
Brian Q. Truong, DO, MS1; Kendyl E. Fahmy, OMSIV, MS2; Micah W. I. Jones, DO3
1Aultman Hospital, Canton, Ohio
2Edward Via College of Osteopathic Medicine, Blacksburg, Virginia
3LewisGale Medical Center, Salem, Virginia
DOI: http://doi.org/10.70709/of6zu0vz
Abstract
Lateral epicondylitis, also known as tennis elbow, is a prevalent overuse injury resulting from repetitive wrist extension and extensor carpi radialis brevis overload. Approximately 90% of cases resolve within 12 to 18 months with conservative management, which may include corticosteroid injections, platelet-rich plasma (PRP) injections, ultrasound-guided percutaneous needle tenotomy (PNT), bracing, physical therapy, occupational therapy, and nonsteroidal anti-inflammatory medications. Despite the variety of available nonoperative modalities, there is currently no universally effective standard for the conservative management of lateral epicondylitis. This article comprehensively reviews existing literature on nonoperative treatments and outlines our proposed approach, which seeks to optimize potential benefits while minimizing iatrogenic risks.
Keywords: Lateral Epicondylitis, Nonoperative Management
Introduction
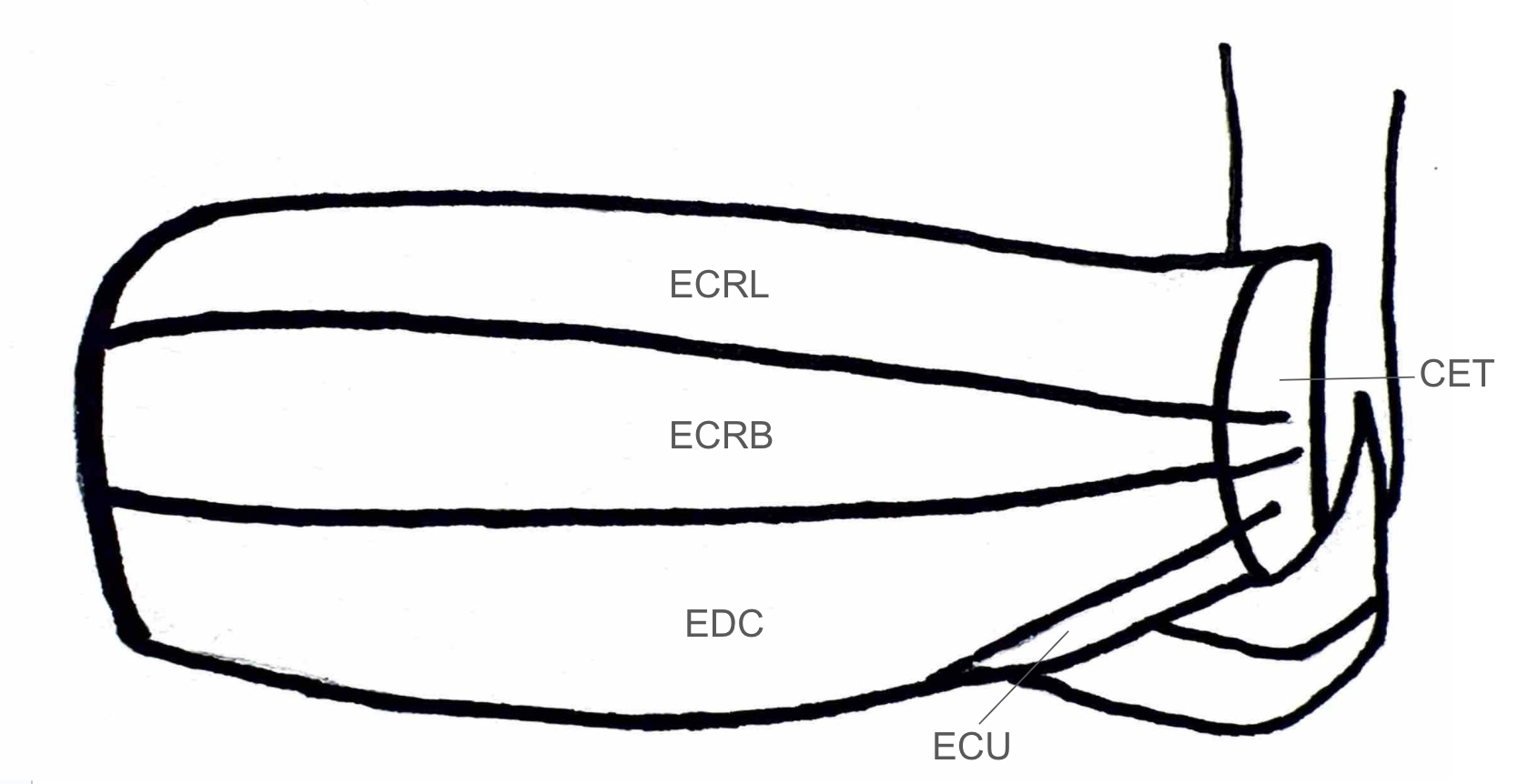
Lateral epicondylitis, colloquially known as tennis elbow, affects 1-3% of individuals annually, predominantly in those between 35 and 50 years of age (3,5). This disease is associated with overuse of the extensors of the wrist and hand, in particular the extensor carpi radialis brevis (ECRB), which originates on the lateral epicondyle of the humerus (Figure 1). Repetitive wrist extension and mechanical overload lead to microtears near the tendinous insertion of the ECRB on the lateral epicondyle. Risk factors include repetitive wrist extension and gripping, particularly in professions requiring manual labor, frequent tool use, and repetitive arm movements. Additional risk factors include obesity, smoking, and diabetes (5,6).
