
Nicholas Brott, DO1; Alexander Fischbach, DO1; Matthew Spittler, DO1; Collin Haben, DO1; Steven Jackson, DO1; and Corey Diemer, DO2
1Western Reserve Hospital
2ATSU-Kirksville College of Osteopathic Medicine
Abstract
Introduction
Hip and knee arthroplasties are common procedures within orthopedics, with over 2.5 million hip and knee arthroplasties done in the United States from 2021-2022 (1). While there has been an increase in the total number of hip and knee arthroplasties in an increasingly younger population, the vast majority of patients are older, and therefore inherently have more risks associated with surgery (2). As surgical implants and techniques continue to improve, there was an interest in performing a study to identify modalities to improve postoperative care. Specifically, the goal of this study was to determine if administration of intravenous steroids given during and after total hip and knee arthroplasties lead to decreased use of narcotic pain medication and earlier discharges from the hospital in a community hospital setting. Both of these endpoints are believed to be indicative of how well pain is managed and how soon patients are able to mobilize more effectively, decreasing complications, and improving outcomes.
Methods
This study was conducted over a ten-month period at a community hospital in northeast Ohio. The control group included patients undergoing elective primary total hip and knee arthroplasties over a four-month span. The steroid group included all patients undergoing elective primary hip and knee arthroplasties over a six-month span that received three total doses of 10 mg IV dexamethasone (one intraoperative and two more postoperative eight hours apart). All procedures were performed by the same arthroplasty fellowship trained orthopedic surgeon at the same facility. All hip arthroplasties were performed through a posterior approach, and all knee arthroplasties through a medial parapatellar approach. All aspects of care were attempted to be kept as consistent as possible.
Results
It was hypothesized that the group receiving IV steroids would require less narcotic pain medication (calculated using MME) in the first 24 hours postoperative and would discharge sooner from the hospital. The results did not show a significant difference in narcotic pain medication in the first 24 hours (73.15 MME in control group, 72.69 in steroid group) but did demonstrate a statistically significantly decreased length of stay (2.74 days in control group, 1.88 in steroid group) as can be seen in Figure 1 and 2. Conclusion
These findings demonstrate that there likely is benefit from implementing IV steroids in the pain regimen for hip and knee arthroplasty patients.
Keywords: Steroids, length of stay, arthroplasty, perioperative
Introduction
Hip and knee arthroplasties are common procedures within orthopedics. Over 2.5 million hip and knee arthroplasties were done in the United States from 2012-2022 (1). The number of arthroplasties will continue to increase. One of the major considerations in joint arthroplasty is pain control due to the inherent pain that most patients experience postoperatively. Many surgeons employ a multimodal pain management approach to decrease pain postoperatively. Opioid medication has been a mainstay in postoperative pain control; however opioid medications do not come without risks. IV corticosteroid use in total joint arthroplasty has been studied to decrease nausea, vomiting, pain, and swelling postoperatively. Multiple studies have demonstrated the benefit of using perioperative steroids in total joint arthroplasty (3). Multiple doses of steroids have been found to be beneficial in reducing pain, decreasing time to ambulation, and decreasing length of stay in total hip arthroplasty (4).
The aim of this study is to determine if perioperative dexamethasone administration reduces inpatient opioid use, and length of hosptial stay for postoperative primary total joint arthroplasty patients in a community hospital.
Materials and Methods
This study utilizing retrospective chart review took place over a ten month period at a community hospital in northeast Ohio. Based on the volume of total joint arthroplasties performed by the primary surgeon, ten months was the time frame dedicated as providing enough subjects for sufficient power for the study. This retrospective study was exempt from IRB approval. The steroid regimen in this study consisted of three 10mg doses of IV Dexamethasone. The first dose was given intraoperatively, the second dose 8 hours postoperative, and the third dose 16 hours postoperative. Inclusion criteria for the study were patients undergoing elective primary total hip and knee arthroplasty performed by a single arthroplasty fellowship trained orthopedic surgeon at the same community hospital. Patients were excluded from this investigation if their surgery was a revision total knee or total hip arthroplasty, or if the procedure was performed for the management of a fracture. Patients were also excluded if they had been taking opioids routinely prior to surgery, most commonly from a pain management practice. Lastly, insulin-dependent diabetic patients were excluded to decrease the risk of adverse events related to the hyperglycemic inducing effect of steroids.
