
Reagan Boyett, OMS III1; Morgan Wirth, OMS II2; Tyler Overbeek, OMS IV2; Nathan Douthit, MD2; Blake Boyett, DO3
1Edward Via College of Osteopathic Medicine – Auburn and The Orthopedic Center
2Edward Via College of Osteopathic Medicine – Auburn
3The Orthopedic Center
Abstract
Introduction
Guillain-Barré Syndrome (GBS) is an immune-mediated polyneuropathy that can be triggered by physiologic stress including infection, immunization, and in very rare cases, spinal surgery. The predominant symptoms of weakness and sensory impairment are easily attributed to mechanical complications following surgery. This report adds to the literature a case of GBS following transforaminal lumbar interbody fusion (TLIF) of L4/L5 and discusses presentation, diagnostic considerations, and appropriate post-operative management.
Case
A 49-year-old male was diagnosed with GBS following a (TLIF) of L4/L5. The patient presented to the emergency room for weakness in his legs and areflexia two weeks after his spinal surgery. Laboratory and imaging revealed no postoperative cause. Lumbar puncture revealed albuminocytologic dissociation, consistent with GBS. The patient was treated and regained complete sensation and reflexes by three months and recovery of most muscle strength by six months.
Conclusion
Guillain-Barré Syndrome is a rare complication of spinal surgery and can mimic intraoperative damage to the spinal cord. Early diagnosis and treatment are essential to avoid respiratory paralysis and rule out spinal cord injury. Because of its life-threatening complications, GBS should be considered on the differential diagnosis of lower extremity weakness after spinal surgery.
Keywords: Guillain-Barré Syndrome, postoperative complication, transforaminal lumbar interbody fusion, case report
Introduction
Guillain-Barré syndrome (GBS) is an acute immune-mediated polyradiculoneuropathy with a progressive, symmetrical weakness and sensory impairment, beginning in the lower limbs and extending proximally. It is the global leading cause of acute flaccid paralysis, with approximately 1–2 cases per 100,000 population per year. (1,2) The majority of the illnesses are triggered by an infection and vaccines that provoke an autoimmune response by molecular mimicry that targets peripheral nerve components, including myelin and axons. (1,3-5) Rarely, surgery can be the inciting event leading to the development of GBS, though the mechanism behind this is poorly understood. (6). There have been genetic correlations reported with GBS affiliated with immune genes, but many studies conflict. (7) Clinical manifestations involve progressive weakness of the limbs, areflexia, sensory impairment that varies and, in advanced cases, respiratory failure and autonomic dysfunction (8-9).
This case of GBS following transforaminal lumbar interbody fusion (TLIF) of L4/L5 provides a valuable contribution to existing literature as weakness and sensory impairment following spinal surgery should raise concern for postoperative complications. These traditionally include structural (fusion failure, migration of hardware), infectious, and hemorrhagic. Immunologic complications like GBS should be promptly evaluated and treated.
Case Description
A 49-year-old male presented to the emergency department for an evaluation of weakness in his legs to the point that he was unable to get out of bed. He had TLIF of the L4/L5 exactly two weeks prior to admission to the hospital. The patient stated that he had been recovering well up until a few days prior to admission. He had episodes of his legs giving out while using the bathroom and at times, was unable to leave the bed. Pertinent family history showed Guillain-Barré Syndrome in his father. His respirations were clear and nonlabored, and the patient was calm and cooperative.