While most cases naturally resolve with watchful waiting, some patients may opt for a more active role in treatment (13). The average pathological course of lateral epicondylitis ranges from 1 to 1.5 years (5). Conservative management includes corticosteroid injections, platelet-rich plasma (PRP) injections, bracing, physical therapy, occupational therapy, and nonsteroidal anti-inflammatory medications (4,5). However, 10% of individuals continue to experience symptoms despite these interventions (7). Studies indicate that the median duration of lateral epicondylitis in this population is approximately 2.3 years. When conservative measures fail, operative treatment may include debridement and repair of the ECRB tendon (7).
Despite various proposed strategies, a definitive standard for the non-operative management of lateral epicondylitis has yet to be agreed upon. Guidelines have been developed by a host of organizations including the American College of Occupational and Environmental Medicine, the Canadian Shoulder and Elbow Society, and the Japanese Orthopaedic Association, though these recommendations vary greatly (14). In this article, we present our approach which attempts to optimize potential benefits while minimizing iatrogenic risks.
Treatment Modalities
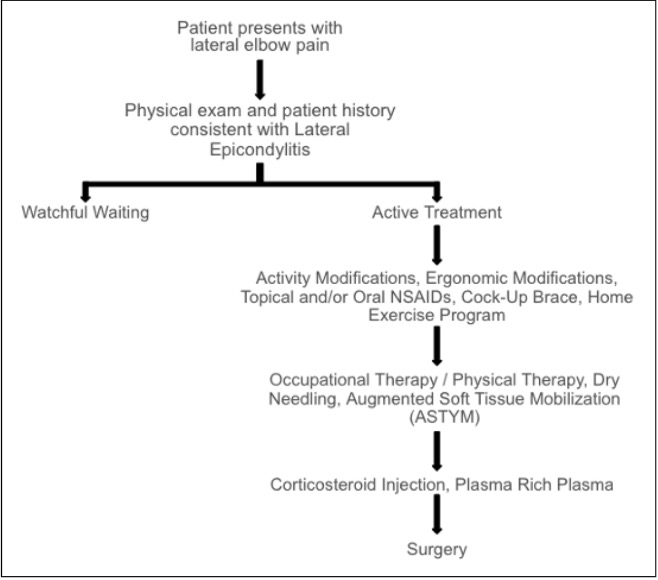
Various treatment modalities have been proposed for lateral epicondylitis. The primary treatment objectives include pain management, preservation of elbow mobility, enhancement of grip strength, restoration of normal function, and prevention of further damage of the ECRB (8). Lateral epicondylitis has been seen to resolve with non-operative treatment in 90% of cases. First-line treatment modalities commonly consist of activity modification, NSAIDs, bracing, physical or occupational therapy, and a home exercise program (Figure 2) (4,5,8).