Data was collected through retrospective chart review during the timeframe of the study. Outcome measures collected included: patient demographics, procedure, pain medication received during the first 24 hours postoperatively, and length of stay (midnights). Narcotic pain medication usage was determined utilizing morphine milligram equivalents as dictated by UCSF pain management education sources (5). At this institution and this study, all total hip and knee arthroplasty patients spend at least one midnight in the hospital, not performing same day discharges.
The control group of this study consisted of patients undergoing total joint arthroplasty prior to implementation of our steroid regimen, dedicated as the patients who underwent primary total knee and hip arthroplasty from June through September of 2023. The group that received IV steroids were patients that underwent primary elective total hip and knee arthroplasties between October 2023 and March 2024. All aspects of preoperative, intraoperative, and postoperative care were attempted to be maintained as constant between the two groups.
Our study focused on outcome measures during the first 24 hours postoperatively, because this is theoretically when steroids would have the biggest effect. However, there is data that suggests extended use of steroids could be beneficial for patients (6).
Results
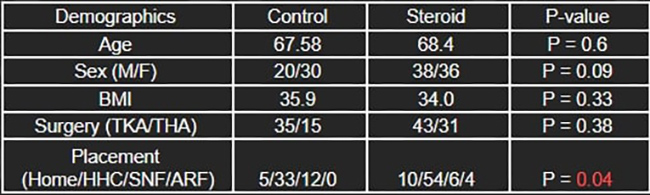
This study included 124 total joint arthroplasty patients (M = 58; F = 66). Patients were divided into control groups (n = 50) and a steroid group (n = 74). Demographic variables of age, sex, body mass index (BMI), and type of surgery (total knee arthroplasty [TKA] vs total hip arthroplasty [THA]), were similar between groups with no significant differences observed (Table 1). The only significant difference observed was in the Chi-squared analysis comparing discharge placement after total joint arthroplasty (p = 0.04). However, further analysis comparing patients who were discharged home or home with home health care, versus patients who were discharged to a skilled nursing facility or an acute rehab facility, did not reveal significant differences in discharge placement (p > 0.15) (Figure 1).

When examining the 24-hour postoperative MME used between patients who received IV steroids and those who did not, no significant difference was found (p = 0.94; Figure 2). Patients who received IV steroids had an average of 72.69 MME compared to controls who had received 73.15 MME (Table 2).


Postoperative steroid use was significantly associated with a shorter length of stay compared to control patients who did not received steroids (p < 0.01; Figure 3). Patients who received postoperative steroids had an average 1.8 day length of stay while control subjects had a 2.7 day length of stay, on average (Table 2).


Discussion
Perioperative steroid administrations in total joint arthroplasty patients are a well-established means of reducing opioid consumption in patients who undergo total joint arthroplasty and length of postoperative hospital stay (7-12). However, there is some conflicting evidence in the literature regarding its effect on MME length of hospital stay (13 -16). This investigation evaluated the impact of postoperative steroid administration on MME and length of stay after total joint arthroplasty in a community hospital setting. A majority of these investigations were conducted in large academic centers or include multi-center cohorts. Thus, there is a dearth of literature regarding the effect of perioperative steroid use on MME usage and length of stay in the community hospital setting after total joint arthroplasty.
Our main outcome measures of morphine milligram equivalents in the first 24 hours and length of stay had differing results. Morphine milligram equivalents for pain medication administered within 24 hours postoperative were found not to be different between the two groups. The control group had an average of 73.15 morphine milligram equivalents compared to 72.69 used in the steroid group. However, there was a difference in length of stay. Length of stay was 2.74 days in the control group and 1.88 days in the steroid group. This difference was found to be statistically significant with a p-value of < 0.01. This is likely explained by the steroids having an anti-inflammatory and anti-emetic effect allowing patients to ambulate and better work with physical therapy. With sooner and improved performance in physical therapy, patients are more likely to meet criteria for safe discharge at an earlier time.
