
Isabella M. Cashin, DO1; Kendyl E. Fahmy, OMSIV, MS2; Micah W. I. Jones, DO3
1Wellspan Health, York, Pennsylvania
2Edward Via College of Osteopathic Medicine, Blacksburg, Virginia
3LewisGale Medical Center, Salem, Virginia
DOI: http://doi.org/10.70709/j1x28yt29
Abstract
Osteomyelitis is an acute or chronic bone infection that may arise from hematogenous spread or direct inoculation. Prosthetics, ischemia, and trauma increase susceptibility by introducing foreign material or compromising the blood supply. Staphylococcus aureus is the most common causative organism, whereas Neisseria gonorrhoeae is rarely reported. We describe a case of osteomyelitis of the proximal phalanx of the left middle finger, with associated synovitis of the dorsal and palmar tendon sheaths, caused by N. gonorrhoeae.
A patient presented three weeks post-injury with worsening pain, swelling, and limited motion of the finger. Imaging revealed bone lucency and chondral fragmentation, and MRI findings were consistent with osteomyelitis. The patient underwent incision, debridement, and synovectomy. Cultures confirmed N. gonorrhoeae. After completing intravenous antibiotics, the patient was lost to follow-up. This case highlights the importance of bone culture and biopsy for definitive diagnosis and targeted treatment, especially in rare infections such as N. gonorrhoeae.
Keywords: Tenosynovitis, Osteomyelitis, Neisseria gonorrhea
Introduction
In the United States, Neisseria gonorrhoeae is the second most common sexually transmitted infection. In 2022, there were a total of 648,056 cases reported, representing a 9.2% decrease compared with 20213. The true incidence is likely underestimated as N. gonorrhoeae infections can be asymptomatic. The decline in reported cases may reflect either a genuine reduction in transmission or decreased screening rates2-3.
Disseminated Neisseria gonorrhea (DGI) commonly occurs due to sexual transmission. The bacterium invades the bloodstream, which can be seen as septic arthritis in young adult populations, polyarthralgia, bacteremia, and rarely endocarditis2. These presentations can occur in the absence of genitourinary symptoms. DGI is reported to only occur in 0.5%-3% of individuals with gonorrhea, mostly commonly presenting as septic arthritis4. A rare complication of DGI with prolonged septic arthritis is osteomyelitis. Few reports exist of DGI osteomyelitis. The most common anatomy involved is larger joints such as the shoulder, knee, and spine4-5. Although limited literature exists on the treatment of DGI, the most used antibiotic regimen consisted of multiple weeks of intravenous therapy followed by subsequent oral therapy 4-5.
In this case report, we present a case of disseminated gonococcal infection in a middle-aged male with involvement of the proximal interphalangeal joint, extensor and palmar tendons. The course was complicated by delayed presentation and necessitated prolonged antibiotic therapy. We additionally review previously reported cases of DGI associated with osteomyelitis.
Report of Case
A right-hand dominant male with a non-contributory past medical history presented with a chief complaint of middle finger pain and swelling in the left hand. The pain was localized to the left middle finger and was exacerbated by movement or pressure and alleviated by rest. The pain was rated as 8/10 in severity. The patient denied numbness, tingling, fever, chills, or drainage from the finger. There was no history of diabetes mellitus, autoimmune disease, or gout.
The patient reported an injury to the left middle finger three weeks prior to presentation, which resulted in a contusion and immediate discomfort. Following the accident, the patient presented to the emergency department (ED) where radiographs were obtained. The images did not show a fracture. No skin laceration was reported, and antibiotics were not started. After ED presentation, the patient experienced increased swelling, pain, and loss of motion. The patient denied drainage or erythema but reported a fluid-filled blister that formed and ruptured.
Examination of the left hand revealed intact skin with delamination over the PIP joint of the left middle finger. Full finger extension was limited and elicited pain along the middle and proximal phalanx. Both the DIP and PIP joints had a decrease in range of motion. There was no tenderness along the tendon sheath at the distal phalanx, DIP joint, or proximal to the A1 pulley. Swelling was present along the radial and ulnar sides of the PIP joint. Pain was located palmary and dorsally at the PIP joint. There was mild warmth to the finger. No tracking erythema, collateral instability, or pain in the remainder of the hand and wrist was noted. Neurovascular structures in the surrounding areas were intact. All other physical examination findings were within normal limits.
