
Jonathan Elias BA, OMS-31; Lothar Vidal BS, OMS-31; Timothy Gelatt BS, OMS-31; Sami Dakhel MS, OMS-31; Richard Jermyn DO, Dean1; James Sanfilippo MD2
1Rowan-Virtua School of Osteopathic Medicine
2Virtua Health System
DOI: http://doi.org/10.70709/v3pg0260a73h1o
Abstract
Purpose
To determine the effectiveness of the combinatorial treatment of microwave ablation with a vertebroplasty in the reduction of cancer-related back pain, functionality, and daily morphine equivalent consumption. Retrospective studies have demonstrated the efficacy of microwave ablation (MWA) and percutaneous vertebroplasty (VP) in improving cancer-related back pain; however, a systematic review and meta-analysis has yet to be conducted.
Methods
The systematic review and meta-analysis followed the 2020 PRISMA guidelines. Five online databases (Cochrane, Embase, PubMed, Web of Science, Scopus) were screened. Included were studies that reported 4-week and/or 12-week visual analogue scales (VAS) scores, Oswestry disability index (ODI) measures, and daily morphine equivalent consumption (DMC).
Results
Four studies fit our inclusion criteria, yielding a combined sample size of 117 patients. Our results show clinically and statistically significant results of utilizing MWA with VP at both 4-weeks and 12-weeks. At 4 weeks post-intervention, VAS, DMC, and ODI scores were significantly improved. Reduction in VAS and DMC scores was also significant at 12 weeks post-intervention. Lack of data prevented assessment of ODI at 12 weeks post-intervention.
Conclusions
Microwave ablation in combination with vertebroplasty greatly reduced pain, disability, and opioid consumption in patients with metastatic spinal cancer over a 4-week and 12-week timeline.
Keywords: Microwave Ablation, Vertebroplasty, Spinal Neoplasm, Back Pain, Opioid Use
Introduction
It is estimated that 20–80% of advanced malignant tumors will metastasize to bones, with the spine being the most common site of bone metastasis (60–70%) [1]. Their incidence is increasing due to advances in imaging, treatments, and cancer survival rates [2, 3]. Cadaveric studies indicate spinal metastases in 30–90% of terminal cancer patients, highlighting significant morbidity. The spine’s weight-bearing function and adjacent vital anatomical structures, as well as the potential for pathological fractures and nerve compression, make spinal metastases particularly problematic [4].
Treatment options for spinal metastases aim to relieve pain and preserve nerve function, often using minimally invasive techniques. Galibert, et al, first reported using one such technique, vertebroplasty (VP), in 1987 to treat vertebral angioma [5]. This procedure involves injecting bone cement into the fractured vertebra, providing immediate pain relief and preventing further vertebral degeneration [8]. Its benefits for pain relief and vertebral bone strengthening have been widely documented and when used in combination with microwave ablation (MWA), is known to be effective in reducing the pain of patients with spinal metastases [6, 7].
MWA reduces the invasiveness of cancer treatment by using microwave energy to destroy cancerous tumors, including those in the liver and bones [9, 10]. The resulting reduction in tumor size alleviates pressure on the nervous system and surrounding structures [9]. This procedure begins with a small incision in the targeted zone to allow the insertion of a flexible probe into the tumor under guidance of specialized imaging. The probe then emits an electromagnetic field that generates energy in the form of heat, leading to tumor necrosis [11]. Compared to traditional methods such as surgery, MWA reduces tissue damage, tumor metastasis stimulation, and the likelihood of postoperative recurrence [12]. The procedure is also less affected by tissue characteristics such as impedance and perfusion, prevalent in approaches like radiofrequency ablation and cryoablation, allowing MWA to produce large ablation zones rapidly [10, 13]. Although the limited research regarding its use in bone tumors raises concerns about complications such as fractures and neurocutaneous damage, MWA shows promise in treating bone tumors without damaging surrounding healthy tissue [14, 9].
These techniques provide spinal stabilization, relieve mechanical and tumor-related pain, and improve mobility and comfort, thereby possibly reducing opioid dependence. However, limited evidence exists on the effects of MWA followed by VP on pain, disability, and daily morphine equivalent consumption (DMC) in metastatic spinal cancer. To address this gap, we conducted a systematic review and meta-analysis evaluating the impact of MWA with VP on these outcomes at 4- and 12-week follow-up. We hypothesize significant reductions in pain, disability, and opioid consumption following MWA with VP.
Methods
A systematic review and meta-analysis were completed following the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16]. This study aimed to determine the effectiveness of utilizing MWA followed by VP in patients with metastatic spinal cancer. The primary outcome analyzed was the Visual Analogue Scale (VAS), with secondary outcomes of Oswestry Disability Index (ODI) and DMC.
Search Procedure
A systematic review was conducted using five online databases (Cochrane, PubMed, Embase, Web of Science, Scopus) on April 6, 2025, for studies to be screened in the analysis. The NIH MeSH tool was utilized to determine key terms for the search string, and Boolean operators were used to yield the following string: (“Microwave ablation” OR “MWA”) AND (“Percutaneous Vertebroplasty”) AND (“VAS” OR “NRS” OR “Pain”). The same string was utilized on all five databases.
Inclusion and Exclusion Criteria
Retrospective, randomized controlled trials (RCT), and cohort studies were included in the analysis. The studies must have maintained a patient population consisting of those with metastatic spinal cancer who underwent MWA followed by VP, and included VAS, ODI, or DMC presented as pre-intervention and post-intervention mean and standard deviation (SD). Furthermore, included studies must have been available as full text in English (or English translation). The following study types were excluded: cross-sectional, case-control, conducted on animals, reviews, and meta-analyses. Those reported solely as abstracts, unavailable in English, without data specific to metastatic spinal cancer patients, or lacking pre-intervention and post-intervention VAS, ODI, or DMC means and SD for this population were also excluded.