An earlier discharge has numerous benefits, including decreased health care costs and lower complication risks. In a study by Salomon et al. In 2021, researchers found longer hospital stays to be correlated with increased risk of venous thromboembolisms, one of the more serious and common complications after lower extremity total joint arthroplasties (17). Additionally, a study performed by Demik et al. found that with increased length of stay there is a statistically significant increase in numerous complications in the first thirty days after surgery. These include superficial infection, wound infection, wound dehiscence, pulmonary embolism, pneumonia, urinary tract infection, stroke, myocardial infarction, and Clostridium difficile infection (18).
Our study showed a statistically significant shorter length of stay when IV steroids were administered in the intraoperative and postoperative period. Patients who received IV steroids discharged on average nearly 24 hours earlier. The percent difference in length of stay was 31.39% between the two groups (2.74 in control, 1.88 in steroid group). It is important to recognize there are several limitations to this study. Due to the heterogeneity of total joint arthroplasty, not all variables could be controlled. Several measures that were not taken into account were: intraoperative time, blood loss, medical comorbidities, regional blocks, spinal anesthetics. It was also not examined if there were any differences in physical therapy treatments between the two groups, though therapy was performed by hospital employed physical therapists with the same protocols throughout the study. There was also not a reliable way to track “time to ambulation” as an outcome measure postoperatively. Aside from administration of IV steroids, no other component of surgical care or postoperative care was altered.
Conclusion
From results of this study, there was found to be a statistically significant decrease in length of stay when IV steroids were administered in the initial 24 hours after primary total hip and knee arthroplasties. However, when looking at narcotic pain medication usage in the first 24 hours after surgery, there was not a statistically significant difference in morphine milligram equivalents between the two groups. While this end point was not statistically significant, the decreased length of stay does allow for the assumption of some advantages with IV steroid administration as patients were able to clear physical therapy earlier and be comfortable enough for discharge from the hospital sooner. As mentioned in the discussion, shorter lengths of stay plays a role in decreasing several complications in the first thirty days after surgery.
References
- American Joint Replacement Registry (AJRR): 2022 Annual Report. Rosemont, IL: American Academy of Orthopaedic Surgeons (AAOS), 2022. https://www.aaos.org/registries/publications/ajrr-annual-report/
- Katie St John, Andrew Hughes, Joseph Queally. A study of population trends and future projections for the hip and knee arthroplasty service in the Republic of Ireland, The Surgeon, Volume 23, Issue 4, 2025, Pages 216-219, ISSN 1479-666X. https://doi.org/10.1016/j.surge.2025.02.005.
- Hannon CP, Fillingham YA, Mason JB, et al. Corticosteroids in Total Joint Arthroplasty: The Clinical Practice Guidelines of the American Association of Hip and Knee Surgeons, American Society of Regional Anesthesia and Pain Medicine, American Academy of Orthopaedic Surgeons, Hip Society, and Knee Society. J Arthroplasty. 2022;37(9):1684-1687. doi:10.1016/j.arth.2022.03.043
- Lucero CM, García-Mansilla A, Zanotti G, Comba F, Slullitel PA, Buttaro MA. A Repeat Dose of Perioperative Dexamethasone Can Effectively Reduce Pain, Opioid Requirement, Time to Ambulation, and In-Hospital Stay After Total Hip Arthroplasty: A Prospective Randomized Controlled Trial. J Arthroplasty. 2021;36(12):3938-3944. doi:10.1016/j.arth.2021.08.020
- Calculation of oral morphine equivalents (ome) Pain Management Education at UCSF. Available at: https://pain.ucsf.edu/opioid analgesics/calculation-oral-morphine-equivalents-ome
- Lei Y, Huang Z, Huang Q, Huang W, Pei F. Repeat Doses of Dexamethasone up to 48 Hours Further Reduce Pain and Inflammation After Total Hip Arthroplasty: A Randomized Controlled Trial. J Arthroplasty. 2020;35(11):3223-3229. doi:10.1016/j.arth.2020.06.023
- Gasbjerg KS, Hägi-Pedersen D, Lunn TH, et al. Effect of dexamethasone as an analgesic adjuvant to multimodal pain treatment after total knee arthroplasty: randomised clinical trial. BMJ. 2022;376:e067325. Published 2022 Jan 4. doi:10.1136/bmj-2021-067325Meng J, Li L. The efficiency and safety of dexamethasone for pain control in total joint arthroplasty: A meta-analysis of randomized controlled trials. Medicine (Baltimore). 2017 Jun;96(24):e7126. doi: 10.1097/MD.0000000000007126. PMID: 28614232; PMCID: PMC5478317.