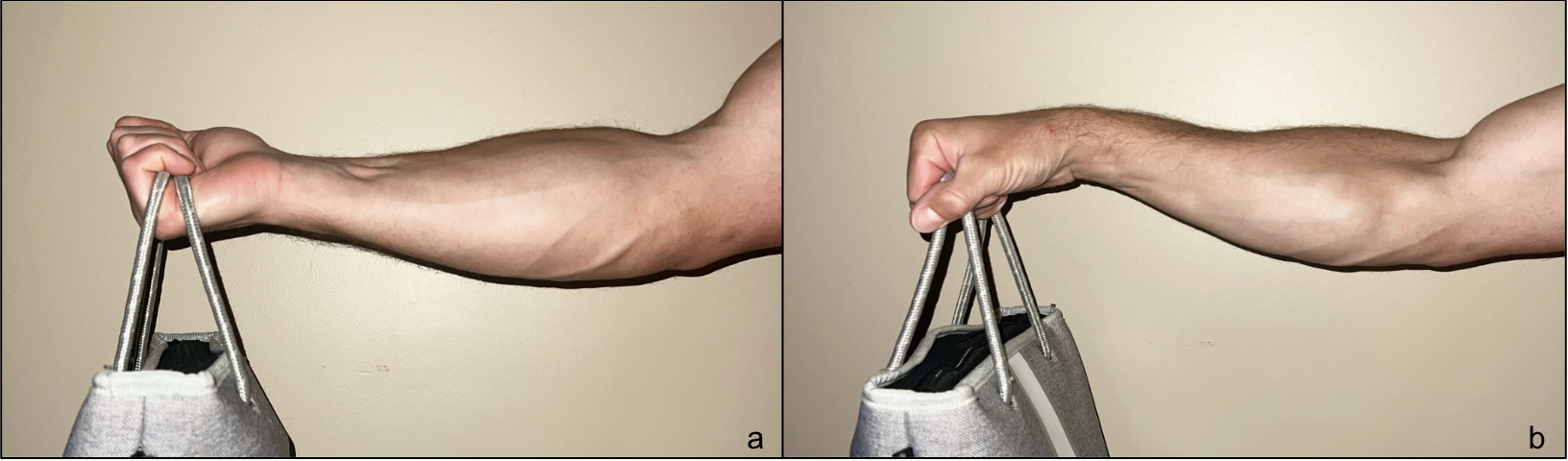
Within ergonomic modifications, we further subdivide into non-device based and device-based options. A study by Ikeda et al. demonstrated that activation of the ECRB during wrist extension in forearm pronation generates increased traction forces at its tendinous origin. This was established through measurements of muscle strength and electromyographic activity (28). The resulting biomechanical loading pattern helps explain the ECRB’s predisposition to developing lateral epicondylitis in the pronated position, as both contact pressure and muscle strain on the ECRB are maximized when the forearm is pronated (15,16,28). In contrast, lifting with the forearms supinated utilizes the flexors to offset the force exerted through the ECRB. An example of these lifting techniques can be seen in Figure 3. Forearm supination during activity is recommended due to its favorable safety profile and potential to reduce strain on the ECRB.
