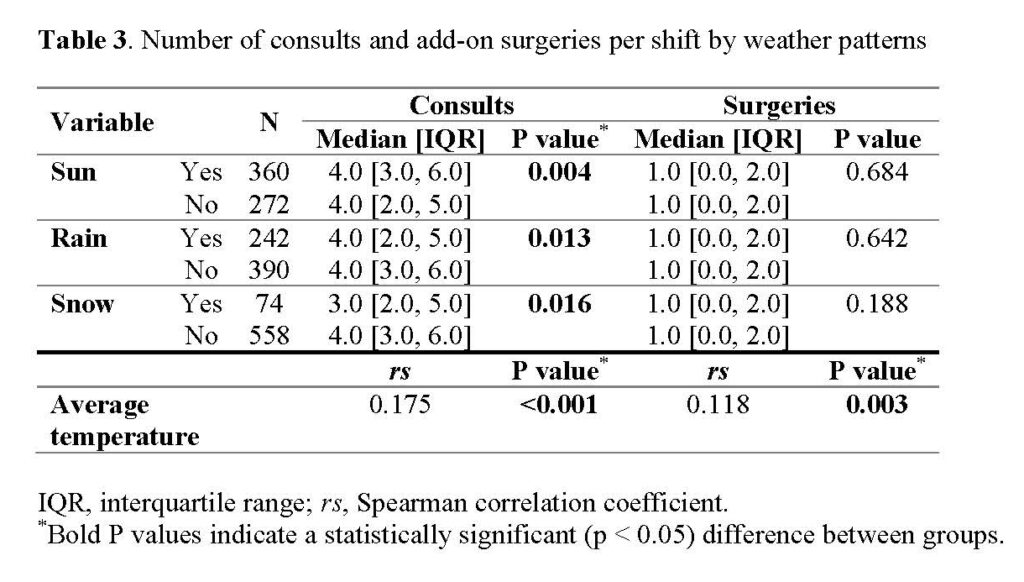
Results among weather patterns are shown in Table 3. Sunny weather accounted for 60.0% of shifts, while rain was documented in 38.3% and snow occurred during 11.7% of shifts. Sunny days were associated with a significantly higher number of consults/shift (4.0 [3.0, 6.0]; p = 0.004) while rain (4.0 [2.0, 5.0]; p = 0.013) and snow (3.0 [2.0, 5.0]; p = 0.016) resulted in fewer consults/shift. No significant associations were observed between add-on surgeries/shift and sun, rain, or snow (p = 0.684; p = 0.642; p = 0.188). Average daily temperature showed a significant yet weak correlation with both consults (rs = 0.175; p = <0.001) and add-on surgeries (rs = 0.118; p = 0.003) per shift.
Holidays and Full Moons
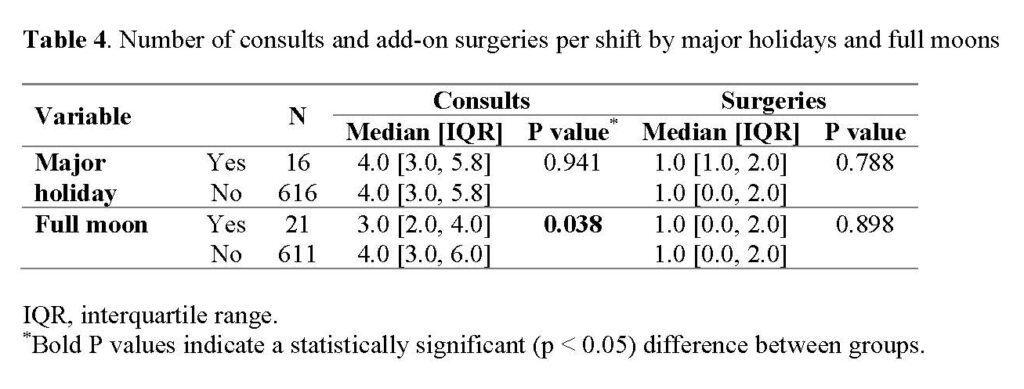
Sixteen shifts fell on major holidays (2.5%) and 21 occurred during a full moon (3.3%). Shifts that fell on a full moon were significantly associated with more consults/shift (3.0 [2.0, 4.0]; p = 0.038), but not with add-on surgeries (p = 0.898). No differences were observed in consults/shift or add-on surgeries/shift in relation to major holidays (p = 0.941; p = 0.898, respectively) (Table 4).