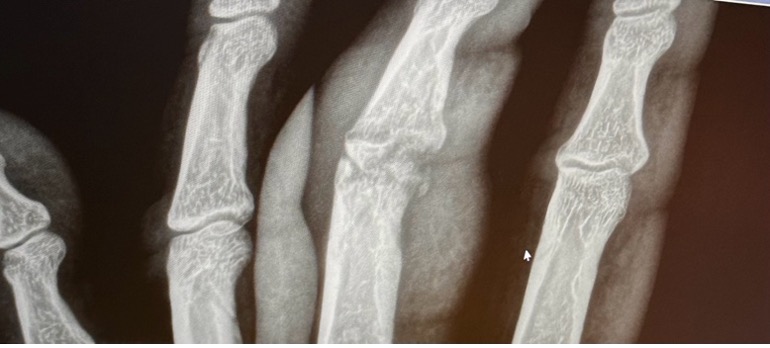
New radiographs were obtained. Images showed significant changes from initial films, including resorption of bone with the fragmentation of the subchondral surface of the proximal to the PIP joint (Figures 1-4). Due to concerns regarding osteomyelitis or avascular necrosis, an MRI with contrast of the left middle finger was acquired. Laboratory work was completed, including CRP, ESR, CBC with differential, and CMP, and oral Trimethoprim-Sulfamethoxazole 800mg was initiated. Ketorolac tromethamine 10mg was provided for pain.



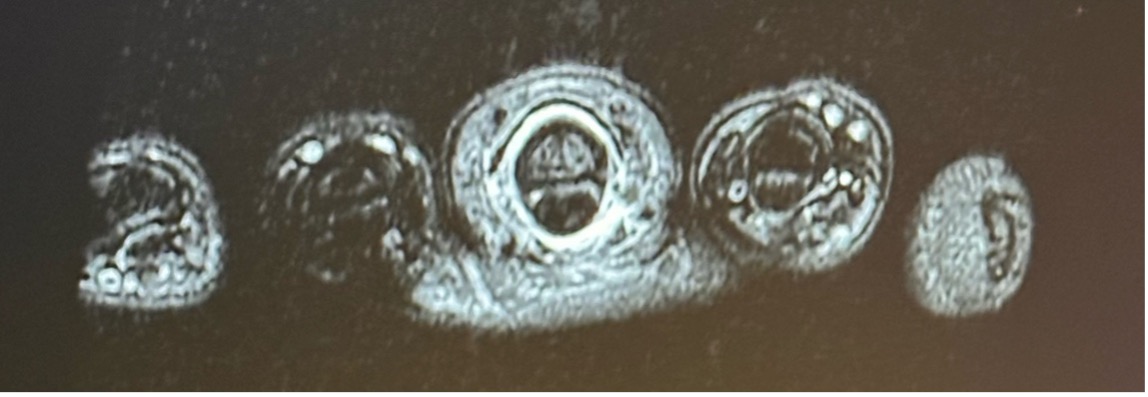
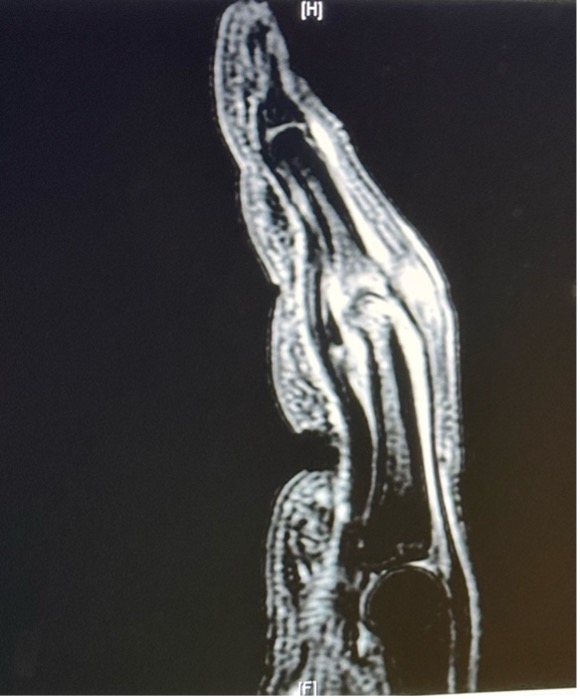
During follow-up, MRI images were reviewed. The images were consistent with osteomyelitis of the proximal phalanx with synovitis, injury to the collateral ligaments and capsule, and infection of the PIP joint (Figures 5-7). Laboratory values were within normal limits, and the patient remained afebrile. The risks and benefits of conservative management versus surgical intervention were discussed. Incision and drainage of the left middle finger with synovectomy, open bone biopsy, and arthrotomy of the PIP joint were recommended. The patient expressed understanding and elected to proceed with surgical intervention.