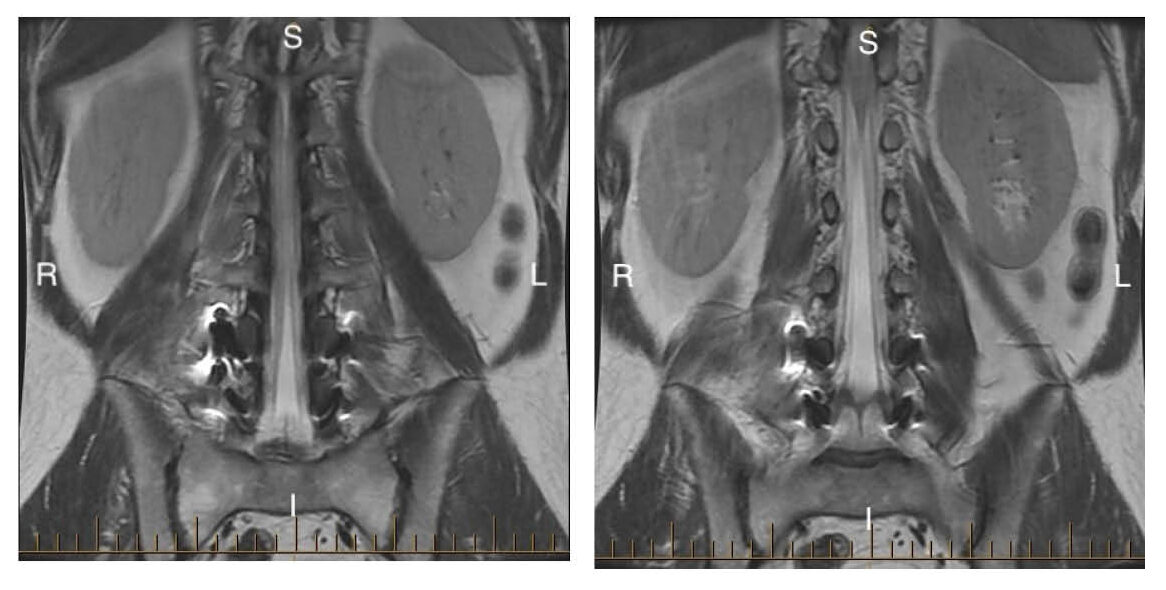
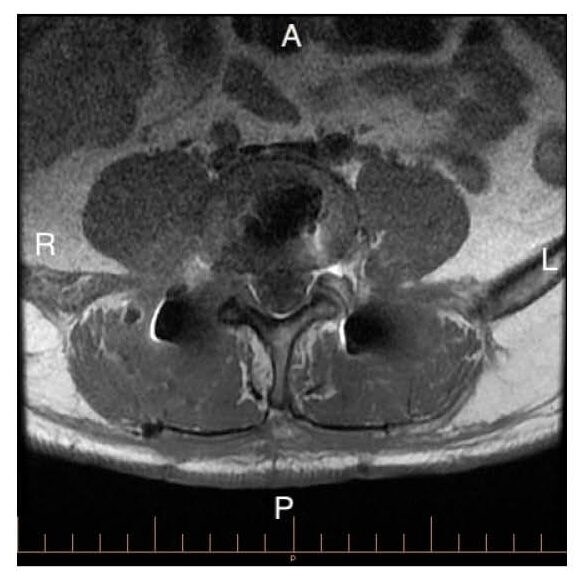
In the emergency department, vital signs were within normal limits. Flexion/extension of the hips was preserved at 5/5; however, bilateral plantarflexion was a 3/5 strength, and there was intermittent decreased sensation in the bilateral extremities in a non-dermatomal distribution affecting the feet and ankles and areflexia at the plantar reflexes. MRI of the lumbar spine was negative. (figure 1-6) Laboratory evaluation, including complete blood count and comprehensive metabolic panel, was largely unremarkable. However, inflammatory markers were elevated, with an ESR of 36 mm/hr (reference ≤15) and a CRP of 1.57 mg/dL (reference ≤0.5). (table 1) MRIs of the brain and cervical and thoracic spinal regions were negative. The radiologist noted a nonspecific fluid collection posterior to the right pedicle screw at L4. This did not appear to compress any neurologic structures and was not considered relevant to the current presentation.