DISCUSSION
A number of factors may influence how busy an orthopedic surgeon is during his or her call shifts and it has been shown that individual residents or faculty are often believed to be “black clouds” in residency programs. By evaluating a total of 632 call shifts among 22 resident and attending physicians at a Level I trauma center, our hypothesis was validated that the individual on call was not associated with the volume of consults or add-on surgeries per shift. Instead, days of the week, months, seasons, and weather patterns all influenced how busy the on-call orthopedic surgeons were.
Anecdotally, the perception of a “black cloud” resident remains common and may be more closely related to one’s personality, ability to work well with others, or current stresses rather than his or her workload. Tanz & Charrow9 investigated this notion among pediatrics residents, finding lack of sleep as the major predictor of perceived workload while on call. However, they found no association between perceived workload and actual workload, including in residents who were thought of as a “black cloud.” A resident’s perceived workload may be related to higher acuity and greater heterogeneity of cases,18 which may contribute to the attribution of a “black cloud” label. Declaring a fellow resident or faculty member as a “black cloud” is quite prevalent,2,4,5 yet evidence supporting these beliefs is overwhelmingly lacking.2-9 This unfounded belief can have a lasting detrimental impact on a resident’s professional reputation, and dispelling this notion is important to ensure equitable treatment of trainees. The number of consults and add-on surgeries/shift were distributed relatively evenly among the residents and attending surgeons in our cohort, and no statistically significant differences were found among individuals. Similar to findings in other medical specialties, the results of our study indicate that a “black cloud” phenomenon does not influence the quantitative workload of an orthopedic surgery resident or attending surgeon.
Our findings do, however, suggest an association between calendar variables and associated workload. The calendar alone may thus play a more influential role on the orthopedic trauma volume during a given shift. We found significant differences in the total number of consults related to the day of the week, month of the year, and season. In particular, weekends demonstrated a higher number of consults/shift when compared to weekdays. This is consistent with the literature, as weekends have been shown to have a higher incidence of trauma presentations.17,18 We suspect this is likely related to people having an extended period of free time and thus more opportunities for injury. However, the type of injury and injury severity may vary by day of the week. For instance, Atherton et al.19 documented a higher incidence of low-energy femoral neck fractures earlier in the week. According to data from the National Safety Council, the highest incidence of fatal motor vehicle accidents occurs on Saturdays, whereas nonfatal crashes are more common during the week.20 This trend may help explain our finding of more consults/shift on weekends, as lower-energy ED presentations during the week may not be severe enough to necessitate a formal orthopedic consult compared to higher severity trauma which occurs more commonly over the weekend.
Summer months have been consistently associated with an increased volume of general and orthopedic trauma.13,18,21-23 We found summer to have the highest incidence of consults/shift, with June in particular yielding higher numbers than December and April. Especially in temperate climates, summer ushers in a period of warm weather which encourages more time outdoors and off work, and accordingly, more opportunities for injury. This may be especially pronounced in the pediatric population, which has been shown to have higher volumes of orthopedic trauma in the summer.17 However, this is nothing new to the orthopedic surgery resident, as the beginning of the academic year on July 1st is commonly known to coincide with the height of orthopedic trauma season.