With this condition often affecting office workers, utilizing a vertical mouse positions the hand in a lateral position to avoid prolonged wrist extension and reduce overuse of the ECRB. A study from Quemelo and Vieira demonstrated that use of a vertical mouse was associated with decreased pronation (28° versus 42°), increased ulnar deviation (5° ulnar versus 7° radial), and decreases utilization of the extensor carpi (13% versus 16%) and extensor digitorum (10% versus 13%) muscles. Additionally, elevating oneself further superior to the keyboard will naturally encourage typing with the wrists in a flexed position (1). Due to the potential benefits and their relatively low overall risk, we routinely recommend these interventions when occupationally relevant.
Occupational therapy plays a supporting role in managing lateral epicondylitis, as it has minimal adverse effects and improves pain and function (4,8). Eccentric exercises, which lengthen the extensor tendons, have been found to have superior efficacy compared to other therapy modalities (8). Gradually increasing exercise duration and intensity helps promote tendon healing, so program protocol adherence is important to ensure effectiveness and restore function (4,8). Additionally, learning proper technique for our recommended ergonomic interventions may be of use. We recommend occupational therapy to all patients.
Dry needling involves the insertion of needles into or near myofascial trigger points to enhance blood flow and promote the release of endogenous opioids or neurotransmitters such as serotonin and norepinephrine (11). In lateral epicondylitis, these needles are inserted at the lateral epicondyle and along the ECRB and supinator tendons (17). While multiple sessions are often required to achieve therapeutic benefits, there is no standardized protocol regarding the interval or duration of these sessions, nor is there agreement on the optimal needle size or precise insertion points. A study by Uygur et al. demonstrated the efficacy of dry needling as a treatment modality for lateral epicondylitis, with significant improvement in symptoms observed at the six-month follow-up (2). A potential risk of this intervention is damage to the radial nerve. Cadaveric studies have demonstrated an anatomical relationship when a tendinous arch of the ECRB is present. However, the relative distance of the radial nerve branches from the supinator suggests a lower overall risk (17,18). While the precise risk of nerve injury from dry needling for lateral epicondylitis has not been clearly established, only 0.7% of dry needling practitioners report encountering a nerve injury over the course of their careers. (19). We consider the potential benefit to outweigh the limited risk.
Augmented Soft Tissue Mobilization (ASTYM) therapy utilizes cellular mediators and growth factors to promote scar tissue resorption and soft tissue regeneration. During treatment, a handheld instrument is applied to the skin with controlled pressure, generating shear forces that stimulate reparative cellular responses and facilitate tissue remodeling (10). In contrast, Instrument-Assisted Soft Tissue Mobilization (IASTM) employs tooled cross-friction massage to disrupt and remodel soft tissue adhesions (27). In a randomized controlled trial, Sevier et al. found that an ASTYM-only group achieved a 78.3% resolution of symptoms after four weeks of treatment, compared to 40.9% in an eccentric exercise-only group (10). With the potential added benefit of ASTYM in the recovery process, we aim to incorporate ASTYM in occupational therapy when possible.
Counterforce braces are frequently recommended for the management of lateral epicondylitis. These braces help alleviate pain by redistributing mechanical stress away from the origin of the ECRB, thereby reducing overuse and facilitating tissue healing. Examples of these braces can be seen in Figure 4. Proper placement is essential, with the brace positioned 5 cm distal to the lateral epicondyle over the extensor muscle belly (8, 12). Placement too proximally can result in posterior interosseous nerve (PIN) compression at the Arcade of Frohse, potentially causing motor deficits. There is often difficulty distinguishing between radial tunnel syndrome and lateral epicondylitis. If a patient is incorrectly diagnosed, the counterforce brace may potentially exacerbate radial tunnel syndrome. However, the incidence of iatrogenic radial tunnel syndrome or exacerbation of a preexisting syndrome is not well described in the literature (20). While there is some evidence to suggest benefit with counterforce bracing, our experience with patient frustration with treatment-resistant lateral epicondylitis has led us to avoid counterforce bracing to prevent potential worsening of symptoms (21).
