
Derek Renner, DO
Western Reserve Hospital, Orthopedic Department
DOI: http://doi.org/10.70709/axe77rmd
Keywords: Trigger Finger, Attritional Tearing flexor tendons, steroid injections
Introduction
Stenosing tenosynovitis, commonly known as trigger finger, is a condition characterized by the inability to smoothly flex and extend a digit due to impingement of the flexor tendon by the first annular ligament (A1 pulley). This is commonly thought to be the result of repetitive use and inflammation. Clinical manifestations include tenderness to palpation, a palpable nodule at the base of the affected digit, and pain, catching, or locking during finger movement. Trigger finger can affect individuals of all ages and activity levels, with a higher prevalence observed in certain demographic groups such as women and individuals with comorbid conditions like diabetes and inflammatory diseases.
While conservative management options such as anti-inflammatories, splinting and corticosteroid injections are often effective initial therapies, advanced or refractory cases may require surgical intervention. Corticosteroid use can result in tendon weakening, a phenomenon known as corticosteroid-induced tendinopathy. This is thought to occur via several mechanisms. For one, corticosteroids have been shown to weaken tendons by inhibiting the synthesis of collagen1. Secondly, corticosteroids alter the activity of matrix metalloproteinases (MMPs) which may affect tendon integrity 1,2. Lastly, corticosteroids can inhibit cell proliferation and induce necrosis/apoptosis, which can lead to further atrophy and weakening of the tendon and structures surrounding the injection site 3-5.
The presence of attritional tears within the flexor tendon sheath have been observed during surgical exploration or imaging studies in patients with trigger finger, with the current literature describing multiple individual case reports indicating tendon rupture after corticosteroid injection. A review of the literature showed multiple individual case reports of tendon rupture following corticosteroid injections in the hand. Such reports include rupture of the extensor pollicis longus, flexor pollicis longus, flexor digitorum profundus and superficialis, as well as multiple pulley ruptures in the hand after steroid injection6-12. However, a study showing a relationship between injections and tendon rupture in the hand has not been performed to our knowledge.
Our primary goal was to analyze whether trigger finger injections are related to attritional tearing of the flexor tendons seen intra-operatively. To investigate the relationship between trigger finger injections and attritional flexor tendon tearing. Data from operative trigger finger releases from the past 5 (2019-2023) were retrieved and the charts were reviewed to determine whether intraoperative tearing was found. Clinic notes were also reviewed to determine the amount of injections performed for the affected digit.
Materials and Methods
Data from the past 5 years of operative cases at the primary hospital were retrieved. There were a total of 343 cases from the last 4 years that were reviewed. Over 90% of those cases were performed by the primary upper extremity trained orthopedic surgeon at the primary institution, the others were performed by 3 other orthopedic surgeons. All of the trigger finger injections were performed by the primary surgeon. Operative notes and reports from 2019-2023 were reviewed for intra-operative record of attritional tearing with or without repair. Every patient’s clinic records were also reviewed for number of trigger finger injections in each affected digit. With this information, statistical analysis was performed to examine whether there was any correlation between number of trigger finger injections and attritional tearing seen intra-operatively. Other variables considered were age, number of digits affected, and which digit was affected.
Results
In total there were 343 trigger finger releases performed from 2019-2023. The digits are labeled Left (L) or Right (R), and 1-5 corresponding to the thumb (1), index (2), long (3), ring (4), and little (5) fingers. The right R1 and R3 were most affected at 61 and 64 affected digits respectively. Left L1 and L3 were close behind at 46 and 57 respectively. Interestingly, L2, L5, R2, and R5 were significantly less affected at 7, 5, 15, and 11.