We found daily variations in weather to be associated with the number of consults/shift, which included higher volume on predominantly sunny days, and fewer consults/shift on days with rain or snow. Average temperature was weakly correlated with both consults and add-on surgeries. A positive, strong correlation has been well-documented between higher daily temperature and trauma volume, as well as the presence of sunshine.13,19,21,24-27 While more consults on warmer days would help explain the increased volume in summer months, the effects of weather patterns have been less clearly defined in the literature. Numerous authors have found precipitation to be negatively associated with trauma volume,12,13,17,19,28 while others have documented a positive correlation.26,27 Precipitation may discourage people from venturing outside, yet it may also create adverse driving conditions or environments conducive for falls. For instance, a study from Minnesota, USA found that women aged 45-74 years old had an increased risk of hip fractures on days with snow or freezing rain,29 which may be a unique risk to northern climates. Others studies have shown increased incidence of distal radius fractures on days with snow.30-33 Our study was conducted in a region that regularly sees snow throughout the winter season, which we believe strengthens the negative correlation found between snow and consults/shift and ultimately suggests that snowfall may in fact act as a deterrent to orthopedic trauma.
Additional superstitions have been well documented in the literature, yet scientific evidence remains limited for any clinical relationship. Superstitions related to a full moon have postulated physiologic correlations as well,34 yet it is unclear whether this phenomenon influences human behavior in a meaningful way. Studies that have investigated nights with a full moon have found no increases in variables related to orthopedic care, including dog bites,35 traffic accidents,36 major trauma,37 or ED patient volume.10 However, one study found a decreased incidence in general trauma patients treated in the ED during a full moon.28 Similar to this study, we found the presence of a full moon to be associated with fewer consults/shift. Of note, only 21 shifts with full moons were included, so it remains uncertain whether this finding represents a clinically significant phenomenon.
This study, and the associations drawn, are not without limitations. The purpose of this study was to analyze factors that influence the sheer volume of orthopedic surgery consults and resultant add-on cases among on-call physicians, rather than the clinical outcomes for their patients. As such, this study’s broad objectives did not factor in the severity of each case, which may be influenced by the variables tested. Patient medical records were not examined, therefore, potential covariables such as patient age, comorbidity, and injury pattern were not included. It was thought that the number of add-on surgeries/shift would provide a measure of shift severity, however, future research should include the degree of consult severity in their analysis. Another limitation is the number of consults/shift may be low relative to other Level I trauma centers, which may decrease the overall power of our analysis. There may also be an aspect of delay in timing of consult notification that affects the shift to which a given consult is attributed. For instance, if a patient comes in overnight, but orthopedic surgery is not consulted until 8:00 a.m., this consult may not be accurately attributed to variables that may have influenced the initial injury. Furthermore, the daily duration of sun and volume of precipitation were not recorded, which may have omitted a more specific relationship with these variables.
Overall, the results of this study provide valuable insights into the factors that can influence the number of orthopedic surgery consults and add-on surgeries during call shifts at a Level I trauma center. The findings suggest that temporal factors such as the day of the week, month of the year, and season, as well as weather patterns and certain superstitions, may have an impact on the number of consults and add-on surgeries. From a resident’s perspective, this information supports the use of balanced call schedules to a feasible extent, with call experience encompassing both weekends and weekdays. These findings may even be useful in optimizing clinical support during high volume days or months of the year. The tendency for residents to maintain superstitions may transcend published data, but those self-attributed “black clouds” can rest assured that they are not being targeted by orthopedic trauma.
In conclusion, multiple temporal and weather-related factors appear to be associated with the number of consults per shift in an orthopedic surgery residency program, but a “black cloud” resident or attending physician was not one of them.
TABLES
REFERENCES
- Coombs RH, Chopra S, Schenk DR, Yutan E. Medical slang and its functions. Soc Sci Med 1993;36:987-998. doi:10.1016/0277-9536(93)90116-l
- Naidech A, Parekh N, Kahn M. Superstitions of house officers. Resident and Staff Physician 2004;50:47-49.
