Porter K, Jiganti M, Tedesco N
Samaritan Health Services, Corvallis, OR, USA
Introduction
Upper extremity amputations, while sometimes necessary for severe trauma or malignancy, are rare, life-altering operations that carry significant physical and psychological burdens. Pain management in such cases remains challenging, with limited evidence on the most effective perioperative analgesic strategies. This case study presents the perioperative pain regimen of a 56-year-old male who underwent forequarter amputation, alongside a discussion of current analgesic modalities for upper extremity amputations, including pharmacologic agents, peripheral nerve catheters, nerve blocks, peripheral nerve stimulation (PNS), targeted muscle reinnervation (TMR), regenerative peripheral nerve interface (RPNI), cryo-analgesia, and scrambler therapy (ST), to evaluate further a potential superior pain-control modality in the peri-operative window for upper extremity amputations.
Methods
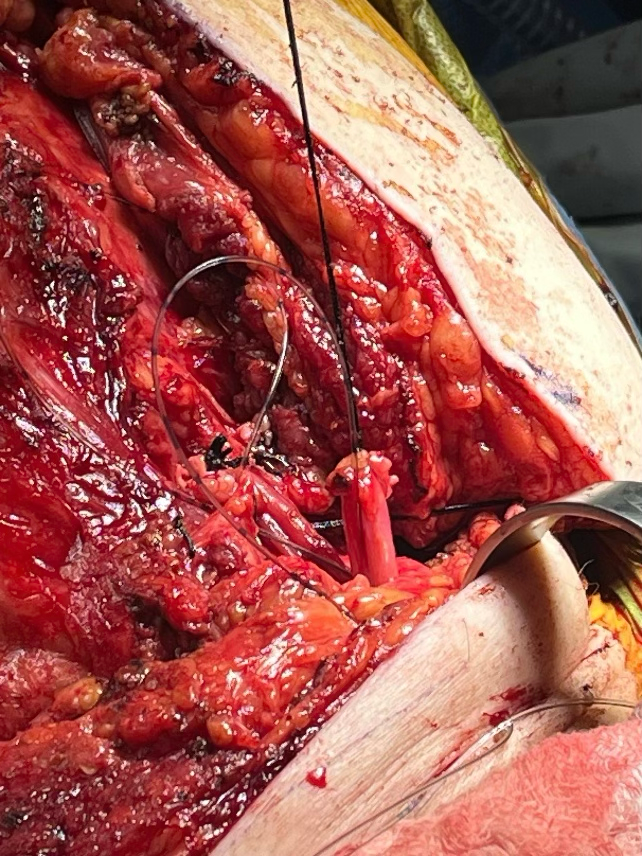
A 56-year-old male with PMH of schizophrenia, HTN, HLD, and T2DM presented with a high-grade undifferentiated pleomorphic sarcoma resistant to chemotherapy in the left proximal humerus. Before surgery, the patient reported severe pain despite daily MS Contin and rescue Oxycodone. Physical exam preoperatively was significant for a visible, 10-12 cm left shoulder mass with decreased shoulder range of motion. Because of extensive bone and neurovascular involvement, the decision was made to undergo forequarter amputation for life-saving efforts. He underwent amputation without complication, and his perioperative pain regimen included peripheral nerve catheters implanted into the severed brachial plexus cords intra-operatively and multi-modal pharmacotherapy.
Results
Postoperative pain was well-controlled with nerve catheters and pharmacotherapy. He was discharged on over-the-counter analgesics alone. At three months, he reported improved pain but noted mild phantom limb pain (PLP) and hypersensitivity. He was referred to physical medicine and rehabilitation and continues symptom management with just over-the-counter analgesics.
Discussion
Despite various techniques, no consensus exists on optimal perioperative pain control in upper extremity amputations. Given the high prevalence of persistent pain, catheter-based analgesia is recommended in the acute phase. A multidisciplinary approach remains essential, and further research is needed to identify superior strategies for acute and chronic pain management. This question is imperative to be addressed as approximately one-half of all amputees continue to experience some form of residual or phantom limb pain, leading to decreased functionality as well as continued physical and mental anguish for this population. More research is required to fully understand the intricacies of how our pain pathways are affected in upper extremity amputations and how to counteract them most adequately.