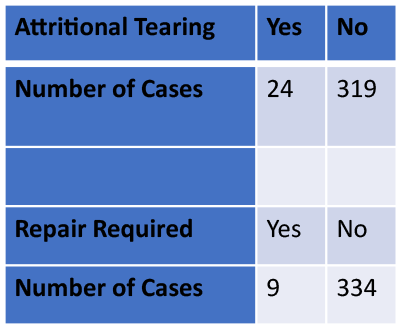
Of the 343 cases, 24 had attritional tearing, and 9 of those cases required repair using 4-0 Ticron in a running locking fashion. Decision to repair was made intraoperatively based on how the flexor tendons looked, as well as the percentage of the tendon that was viable. This varied greatly depending on the size of the tendon and amount of tendinosis. Current literature indicates that flexor tendons should be repaired with greater than 60-75% tendon disruption in cases of laceration13-14. These guidelines were loosely followed during repair, though the mechanism of injury is not laceration. Consideration was also given to the size of the tendon and need for tubularization via a running locking suture. Persistent triggering after trigger finger release can in certain cases be managed with excision of the flexor tendons to improve gliding. In cases of tendon disease, we preferred repair with retention of as much tendon as possible. From our review, 14 of the cases of attritional tearing had no trigger finger injections in the affected digit. 5 digits with tearing seen intra-operatively had 1 injection, 3 digits had 2 injections, 1 had 3 injections, and 1 had 4 injections total. Statistical analysis was performed using Chi-Squared test and showed no significant association between number of injections and attritional tearing of the flexor tendons seen intra-operatively. There was also no association with attritional tearing requiring repair.




Discussion
The results show no statistical significance between number of corticosteroid injections into a finger and attritional tearing seen intraoperatively. With only 24 cases of attritional tearing, a larger sample size of attritional tears would make the power of the study stronger. Next steps might involve completing the chart review for years 2014-2018. We also found it interesting that L1, L3, R1 and R3 were the most affected digits by a large number. There may be an explainable cause for this related to anatomy and physiology or amount of use for those digits, but we did not investigate further. We noticed in the cases of attritional tearing there were often comorbidities such as poorly controlled diabetes, Dupuytren disease, and other autoimmune conditions. Looking into specific comorbidities and their severity may be beneficial to identify which patients are more likely to have tearing.
While our study did not show any association between corticosteroid injections for trigger finger and attritional tearing identified intra-operatively, there may still be an association. We know there have been cases of tendon rupture in the hand after steroid injection as outlined previously. There may be some effect of the steroid on the tendon itself, but attritional tearing may likely be multifactorial, with duration of disease and medical comorbidities that affect the hand also playing an indeterminate role.
Shortcomings of the study are that a single surgeon performed all of the trigger finger injections and repair of flexor tendons seen intra-operatively. The decision to repair was also somewhat subjective, with no definite decision point for repair. This decision was made based on amount of tearing, tendinosis, and dynamic assessment of tendon gliding intra-operatively. To further investigate the effect of trigger finger injections on the tendons themselves, it would be beneficial to obtain a larger amount data prospectively, tracking number of injections and the intraoperative findings from multiple institutions. It may also be beneficial to develop a definite grading system for tearing to include percentage of tendinosis, tear morphology (longitudinal, split, attritional) that could make the findings more standardized.
References
- Dean, B. J., Lostis, E., Oakley, T., Rombach, I., Morrey, M. E., and Carr, A. J. “The Risks and Benefits of Glucocorticoid Treatment for Tendinopathy: A Systematic Review of the Effects of Local Glucocorticoid on Tendon.” Seminars in Arthritis and Rheumatism, vol. 43, no. 2, Feb. 2014, doi:10.1016/j.semarthrit.2013.08.003. PMID: 24074644.
- Del Buono, A., Oliva, F., Osti, L., and Maffulli, N. “Metalloproteases and Tendinopathy.” Muscles, Ligaments and Tendons Journal, vol. 3, no. 1, Jan. 2013, pp. 51–57, PMID: 23885345.
- Spang, Christoph, Jialin Chen, and Ludvig J. Backman. “The Tenocyte Phenotype of Human Primary Tendon Cells in Vitro Is Reduced by Glucocorticoids.” BMC Musculoskeletal Disorders, vol. 17, no. 1, 2016, doi:10.1186/s12891-016-1328-9. PMID: 27832770, PMCID: PMC5105245.