- Fabre A, Mancini J. Jinx or Not?: There Is Nothing Like a “Black Cloud” Syndrome. Pediatr Emerg Care 2017;33:686-689. doi:10.1097/PEC.0000000000000663
- Melzer J. Clouds of different colors: A prospective look at head and neck surgical resident call experience. Ear Nose Throat J 2017;96:E19-e24. doi:10.1177/014556131709601205
- Meyr AJ, Gonzalez O, Mayer A. Quantification and perception of on-call podiatric surgical resident workload. J Foot Ankle Surg 2011;50:535-536. doi:10.1053/j.jfas.2011.04.035
- Ong LW, Dawson JD, Ely JW. Black Clouds vs Random Variation in Hospital Admissions. Fam Med 2018;50:444-449. doi:10.22454/FamMed.2018.555558
- Pham HP, Raju D, Jiang N, Williams LA. “Black cloud” vs. “white cloud” physicians – Myth or reality in apheresis medicine? J Clin Apher 2017;32:235-239. doi:10.1002/jca.21503
- Schissler AJ, Einstein AJ. Have the ‘black clouds’ cleared with new residency programme regulations? Intern Med J 2016;46:734-736. doi:10.1111/imj.13076
- Tanz RR, Charrow J. Black clouds. Work load, sleep, and resident reputation. Am J Dis Child 1993;147:579-584. doi:10.1001/archpedi.1993.02160290085032
- Thompson DA, Adams SL. The full moon and ED patient volumes: unearthing a myth. Am J Emerg Med 1996;14:161-164. doi:10.1016/S0735-6757(96)90124-2
- Ali AM, Willett K. What is the effect of the weather on trauma workload? A systematic review of the literature. Injury 2015;46:945-953. doi:10.1016/j.injury.2015.03.016
- Ho VP, Towe CW, Chan J, Barie PS. How’s the weather? Relationship between weather and trauma admissions at a Level I Trauma Center. World J Surg 2015;39:934-939. doi:10.1007/s00268-014-2881-8
- Wilson JM, Staley CA, Boden AL, Boissonneault AR, Schwartz AM, Schenker ML. The Effect of Season and Weather on Orthopaedic Trauma: Consult Volume Is Significantly Correlated with Daily Weather. Adv Orthop 2018;2018:6057357. doi:10.1155/2018/6057357
- Zhao E, Tiedeken N, Wang W, Fowler J. The Black Cloud Phenomenon in Hand Surgery. Hand (N Y) 2019;14:819-822. doi:10.1177/1558944718770206
- NOAA Online Weather Data. Available at: https://www.weather.gov/wrh/Climate?wfo=cle. Accessed 1 April, 2022.
- Haney EM, Nicolaidis C, Hunter A, Chan BK, Cooney TG, Bowen JL. Relationship between resident workload and self-perceived learning on inpatient medicine wards: a longitudinal study. BMC Med Educ 2006;6:35. doi:10.1186/1472-6920-6-35
- Livingston KS, Miller PE, Lierhaus A, Matheney TH, Mahan ST. Does Weather Matter? The Effect of Weather Patterns and Temporal Factors on Pediatric Orthopedic Trauma Volume. Open Orthop J 2016;10:550-558. doi:10.2174/1874325001610010550
- Pape-Köhler CI, Simanski C, Nienaber U, Lefering R. External factors and the incidence of severe trauma: time, date, season and moon. Injury 2014;45 Suppl 3:S93-99. doi:10.1016/j.injury.2014.08.027
- Atherton WG, Harper WM, Abrams KR. A year’s trauma admissions and the effect of the weather. Injury 2005;36:40-46. doi:10.1016/j.injury.2003.10.027
- Crashes by Time of Day and Day of Week. Available at: https://injuryfacts.nsc.org/motor-vehicle/overview/crashes-by-time-of-day-and-day-of-week/#:~:text=On%20average%20in%202021%2C%20fatal,on%20weekdays%2C%20peaking%20on%20Friday. Accessed 4 May, 2022.