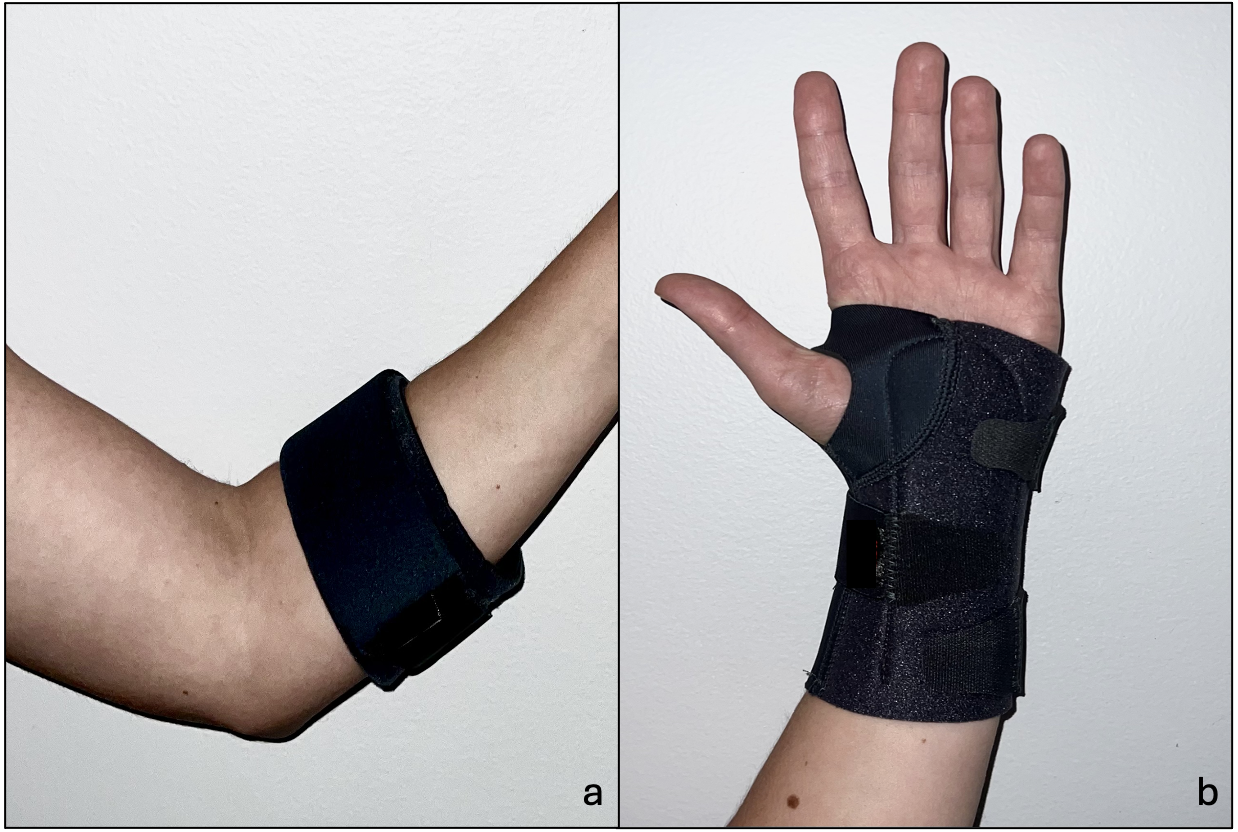
Cock-up wrist braces are less commonly utilized in lateral epicondylitis treatment. By holding the wrist in a neutral position, these braces help alleviate tension on the extensor muscles and tendons and decrease overall mechanical load. (8). Examples of these braces can be seen in Figure 4. Wrist braces have been shown to give short-term pain relief (22). Like counterforce braces, ill-fitting wrist braces can cause nerve compression, potentially affecting the median nerve at the carpal tunnel, the ulnar nerve at Guyon’s canal, or the superficial radial nerve. However, with good evidence to support wrist braces in the conservative management of carpal tunnel syndrome, we consider the risk of nerve compression to be of limited clinical significance (23). We recommend cock-up wrist braces, especially when occupationally relevant.