- Køppen KS, Gasbjerg KS, Andersen JH, Hägi-Pedersen D, Lunn TH, Mathiesen O. Systemic glucocorticoids as an adjunct to treatment of postoperative pain after total hip and knee arthroplasty: A systematic review with meta-analysis and trial sequential analysis. Eur J Anaesthesiol. 2023;40(3):155-170. doi:10.1097/EJA.0000000000001768
- Meng J, Li L. The efficiency and safety of dexamethasone for pain control in total joint arthroplasty: A meta-analysis of randomized controlled trials. Medicine (Baltimore). 2017;96(24):e7126. doi:10.1097/MD.0000000000007126
- Lex JR, Edwards TC, Packer TW, Jones GG, Ravi B. Perioperative Systemic Dexamethasone Reduces Length of Stay in Total Joint Arthroplasty: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Arthroplasty. 2021;36(3):1168-1186. doi:10.1016/j.arth.2020.10.010
- Yoshida B, Piple AS, Wang JC, Richardson MK, Christ AB, Heckmann ND. Perioperative Dexamethasone Associated With Decreased Length of Stay After Total Hip and Knee Arthroplasty. J Am Acad Orthop Surg. 2023;31(19):e778-e787. doi:10.5435/JAAOS-D-22-01146
- Alessio-Mazzola M, D’Andrea G, Abu-Mukh A, Mosca S, Placella G, Salini V. Effect of systemic steroids administration in the clinical outcome of total hip arthroplasty: a systematic review and meta-analysis of prospective randomized controlled trials. Arch Orthop Trauma Surg. 2024;145(1):78. Published 2024 Dec 21. doi:10.1007/s00402-024-05626-6
- Wang C, Luo C, Tang X, Luo L, Zeng Y, Zhang Y, Wang X. A systematic review and meta-analysis on how different dexamethasone administration regimes impact total joint arthroplasty outcomes. Front Pharmacol. 2025 Jul 3;16:1548126. doi: 10.3389/fphar.2025.1548126. PMID: 40678724; PMCID: PMC12267163.
- Arraut J, Thomas J, Oakley CT, Barzideh OS, Rozell JC, Schwarzkopf R. The AAHKS Best Podium Presentation Research Award: A Second Dose of Dexamethasone Reduces Postoperative Opioid Consumption and Pain in Total Joint Arthroplasty. J Arthroplasty. 2023 Jul;38(7 Suppl 2):S21-S28. doi: 10.1016/j.arth.2023.02.007. Epub 2023 Feb 10. PMID: 36775214.
- Ruberto RA, Farah O, Lopez C, Hickernell T. Perioperative Intravenous Glucocorticoids in Total Joint Arthroplasty: A Systematic Review. J Am Acad Orthop Surg. 2023;31(2):e94-e106. doi:10.5435/JAAOS-D-22-00232
- Li D, Wang C, Yang Z, Kang P. Effect of Intravenous Corticosteroids on Pain Management and Early Rehabilitation in Patients Undergoing Total Knee or Hip Arthroplasty: A Meta-Analysis of Randomized Controlled Trials. Pain Pract. 2018;18(4):487-499. doi:10.1111/papr.12637
- Salomon B, Dasa V, Krause PC, Hall L, Chapple AG. Hospital Length of Stay Is Associated With Increased Likelihood for Venous Thromboembolism After Total Joint Arthroplasty. Arthroplast Today. 2021;8:254-257.e1. Published 2021 Feb 24. doi:10.1016/j.artd.2020.12.025
- DeMik DE, Carender CN, An Q, Callaghan JJ, Brown TS, Bedard NA. Longer Length of Stay Is Associated With More Early Complications After Total Knee Arthroplasty. Iowa Orthop J. 2022;42(2):53-59.