During the procedure, intraoperative vancomycin was administered, and antibiotic powder was placed prior to closure. Bone biopsy and soft tissue specimens, including aerobic and anaerobic cultures, were sent for microbiology analysis. Bone specimens were additionally sent to pathology.
Postoperatively, the patient was placed on Trimethoprim-Sulfamethoxazole and Amoxicillin-clavulanic acid as instructed by Infectious Disease (ID) with plans to follow up for potential PICC line placement. Following the ID consult, a PICC line was placed with daptomycin 750mg IV q24 hours initiated and ertapenem 1g IV daily for six weeks. Trimethoprim-sulfamethoxazole was also discontinued.
Cultures of the bone resulted in infection by S. epidermidis and N. gonorrhea with resistance to penicillin. Amoxicillin-clavulanic acid was discontinued, and clindamycin was initiated in addition to IV therapy already discussed. The patient was called and asked if he was experiencing any genitourinary symptoms or if he or his partner had any STI symptoms. The patient denied having any symptoms and stated that their partner was not either. Both the patient and partner denied extramarital relations.
During the postoperative appointment, sutures were removed, and additional radiographs demonstrated periosteal reaction but no evidence of fusion (Figures 8-10). A splint was provided and the patient was recommended to follow up in four weeks. The patient did not follow up. Medical records were received regarding a follow-up appointment with ID, noting no signs of infection, and intact, clean, dry, and healed incisions. The PICC line was discontinued, and antibiotics were completed. Decreased active range of motion was reported, with no measurements listed in the records.



Discussion
The presentation of swelling and pain with flexion in fingers should illicit concern for suppurative flexor tenosynovitis (FTS)6. Diagnosis of FTS can be made clinically with the use of four cardinal signs, known as Kanavel’s signs. The Kanavel criteria include tenderness over the tendon sheath, flexed finger posture, pain with passive extension, and fusiform swelling of the whole finger6. When any of the Kanavel signs are present, it indicates high sensitivity, but low specificity for FTS. Not all four signs are required for diagnosis. The earliest sign to present is pain with passive extension, with the last being tenderness to palpation over the tendon sheath6. When suspected, emergent open management is required6. In our case, FTS was of concern; however, the diagnosis was unclear. The history of prior injury and duration of symptomology lead to obtaining further imaging rather than emergent surgical intervention.
Neisseria gonorrhea is an infection that can disseminate, causing tenosynovitis, polyarthralgia, and osteomyelitis8. Gonococcal tenosynovitis has been found to infect the flexor tendon sheath8. In our clinical scenario, both the flexor and extensor compartments were affected. Typically, tenosynovitis is seen following trauma, as was present in our case7. Treatment of tenosynovitis begins with irrigation and debridement of each compartment and initiation of intravenous antibiotics. The diagnosis of DGI usually presents with genitourinary symptoms in addition to arthralgia and synovitis symptoms6. However, in our case, the patient denied genitourinary symptoms, therefore no urinalysis or cultures were done to confirm. Given the MRI results, operative management was warranted and bone biopsy confirmed osteomyelitis.