If first-line interventions fail to provide significant relief, second-line treatments may include ultrasound-guided percutaneous needle tenotomy (PNT), corticosteroid injections or PRP therapy. PNT is a minimally invasive procedure that involves targeted needle fenestration of abnormal tissue under ultrasound guidance. The technique facilitates the removal of degenerative tendon fibers while stimulating the release of local angiogenic mediators, promoting increased vascular permeability and a controlled inflammatory response. Several studies have demonstrated that PNT promotes neovascularization and collagen remodeling within the tendon (29). A systematic review by Maag et al. concluded that PNT is both an effective and low-risk intervention (30). Given its favorable safety profile and evidence of improved patient-reported pain outcomes, we recommend PNT be considered prior to surgical management.
Corticosteroid injections are historically included in treatment protocols, offering short-term relief by reducing inflammation. However, these injections do not target the underlying microtears at the tendon insertion of the ECRB on the lateral epicondyle (2). Corticosteroid injections can result in skin atrophy, hypopigmentation, tendon weakening, and impaired collagen synthesis. This can increase the risk of the ECRB tendon rupture and contribute to long-term tendon degradation (2,9). Evidence suggests that the efficacy of corticosteroid injections is limited, with studies reporting short-term relief but equivocal outcomes at the six-month follow-up (9,24). In our experience, however, these adverse events are of limited clinical significance. A patient refractory to this and all preceding treatment for a prolonged period would be a candidate for tendon debridement and repair. Removal of pathologic tissue would likely include a significant portion of steroid-degraded tendon as well. As an attempt to avoid operative treatment, we offer steroid injections if the previous conservative measures have failed.
PRP is an autologous, biologically derived product that can be exogenously applied to the origin of the ECRB. PRP contains a high concentration of platelet-derived growth factors, which are thought to promote tendon healing by stimulating tissue regeneration and repair (8,9). PRP preparations exhibit considerable variability in platelet and growth factor concentrations. Factors influencing PRP composition include the volume of whole blood collected, the method of platelet recovery, and the final volume of plasma. Currently, there is no standardized guideline regarding leukocyte content in PRP preparation, as the role of leukocytes in enhancing therapeutic efficacy remains incompletely understood. However, multiple studies have demonstrated that leukocyte-rich PRP preparations may positively influence the healing of soft tissue injuries (26). Animal models have demonstrated that PRP can induce tendon remodeling and enhance tendinosis repair (3). Peerbooms et al. reported a mean improvement of 63.9% in patients with lateral epicondylitis after one year of PRP treatment, in contrast to a 24% improvement observed following corticosteroid injections. Although repeat PRP injections may offer additional benefits in cases where the initial treatment yields suboptimal results, there is currently a lack of definitive studies to support this hypothesis (3). While clinical trends have recently favored PRP in the management of lateral epicondylitis, concerns have been raised over the statistical fragility of the supporting evidence. Furthermore, in our experience, patients often rely on self-pay in order to cover PRP. While we do offer PRP as an option, we do so after an extended discussion regarding the efficacy of treatment.
Conclusion
The treatment resistant nature of lateral epicondylitis predisposes management to involve a multimodal approach. Initial interventions should focus on activity and ergonomic modifications, wrist bracing, and occupational therapy with adjuncts including dry needling and ASTYM. With evidence trends for corticosteroid and PRP injections changing over the years, we continue to offer both with guarded usage. In the face of a dearth of high-quality literature, we seek to adapt current evidence-based treatment with our clinical experience.
References
- Quemelo PR, Vieira ER. Biomechanics and performance when using a standard and a vertical computer mouse. Ergonomics. 2013;56(8):1336-1344. doi:10.1080/00140139.2013.805251.
- Uygur E, Aktaş B, Yilmazoglu EG. The use of dry needling vs. corticosteroid injection to treat lateral epicondylitis: a prospective, randomized, controlled study. J Shoulder Elbow Surg. 2021;30(1):134-139.