| Lab | Results | Units | Normal Limit |
| Sodium | 127 | mEq/L | 136-145 |
| Potassium | 4.2 | mEq/L | 3.5-5.1 |
| Chloride | 88 | mEq/L | 98-107 |
| CO2 | 26 | mEq/L | 23-29 |
| Anion gap | 13 | mmol/L | 4-20 |
| Glucose | 106 | mg/dL | 70-104 |
| BUN | 15 | mg/dL | 8-21 |
| Creatinine | 0.8 | mg/dL | 0.9-1.5 |
| GFR | 109.2 | mL/min | 75.0-116.0 |
| Calcium | 9.3 | mg/dL | 8.8-10.2 |
| WBC | 8.9 | K/cumm | 4.5-10.9 |
| RBC | 5.06 | mil/cumm | 4.7-6.1 |
| HGB | 15.3 | gm/dL | 14.0-18.0 |
| HCT | 43.5 | % | 42.0-52.0 |
| MCV | 86 | fL | 80-98 |
| MCH | 30.2 | pg | 23-31 |
| MCHC | 25.2 | g/dL | 32-36 |
| RDW | 12.7 | % | 11.5-14.5 |
| PLT | 308 | K/cumm | 140-400 |
| MPV | 8.4 | fL | 7.4-10.4 |
| CRP | 1.57 | mg/dL | 0-0.50 |
| ESR | 36 | mm/hr | 0-15 |
| Blood culture | No growth at 5 days | ||
|
Table 1 |
|||
Due to the non-dermatomal distribution, elevated CRP and ESR, and involvement of S1-S2 reflexes, CSF infection and inflammatory causes were considered. A lumbar puncture was performed. CSF was sent for culture, complete blood count (CBC), protein, and glucose. (table 2) Empiric trimethoprim-sulfamethoxazole was given while waiting culture results due to concern for potential infection. The cultures returned after 72 hours with no growth, ruling out infection, and CSF analysis demonstrated albuminocytologic dissociation consistent with GBS. An elevated RBC count in the CSF was a likely consequence of spinal tap. Due to the patient’s concerning symptoms, he was transferred to a nearby hospital 7 days after admission where a neurology team continued to manage his case. The patient was treated with intravenous immunoglobulin (IVIG) for GBS but had an adverse reaction of psychosis. IVIG was stopped, and the patient underwent plasmapheresis treatment.
| Lab | Results | Units | Normal Limit |
| WBC Count | 3 | /cumm | 0-5 |
| RBC Count | 41 | /cumm | 1-5 |
| CSF Glucose | 63 | mg/dL | 40-70 |
| CSF Protein | 1302 | mg/dL | 15-45 |
| CSF Culture | No growth at 72 hours | No growth | |
|
Table 2 |
|||
Though the patient reported improvement at his two-month and four-month postoperative follow-up, he still experienced weakness but regained full sensation and reflexes. He was undergoing physical therapy for both his back and GBS symptoms at both of these visits. At his six-month postoperative visit, he complained of mild weakness but was overall doing well. (figure 7)

Discussion
Our patient’s initial presentation raised concern for a common postoperative complication. (Table 3)
| Category | Example | Diagnostic Test |
| Hemorrhagic | Delayed epidural hematoma | MRI without contrast (emergent)
MRI with contrast (diagnostic) |
| Infectious | Epidural Abscess
Meningitis |
MRI with IV contrast
Laboratory evaluation for systemic infection (CBC) Lumbar puncture |
| Hardware malposition | Cage migration | CT without contrast (emergent)
MRI if neural compression suspected |
| Ischemic | Spinal cord ischemia | MRI lumbar spine without and with contrast |
|
Table 3 |
||
However, the specific loss of plantar flexion and absence of ankle reflexes were more consistent with an S1–S2 lesion, which would not typically result from an L4–L5 injury. Furthermore, MRI of the brain and spine (Figures 1–6) appeared normal. In this setting, the differential must be broadened to include atypical disease. Lumbar puncture revealed elevated protein and normal WBCs, ESR, and CRP, findings consistent with Guillain-Barré Syndrome (GBS), while CSF cultures were negative.