Classification of osteomyelitis remains difficult due to its varied etiologies, and existing systems are not widely accepted9. The Waldvogel classification depends on the persistence of acute or chronic infection and the source of infection10. This classification has shown improved disease cure rates and evidence of differences in clinical presentation10. The Cierny-Mader classification is based on the condition of the host, the functional impairment caused by the disease, the site of involvement, and the extent of bony necrosis10. This system allows for strategies for debridement, antibiotic management, and dead space management10.
Treatment of osteomyelitis lacks definitive guidelines and depends on the cultures from the area of infection10. The gold standard for diagnosis is bone biopsy with antibiotics tailored to the sensitivity and resistance of the microorganism involved10. In this case, antimicrobial therapy was modified in accordance with the results of bone and synovial fluid cultures. Although Neisseria gonorrhoeae is generally susceptible to beta-lactam and macrolide antibiotics, the isolated strain demonstrated resistance to penicillin. Accordingly, intravenous therapy was adjusted, highlighting the critical role of culture and sensitivity testing in optimizing antimicrobial selection and ensuring effective clinical management10.
Given the complex presentation of osteomyelitis and tenosynovitis secondary to Neisseria gonorrhoeae, clinicians should maintain a high index of suspicion for gonococcal infection as a potential differential diagnosis, even in the absence of classical genitourinary manifestations. With an estimated two million Americans affected, it is essential to obtain thorough sexual histories and consider urinary screening in young and middle-aged patients presenting with joint arthralgia and erythema.10.
Conclusions
In this case, a middle-aged male developed osteomyelitis of the proximal interphalangeal phalanx following direct trauma. The infectious organism was subsequently identified as Neisseria gonorrhoeae.. This presentation underscores the importance of considering gonococcal dissemination in similar clinical scenarios, as well as deliberate, comprehensive screenings and social histories in populations at most significant risk.
References
- Momodu, I. I., & Savaliya, V. (2023, May 31). Osteomyelitis. StatPearls – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK532250/
- Department of Public Health. Disseminated gonococcal infection. https://www.cdph.ca.gov/Programs/CID/DCDC/Pages/Disseminated-Gonococcal-Infection.aspx#:~:text=DGI%20occurs%20when%20the%20sexually,on%20rare%20occasions%2C%20endocarditis%20or
- National Overview of STIs, 2022. https://www.cdc.gov/std/statistics/2022/overview.htm#Gonorrhea
- Liakos W, Schaffler B, Rajan S, Hagmann SHF. Gonococcal osteomyelitis in a pediatric patient with disseminated gonococcal infection: Implications for antimicrobial management. IDCases. 2020;21:e00875. Published 2020 Jun 18. doi:10.1016/j.idcr.2020.e00875
- Roy M, Ahmad S, Roy AK. Rare presentation of vertebral discitis, osteomyelitis and polyarticular septic arthritis due to disseminated Neisseria gonorrhea infection. J Community Hosp Intern Med Perspect. 2020;10(1):55-59. Published 2020 Feb 10. doi:10.1080/20009666.2019.1710930
- Chan E, Robertson BF, Johnson SM. Kanavel signs of flexor sheath infection: a cautionary tale. Br J Gen Pract. 2019;69(683):315-316. doi:10.3399/bjgp19X704081
- Jain N, Saadat S, Goldberg M. Flexor Tenosynovitis Caused by Neisseria gonorrhea Infection: Case Series, Literature Review, and Treatment Recommendations. Arch Plast Surg. 2023;50(2):216-219. Published 2023 Feb 1. doi:10.1055/a-1938-0837
- Anwar S, Acharya S, Shahab A, Glaser A. Osteomyelitis and extensor tenosynovitis- an unusual presentation of Neisseria gonorrhoeae. IDCases. 2020;22:e00967. Published 2020 Sep 29. doi:10.1016/j.idcr.2020.e00967
- Jha Y, Chaudhary K. Diagnosis and Treatment Modalities for Osteomyelitis. Cureus. 2022;14(10):e30713. Published 2022 Oct 26. doi:10.7759/cureus.30713
- Kavanagh N, Ryan EJ, Widaa A, et al. Staphylococcal Osteomyelitis: Disease Progression, Treatment Challenges, and Future Directions. Clin Microbiol Rev. 2018;31(2):e00084-17. Published 2018 Feb 14. doi:10.1128/CMR.00084-17