- Peerbooms JC, Sluimer J, Bruijn DJ, Gosens T. Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial: platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. Am J Sports Med. 2010;38(2):255-262. doi:10.1177/0363546509355445.
- Cullinane FL, Boocock MG, Trevelyan FC. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clin Rehabil. 2014;28(1):3-19.
- Parikh HB, Stanley M, Tseng CC, Kulber DA, Kuschner SH. Lateral epicondylitis: treatment preferences from the potential patient perspective. Plast Reconstr Surg Glob Open. 2024;12(4):e5706. doi:10.1097/GOX.0000000000005706.
- Sayampanathan AA, Basha M, Mitra AK. Risk factors of lateral epicondylitis: A meta-analysis. Surgeon. 2020;18(2):122-128.
- Kholinne E, Singjie LC, Anastasia M, et al. Comparison of clinical outcomes after different surgical approaches for lateral epicondylitis: a systematic review and meta-analysis. Orthop J Sports Med. 2024;12(5). doi:10.1177/23259671241230291.
- Ma KL, Wang HQ. Management of lateral epicondylitis: a narrative literature review. Pain Res Manag. 2020;2020:6965381. doi:10.1155/2020/6965381.
- Barnett J, Bernacki MN, Kainer JL, Smith HN, Zaharoff AM, Subramanian SK. The effects of regenerative injection therapy compared to corticosteroids for the treatment of lateral epicondylitis: a systematic review and meta-analysis. Arch Physiother. 2019;9:1-12.
- Chughtai M, Newman JM, Sultan AA, et al. Astym® therapy: a systematic review. Ann Transl Med. 2019;7(4):70. doi:10.21037/atm.2018.11.49.
- Cagnie, B., Dewitte, V., Barbe, T., Timmermans, F., Delrue, N., & Meeus, M. (2013). Physiologic effects of dry needling. Current Pain and Headache Reports, 17(8), 348. https://doi.org/10.1007/s11916-013-0348-5
- Kroslak, M., Pirapakaran, K., & Murrell, G. A. (2019). Counterforce bracing of lateral epicondylitis: a prospective, randomized, double-blinded, placebo-controlled clinical trial. Journal of Shoulder and Elbow Surgery, 28(2), 288-295.
- Sayegh, E. T., & Strauch, R. J. (2015). Does nonsurgical treatment improve longitudinal outcomes of lateral epicondylitis over no treatment? A meta-analysis. Clinical Orthopaedics and Related Research, 473(3), 1093-1107. https://doi.org/10.1007/s11999-014-4022-y
- Hegmann, K. T., Hoffman, H. E., Belcourt, R. M., Byrne, K., Glass, L., Melhorn, J. M., Richman, J., Zinni, P. III, Thiese, M. S., Ott, U., Tokita, K., Passey, D. G., Effiong, A. C., Robbins, R. B., Ording, J. A. (2013). ACOEM practice guidelines: Elbow disorders. Journal of Occupational and Environmental Medicine, 55(11), 1365-1374. https://doi.org/10.1097/JOM.0b013e3182a0d7ec
- Takasaki, H., Aoki, M., Muraki, T., Uchiyama, E., Murakami, G., & Yamashita, T. (2007). Muscle strain on the radial wrist extensors during motion-simulating stretching exercises for lateral epicondylitis: a cadaveric study. Journal of Shoulder and Elbow Surgery, 16(6), 854–858. https://doi.org/10.1016/j.jse.2007.03.022
- Tanaka, Y., Aoki, M., Izumi, T., Wada, T., Fujimiya, M., & Yamashita, T. (2011). Effect of elbow and forearm position on contact pressure between the extensor origin and the lateral side of the capitellum. The Journal of Hand Surgery, 36(1), 81–88. https://doi.org/10.1016/j.jhsa.2010.10.005
- Fernández-de-Las-Peñas, C., López-de-Celis, C., Rodríguez-Sanz, J., Hidalgo-García, C., Donnelly, J. M., Cedeño-Bermúdez, S. A., & Pérez-Bellmunt, A. (2021). Is dry needling of the supinator a safe procedure? A potential treatment for lateral epicondylalgia or radial tunnel syndrome. A cadaveric study. International Journal of Environmental Research and Public Health, 18(17), 9162. https://doi.org/10.3390/ijerph18179162
- Vergara-Amador, E., & Ramírez, A. (2015). Anatomic study of the extensor carpi radialis brevis in its relation with the motor branch of the radial nerve. Orthopaedics & Traumatology: Surgery & Research, 101(8), 909–912. https://doi.org/10.1016/j.otsr.2015.09.030
- Gattie, E., Cleland, J. A., & Snodgrass, S. (2020). A survey of American physical therapists’ current practice of dry needling: Practice patterns and adverse events. Musculoskeletal Science & Practice, 50, 102255. https://doi.org/10.1016/j.msksp.2020.102255
- MacDermid, J. C., & Walton, D. M. (2011). Nerve compression syndromes of the forearm. In Neck and Arm Pain Syndromes E-Book (p. 370).