Notably, this was the patient’s first onset of GBS, with spinal fusion likely serving as the trigger. Orthopedic surgery has rarely been reported as a precipitant of GBS (10). Sipila et al concluded a relative risk of 6.28 in patients who had surgery within six weeks of onset of GBS symptoms. (10, 11) Orthopedic surgery is the most strongly correlated surgical specialty with post operative GBS. (6, 12) In such cases, symptoms often progress more rapidly than in typical presentations, underscoring the importance of prompt recognition and treatment to prevent diaphragmatic weakness and respiratory compromise (12). Interestingly, in this patient, progression was slower than expected for a postoperative GBS: one week after symptom onset, deficits were limited to plantarflexion weakness and loss of S1 reflexes.
The patient’s family history was significant for GBS in his father, suggesting a potential genetic contribution. While GBS is predominantly sporadic, a hereditary predisposition has been proposed in some cases (7). This highlights the importance of obtaining a thorough family history when evaluating postoperative neurological complications. There are three subtypes of GBS: demyelinating form (acute inflammatory demyelinating polyneuropathy), the axonal form (acute motor-sensory axonal neuropathy), and the variant form (Miller-Fisher syndrome). The demyelinating form is the most common subtype of GBS; however, in postoperative versus infection onset GBS, there is an increased incidence of the axonal form, but all subtypes have been recorded as a postoperative complication. (11, 13) The axonal form is more aggressive and leads to faster respiratory decay than the classic, demyelinating form. Diagnosis is made with clinical presentation and the aid of analysis of cerebrospinal fluid for albuminocytologic dissociation and nerve conduction studies, but there is not a current gold standard. In the presence of bilateral, relatively symmetric, progressive weakness with decreased or absent reflexes and no alternative causes, GBS is the leading potential diagnosis. If diagnostic uncertainty remains, nerve conduction studies and albuminocytologic dissociation in CSF can help confirm GBS. Some subtypes of GBS have antibody correlations as well. (3,5,9,14).
Initial treatment consists of intravenous immunoglobulin (IVIG) and plasma exchange, both of which have been found effective in promoting the improvement and reduction of morbidity. Choice of treatment depends on center expertise and availability, as both are considered first-line. (3-4,9). Despite treatment, up to 20% of patients have residual disability, with a mortality of less than 5% (2-4).
The strengths of this case report include a thorough diagnostic workup, incorporating MRI imaging, cerebrospinal fluid analysis, and an infectious evaluation, all of which support the diagnosis of Guillain-Barré Syndrome. Additionally, this case highlights a clinically significant adverse reaction to IVIG, requiring transition to an alternative first-line treatment option, and offering valuable insight into real-world management considerations. The inclusion of longitudinal outpatient orthopedic surgery follow-up further strengthens the report by illustrating the patient’s recovery trajectory over time.
However, this case is limited by incomplete access to detailed inpatient and outpatient neurology management records after the patient was transfered. Furthermore, there was no documentation identifying the specific subtype of Guillain-Barré Syndrome, limiting the ability to fully characterize the disease presentation and compare it to existing literature.
Conclusion
Although Guillain-Barré Syndrome is a rare postsurgical complication, clinicians should keep this in the differential for lower extremity weakness after surgery, particularly if the weakness is relatively symmetric and includes sensory disturbance and areflexia. Prompt CSF analysis and, when necessary, nerve conduction studies are critical for timely diagnosis. Early recognition and intervention remain essential to optimizing outcomes. This case highlights the diagnostic process, treatment and prognosis for patients with postoperative GBS.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Abbreviations
Guillain-Barré Syndrome (GBS), magnetic resonance imaging (MRI), cerebrospinal fluid (CSF), transforaminal lumbar interbody fusion (TLIF), intravenous immunoglobulin (IVIG).
Informed consent: Informed consent from the patient to use his data for publication was obtained via recorded phone call.
