
Robert Garner, DO, HCA; Kyle Barner, DO; Andre Jakoi, MD
HCA – Midwest Division
DOI: http://doi.org/10.70709/m9bdrqw3j
ABSTRACT
Study Design
Case report.
Case
A 22-year-old helmeted male involved in a motorcycle versus automobile at highway speeds was ejected a long distance. He sustained multiple upper extremity fractures and was intubated in the emergency department. His upper extremity injuries were treated surgically within two weeks of the accident. The patient continued to have upper extremity weakness three months after the accident. A cervical spine MRI revealed a right C5 nerve root avulsion with pseudomeningocele formation. The patient was referred to a specialist for further evaluation and treatment.
Conclusion
The C5 nerve root avulsion with pseudomeningocele formation diagnosis was delayed likely due to contaminant bilateral upper extremity injures. Consideration of cervical nerve root avulsions should be considered in patients with asymmetric upper extremity neurological physical exams with a high-energy mechanism.
Keywords: Cervical spine, Cervical nerve root avulsion, Pseudomeningocele, Trauma, Spine surgery
INTRODUCTION
Traumatic cervical nerve root avulsions are rare injuries associated with high-speed motor vehicle accidents 1,2,3. The traction forces from the injury pull the nerve root sleeve into the intervertebral foramen with tearing of the meninges followed by proximal nerve root retraction and cerebrospinal fluid filling the neural foramen resulting in a pseudomeningocele 4. The true incidence of these injuries is difficult to quantify with an estimated prevalence of .36 – 6.3 cases per 100,000 people 1. We present a case with a C5 nerve root avulsion with pseudomeningocele following a highspeed motorcycle accident versus automobile with multiple contaminant injuries. Informed consent was obtained by the patient.
CASE PRESENTATION
A 22-year-old male patient presents to the emergency department (ED) as a level one trauma after being involved in a motorcycle versus automobile at highway speeds as a helmeted motorcyclistejected a long distance. His past medical history is non-contributory. He had a Glasgow Coma score of 7 with hypotension; he was intubated in the ED. He had obvious deformities to bilateral upper extremities. A thorough neuro exam was not able to be obtained due to being intubated and multiple orthopedic injuries. Pelvis radiograph revealed an APC III pelvis fracture. A pelvic binder was placed, and massive transfusion protocol was started with improvement in blood pressure. Bilateral upper extremities radiographs demonstrated right glenohumeral dislocation, right comminuted proximal ulna fracture, right comminuted radial head fracture, right radial carpal dislocation, left distal humerus metaphyseal fracture, and open left intraarticular distal radius and ulna fractures which were reduced and splinted appropriately. Cefazolin and TDaP were administrated per open fracture protocol. Further imaging showed a right pulmonary emboli in which an inferior vena cava filter was placed. The cervical computed topography (CT) scan was negative for fracture. The toxicology panel was negative for alcohol and positive for marijuana.
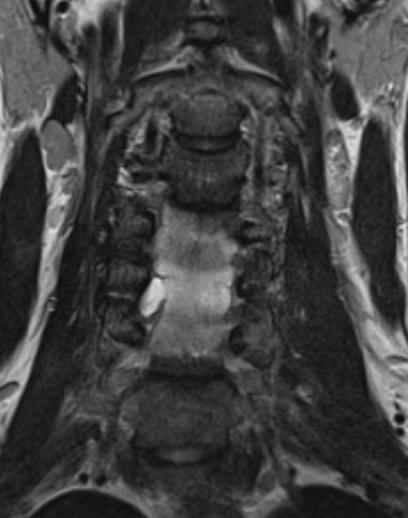
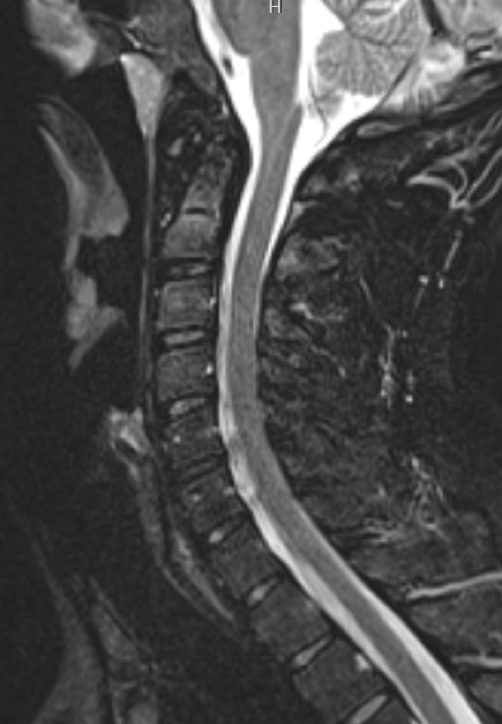
He underwent open reduction and internal fixation (ORIF) of the sacrum and pubic symphysis with percutaneous screws and 3.5mm plate and screws, irrigation and debridement with ORIF for the open left distal radius and ulna fractures with plate and screws the day after the accident. One week later, he underwent ORIF his remaining closed injuries – ORIF right proximal ulna with plate and screws, ORIF right olecranon with plate and screws, ORIF right distal radius with volar plate, bilateral radial head arthroplasty, left elbow internal joint stabilizer (IJS; Skeletal Dynamics, Miami, FL, USA), ORIF left coronoid with screw, left lateral ulnar collateral ligamnet reconstruction, . He was discharged two weeks later and followed up outpatient where he continued 0/5 motor to right deltoid with numbness over his deltoid 14 weeks from the date of injury. A cervical MRI found a pseudomeningocele right C5-C6 neural foramen causing mass effect on the exiting C6 nerve root with avulsion of the C5 nerve root as seen in figure 1 with caudal extension of the pseudomeningocele demonstrated in figure 2 and figure 3. He was referred to a specialist for further evaluation and treatment of C5 nerve root avulsion and did not follow up with the operative surgeon.