- Kroslak M, Pirapakaran K, Murrell GAC. Counterforce bracing of lateral epicondylitis: a prospective, randomized, double-blinded, placebo-controlled clinical trial. J Shoulder Elbow Surg. 2019;28(2):288-295. doi:10.1016/j.jse.2018.10.002
- Songur K, Demir ZD, Baysan C, Dilek B. Clinical and ultrasonographic effectiveness of two different splints used for the treatment of lateral epicondylitis: a prospective randomized controlled study. Arch Phys Med Rehabil. 2024;105(4):655-663. doi:10.1016/j.apmr.2023.12.010
- Figueiredo DS, Ariboni RR, Tucci HT, Carvalho RP. Effects of wrist orthoses in reducing pain in individuals with carpal tunnel syndrome: a systematic review. Disabil Rehabil. 2024;46(23):5395-5403. doi:10.1080/09638288.2023.2301019
- Smidt N, Assendelft WJ, van der Windt DA, Hay EM, Buchbinder R, Bouter LM. Corticosteroid injections for lateral epicondylitis: a systematic review. Pain. 2002;96(1-2):23-40. doi:10.1016/s0304-3959(01)00388-8
- Messer CJ, Oeding JF, Barlow JD, Sanchez-Sotelo J, Krych AJ, Camp CL. The statistical fragility of platelet-rich plasma in lateral epicondylitis: a systematic review and simulated fragility analysis of randomized controlled trials. Arthroscopy. 2023;39(6):1230–1238. doi:10.1016/j.arthro.2023.01.030
- Arnoczky, S. P., Delos, D., & Rodeo, S. A. (2011). What Is Platelet-Rich Plasma? Operative Techniques in Sports Medicine, 19(3), 142 148. https://doi.org/10.1053/j.otsm.2010.12.001
- Chughtai, M., Newman, J. M., Sultan, A. A., Samuel, L. T., Rabin, J., Khlopas, A., & Mont, M. A. (2019). Astym® therapy: A systematic review. Annals of Translational Medicine, 7(4), 70. https://doi.org/10.21037/atm.2019.01.27
- Keda K, Kaneoka K, Matsunaga N, Nagano A, Fujimoto K, Shiraki H. Effects of forearm rotation on wrist flexor and extensor muscle activities. J Orthop Surg Res. 2025;20:53. doi:10.1186/s13018-024-05363-x
- Dakkak M, Patel V, King D, Genin J. Ultrasound-guided tenotomy for lateral epicondylitis with TenJet improves physical functional and decreased pain outcomes at 1 year: a case series review. JSES Int. 2023;7(5):872-876. Published 2023 May 27. doi:10.1016/j.jseint.2023.05.003
- Maag L, Linder S, Hackett L, et al. Effectiveness of Percutaneous Needle Tenotomy for Tendinopathies: A Systematic Review. Sports Health. 2025;17(4):834-842. doi:10.1177/19417381241275659