Institutional Review Board (IRB): IRB is not applicable to this case study.
Artificial Intelligence Disclosure: AI was used for clarity, tone, and grammatical help.
References
- Shahrizaila N, Lehmann HC, Kuwabara S. Guillain-Barré syndrome. Lancet. 2021 Mar 27;397(10280):1214-1228. doi: 10.1016/S0140-6736(21)00517-1. Epub 2021 Feb 26. PMID: 33647239.
- Weiss, N., Marois, C., Le Guennec, L. et al. Critical insights for intensivists on Guillain-Barré syndrome. Ann. Intensive Care 15, 67 (2025). https://doi.org/10.1186/s13613-025-01464-w
- Leonhard SE, Papri N, Querol L, Rinaldi S, Shahrizaila N, Jacobs BC. Guillain-Barré syndrome. Nat Rev Dis Primers. 2024 Dec 19;10(1):97. doi: 10.1038/s41572-024-00580-4. PMID: 39702645.
- Bellanti R, Rinaldi S. Guillain-Barré syndrome: a comprehensive review. Eur J Neurol. 2024 Aug;31(8):e16365. doi: 10.1111/ene.16365. Epub 2024 May 30. PMID: 38813755; PMCID: PMC11235944.
- van den Berg B, Walgaard C, Drenthen J, Fokke C, Jacobs BC, van Doorn PA. Guillain-Barré syndrome: pathogenesis, diagnosis, treatment and prognosis. Nat Rev Neurol. 2014 Aug;10(8):469-82. doi: 10.1038/nrneurol.2014.121. Epub 2014 Jul 15. PMID: 25023340.
- Rudant J, Dupont A, Mikaeloff Y, Bolgert F, Coste J, Weill A. Surgery and risk of Guillain-Barré syndrome: A French nationwide epidemiologic study. Neurology. 2018;91(13):e1220-e1227. doi:10.1212/WNL.0000000000006246
- Khanmohammadi S, Malekpour M, Jabbari P, Rezaei N. Genetic basis of Guillain-Barre syndrome. J Neuroimmunol. 2021;358:577651. doi:10.1016/j.jneuroim.2021.577651
- Elendu C, Osamuyi EI, Afolayan IA, et al. Clinical presentation and symptomatology of Guillain-Barré syndrome: A literature review. Medicine (Baltimore). 2024;103(30):e38890. doi:10.1097/MD.0000000000038890
- Walling AD, Dickson G. Guillain-Barré syndrome. Am Fam Physician. 2013 Feb 1;87(3):191-7. PMID: 23418763.
- Bao L, Chen X, Li Q, Zhang R, Shi H, Cui G. Surgery and Guillain-Barré Syndrome: A Single-Center Retrospective Study Focused on Clinical and Electrophysiological Subtypes. Neuropsychiatr Dis Treat. 2020;16:969-974. Published 2020 Apr 15. doi:10.2147/NDT.S241128
- Sipilä JO, Soilu-Hänninen M. The incidence and triggers of adult-onset Guillain-Barré syndrome in southwestern Finland 2004-2013. Eur J Neurol. 2015;22(2):292-298. doi:10.1111/ene.12565
- Gong Q, Liu S, Liu Y, et al. Guillain-Barré syndrome triggered by surgery in a Chinese population: a multicenter retrospective study. BMC Neurol. 2021;21(1):40. Published 2021 Jan 28. doi:10.1186/s12883-021-02067-1
- Li X, Zhang C. Guillain-Barré syndrome after surgery: a literature review. Front Neurol. 2024;15:1368706. Published 2024 Apr 4. doi:10.3389/fneur.2024.1368706
- van Doorn PA, Van den Bergh PYK, Hadden RDM, et al. European Academy of Neurology/Peripheral Nerve Society Guideline on diagnosis and treatment of Guillain-Barré syndrome. Eur J Neurol. 2023;30(12):3646-3674. doi:10.1111/ene.16073