DISCUSSION
This case adds to the paucity of literature relating to cervical nerve root avulsions, specificality C5. Our patient presented as a polytrauma with multiple distracting bilateral upper extremity injuries and a Glasgow Coma score requiring intubation in the ED limiting the ability to obtain a thorough neurological exam. His C5 nerve root avulsion diagnosis was made 3 months after the accident due to continued weakness in the right upper extremity after surgical fixation of his fractures.
The incidence of cervical nerve root lesions is rare in both adults and pediatric patients following a trauma 1,4. The majority of patients sustaining these injuries were male, with a mean age of 28 years, most commonly associated with motorcycle accidents, and involving supraclavicular lesions.
Approximately one third of patients with these injuries had alcohol in their system at the time of the accident, did not have a driver’s license, and a third of patients had concurrent long bone fractures 1.
The diagnosis of cervical nerve root lesions can be difficult acutely given the association with concurrent injuries and negative CT scans. Newman recommends the consideration of brachial plexus injuries with asymmetric examinations, epidural hematomas, and appropriate traumatic mechanisms 4. The average time from injury to treatment of brachial plexus injures is about 4.7 months 2. A cervical spine MRI without contrast is recommended.
The treatment consists of conservative management with physical therapy and occupational therapy with bracing, versus operative management necessitating a surgical specialist for nerve transfer 2,3,5.. Bertelli states the neurological deficits from brachial plexus injuries are lifelong with significant socioeconomic effects 5.
CONCLUSION
Cervical nerve root avulsions with pseudomeningocele formations are rare traumatic injuries associated with high-speed motorcycle accidents with a delayed diagnosis due to distracting injures. The treatment consists of conservative management with physical therapy and occupational therapy with bracing or requires a specialist for nerve transfers. Consideration of these injuries should occur with asymmetric physical examinations, high speed mechanisms of injury, and obtaining a cervical spine MRI with continued upper extremity weakness after definitive fixation of contaminant injuries.
DATA AVAILABILITY
Data are available upon request to the corresponding author.
AUTHOR CONTRIBUTIONS
RG is the primary author, KB aided with editing, and AJ oversaw the project.
COMPETING INTERESTS
The contact author has declared that none of the authors listed have competing interests.
ETHICAL STATEMENT
Written informed consent for this case report was provided by the patient. IRB approval was obtained by our academic institution.
DISCLAIMER
None of the authors listed have any financial ties with any biotechnology companies. This case report was not incentivized by industry financial or material support. This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
REFERENCES
- Faglioni W Jr, Siqueira MG, Martins RS, Heise CO, Foroni L. The epidemiology of adult traumatic brachial plexus lesions in a large metropolis. Acta Neurochir (Wien). 2014;156(5):1025-1028. doi:10.1007/s00701-013-1948-x
- Irene Fasce, Pietro Fiaschi, Andrea Bianconi, Carlo Sacco, Guido Staffa & Crescenzo Capone (2023) Long-term functional recovery in C5-C6 avulsions treated with distal nerve transfers, Neurological Research, 45:9, 867-873, DOI: 10.1080/01616412.2021.1942410
- Haider A S, Watson I T, Sulhan S, et al. (February 14, 2017) Traumatic Cervical Nerve Root Avulsion with Pseudomeningocele Formation. Cureus 9(2): e1028. DOI 10.7759/cureus.1028
- Newman WC, Tempel ZJ, Tyler-Kabara EC. Posttraumatic Cervical Nerve Root Avulsion with Epidural Hematoma. World Neurosurg. 2015;84(4):. doi:10.1016/j.wneu.2015.06.050
- Bertelli JA, Ghizoni MF. Brachial plexus avulsion injury repairs with nerve transfers and nerve grafts directly implanted into the spinal cord yield partial recovery of shoulder and elbow movements. Neurosurgery. 2003;52(6):1385-1390. doi:10.1227/01.neu.0000065134.21334.d7