- Agar A, Sahin A, Gunes O, Gulabi D, Erturk C. Seasonal variation in paediatric orthopaedic trauma Patients – A single centre experience from Turkey. Journal of Orthopaedic Surgery 2022;30. doi:10.1177/23094990211068146
- Shukla R, Jain N, Agarwal U, Sheikh T, Jain R. Seasonal variation in orthopedic trauma patients-An experience from central India. J Clin Orthop Trauma 2018;9:S40-s43. doi:10.1016/j.jcot.2017.07.009
- Waldron J, Denisiuk M, Sharma R, Boura J, Afsari A, Best B. Does seasonal variation in orthopaedic trauma volume correlate with adverse hospital events and burnout? Injury 2022;53:2053-2059. doi:10.1016/j.injury.2022.02.042
- Kim Y, Kim H, Shin SD, Hong YC. Different influence of outdoor temperature on traumatic and nontraumatic injuries. J Trauma Acute Care Surg 2012;73:944-949. doi:10.1097/TA.0b013e318256de02
- O’Connor ZJ, Helmer SD, Yates CL, Ward JG, Khandelwal A, Haan JM. An evaluation of the effect of wind speed on trauma admissions and injury severity at a midwest level I trauma center. Am Surg 2012;78:614-616.
- Parsons N, Odumenya M, Edwards A, Lecky F, Pattison G. Modelling the effects of the weather on admissions to UK trauma units: a cross-sectional study. Emerg Med J 2011;28:851-855. doi:10.1136/emj.2010.091058
- Rising WR, O’Daniel JA, Roberts CS. Correlating weather and trauma admissions at a level I trauma center. J Trauma 2006;60:1096-1100. doi:10.1097/01.ta.0000197435.82141.27
- Stomp W, Fidler V, ten Duis HJ, Nijsten MW. Relation of the weather and the lunar cycle with the incidence of trauma in the Groningen region over a 36-year period. J Trauma 2009;67:1103-1108. doi:10.1097/TA.0b013e3181986941
- Jacobsen SJ, Sargent DJ, Atkinson EJ, O’Fallon WM, Melton LJ. Population-based study of the contribution of weather to hip fracture seasonality. Am J Epidemiol 1995;141:79-83. doi:10.1093/oxfordjournals.aje.a117348
- Flinkkilä T, Sirniö K, Hippi M, Hartonen S, Ruuhela R, Ohtonen P, et al. Epidemiology and seasonal variation of distal radius fractures in Oulu, Finland. Osteoporos Int 2011;22:2307-2312. doi:10.1007/s00198-010-1463-3
- Giladi AM, Shauver MJ, Ho A, Zhong L, Kim HM, Chung KC. Variation in the incidence of distal radius fractures in the U.S. elderly as related to slippery weather conditions. Plast Reconstr Surg 2014;133:321-332. doi:10.1097/01.prs.0000436796.74305.38
- Jantzen C, Jørgensen HL, Thomsen MT, Riis T, Sommer B, Duus BR, et al. Daily number of fractures is associated with road temperature in an urban area. Dan Med J 2014;61:A4794.
- Weston-Simons J, Jack CM, Doctor C, Brogan K, Reed D, Ricketts D. The impact of snow on orthopaedic trauma referrals. Injury 2012;43:1033-1036. doi:10.1016/j.injury.2011.12.018
- Zimecki M. The lunar cycle: effects on human and animal behavior and physiology. Postepy Hig Med Dosw (Online) 2006;60:1-7.
- Chapman S, Morrell S. Barking mad? another lunatic hypothesis bites the dust. Bmj 2000;321:1561-1563. doi:10.1136/bmj.321.7276.1561
- Laverty WH, Kelly IW. Cyclical calendar and lunar patterns in automobile property accidents and injury accidents. Percept Mot Skills 1998;86:299-302. doi:10.2466/pms.1998.86.1.299
- Coates W, Jehle D, Cottington E. Trauma and the full moon: a waning theory. Ann Emerg Med 1989;18:763-765. doi:10.1016/s0196-0644(89)80014-9