- Wong, M. W., Tang, Y. Y., Lee, S. K., Fu, B. S., Chan, B. P., and Chan, C. K. “Effect of Dexamethasone on Cultured Human Tenocytes and Its Reversibility by Platelet-Derived Growth Factor.” The Journal of Bone and Joint Surgery. American Volume, vol. 85, no. 10, Oct. 2003, pp. 1914–1920, PMID: 14563798.
- Scutt, N., Rolf, C. G., and Scutt, A. “Glucocorticoids Inhibit Tenocyte Proliferation and Tendon Progenitor Cell Recruitment.” Journal of Orthopaedic Research: Official Publication of the Orthopaedic Research Society, vol. 24, no. 2, Feb. 2006, pp. 173–182, PMID: 16435354.
- Cigna, E., Özkan, Ö., Mardini, S., Chiang, P. T., Yang, C. H., and Chen, H. C. “Late Spontaneous Rupture of the Extensor Pollicis Longus Tendon after Corticosteroid Injection for Flexor Tenosynovitis.” European Review for Medical and Pharmacological Sciences, vol. 17, no. 5, Mar. 2013, pp. 689–692, PMID: 23609371.
- Fitzgerald, B. T., Hofmeister, E. P., Fan, R. A., and Thompson, M. A. “Delayed Flexor Digitorum Superficialis and Profundus Ruptures in a Trigger Finger after a Steroid Injection: A Case Report.” The Journal of Hand Surgery, vol. 30, no. 3, May 2005, pp. 479–481, PMID: 15925155.
- Gyuricza, C., Umoh, E., and Wolfe, S. W. “Multiple Pulley Rupture Following Corticosteroid Injection for Trigger Digit: Case Report.” The Journal of Hand Surgery, vol. 34, no. 8, Oct. 2009, pp. 1417–1419, PMID: 19683880.
- Kimura, M., Kuroshima, N., and Matsushita, T. “Flexor Pulley Reconstruction after Rupture Following Corticosteroid Injections for Trigger Thumb: A Case Report.” Hand Surgery: An International Journal Devoted to Hand and Upper Limb Surgery and Related Research, vol. 18, no. 2, 2013, pp. 259–262, PMID: 24156592.
- Nanno, M., Sawaizumi, T., Kodera, N., Tomori, Y., and Takai, S. “Flexor Pollicis Longus Rupture in a Trigger Thumb after Intrasheath Triamcinolone Injections: A Case Report with Literature Review.” Journal of Nippon Medical School = Nippon Ika Daigaku Zasshi, vol. 81, no. 4, 2014, pp. 272–276, PMID: 25186581.
- Tanaka, T., Ogawa, T., Yanai, T., Okano, E., Kohyama, S., and Ochiai, N. “Disruption of Flexor Tendon after Intrasheath Triamcinolone Acetonide Injection for Trigger Digits: Two Case Reports.” The Journal of Hand Surgery Asian-Pacific Volume, vol. 22, no. 3, Sept. 2017, pp. 415–418, PMID: 28774233.
- Yamada, K., Masuko, T., and Iwasaki, N. “Rupture of the Flexor Digitorum Profundus Tendon after Injections of Insoluble Steroid for a Trigger Finger.” The Journal of Hand Surgery, European Volume, vol. 36, no. 1, Jan. 2011, pp. 74–76, PMID: 21169306.
- Haddad R, Scherman P, Peltz T, Nicklin S, Walsh WR. A biomechanical assessment of repair versus nonrepair of sheep flexor tendons lacerated to 75 percent. J Hand Surg Am. 2010 Apr;35(4):546-51. doi: 10.1016/j.jhsa.2009.12.039. Epub 2010 Mar 2. PMID: 20189731.
- Bishop AT, Cooney WP 3rd, Wood MB. Treatment of partial flexor tendon lacerations: the effect of tenorrhaphy and early protected mobilization. J Trauma. 1986 Apr;26(4):301-12. doi: 10.1097/00005373-198604000-00001. PMID: 3959135.