Study Selection
Retrieved results were imported into Rayyan.ai for review. Artificial intelligence was utilized in the detection of duplicates; however, all detected duplicates were confirmed to be true duplicates before deletion. Two independent reviewers examined each study, and any ties were resolved by a third author. The search string yielded 54 studies (1 from Cochrane, 4 from PubMed, 30 from Embase, 9 from Web of Science, 10 from Scopus). After removing 21 duplicates, the reviewers excluded 22 additional articles through screening the titles and abstracts of the remaining 33 studies for relevance. The abstracts of the remaining 11 studies were further reviewed, and 7 studies were eliminated. The full-text articles for the remaining 4 studies were retrieved and thoroughly evaluated for eligibility.
Data Extraction and Statistical Analysis
Two independent blinded reviewers extracted the following data: title, author, year of publication, sample size, locations of primary cancer, and patient pre-intervention and post-intervention (4-weeks and 12-weeks) VAS, ODI, and DMC in mean ± SD. A meta-analysis was performed using SPSS v29. The measurement of Cohen’s d using a random effects model was assessed as a measure of the effect size of VP with MWA on the outcomes of VAS, ODI, and DMC. Cohen’s d value ≥ 0.8 was considered clinically significant, and a p-value ≤ 0.05 was considered statistically significant, both with a 95% confidence interval. VAS and DMC were individually analyzed at 4-weeks and 12-weeks post-intervention, while ODI was only analyzed at 4-weeks due to availability of data. The visualization of the data was facilitated through the utilization of forest plots generated by SPSS v29. Heterogeneity was assessed using I2, H2, and τ2.
Risk of Bias Assessment
The four included studies underwent a diligent assessment of bias by two independent reviewers. Risk of bias for these retrospective studies included in the final analysis was appraised using the Cochrane Methods Risk of Bias In Non-Randomised Studies of Intervention (ROBINS-1) [17]. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to determine the quality of evidence of the included studies (Table 5) [18].
Results
Search Results
Four retrospective studies fit our inclusion criteria and were included in the systematic review and meta-analysis [1, 2, 8, 19]. The selection process is illustrated in a PRISMA flow chart (Figure 1).

Summary of Findings
The summary of each included study is presented in Table 1. The characteristics of each study are presented in Table 2.
Table 1. Summary of findings regarding the title, author, year of publication, type of study, recruitment period, intervention, sample size (N), age (mean ± SD), MWA power/duration of each included study. Abbreviations: MWA; microwave ablation, VP; vertebroplasty, PVP; percutaneous vertebroplasty, W; watts, kJ; kilojoules, min; minutes
| Title | Author; Year | Country | Study Design | Recruitment Period | Intervention | Number of Patients (N) | Mean Age (Years) | MWA Power/Duration |
| Computed tomography-guided microwave
ablation combined with percutaneous vertebroplasty for treatment of painful high thoracic vertebral metastases |
Wu, Linlin; 2021 [8] | China | Retrospective Chart Review | January 2015 to June 2020 | CT-guided MWA with PVP | 23 | 64.35 ± 8.28 | 20 – 30 W; 3 – 5 min |
| Assessing long-term locoregional control of spinal osseous metastases after
microwave ablation |
Motaghi, Mina; 2022 [2] | USA | Retrospective Chart Review | 2013 to 2020 | MWA with VP | 28 | 68.2 ± 9.2 | 2.6 – 4.1kJ; 3.5 – 5.5 min |
| PVP with or without microwave ablation for the
treatment of painful spinal metastases from NSCLC: a retrospective case-control study |
Liu,Yiming; 2023 [19] | China | Retrospective Case-Control Study | October 2014 to October 2021 | MWA with PVP | 28 | 56.14 ± 9.74 | 25 – 45 W; N/A |
| Microwave ablation combined with vertebral
augmentation under real-time temperature monitoring for the treatment of painful spinal osteogenic metastases |
Fan, Jing; 2020 [1] | China | Retrospective Chart Review | April 2015 to March 2021 | CT-guided MWA with VP | 38 | 60.98±14.15 | 20 – 50 W; 1 – 6 min |
Table 2. Summary of findings regarding the title, author, year of publication, inclusion criteria, outcomes measured and collected, and significant findings.
| Title | Author; Year | Inclusion Criteria | Outcomes Measured | Main Findings |
| Computed tomography-guided microwave
ablation combined with percutaneous vertebroplasty for treatment of painful high thoracic vertebral metastases |
Wu, Linlin; 2021 | Tumors located at the levels of T1–T4, target lesion had focal and persistent pain, VAS score > 4, the presence of persistent or recurrent pain after radiotherapy, or ineligibility for radiotherapy, estimated life expectancy of at least 3 months | Baseline and postoperatively 24 hours, 1 week, 4 weeks, 3 months, and 6 months after surgery; VAS, ODI, and DMC | VAS and DMC significant at all timepoints; ODI significant at 1, 3, 6 months post-intervention. |
| Assessing long-term locoregional control of spinal osseous metastases after
microwave ablation |
Motaghi, Mina; 2022 | ≤ 3 vertebral levels containing osseous
spinal metastases, VAS score > 6, not controlled by analgesics and resulting in a return visit to the oncologist, not a candidate for, could not complete, or had previously declined radiation therapy, positive biopsy either before or during MWA procedure, availability of both pre- and post-procedure PET/CT scans for response assessment |
Baseline and postoperatively at 24 hours, 4 weeks, and 6 months after surgery; VAS | VAS was significant at all timepoints. |
| PVP with or without microwave ablation for the
treatment of painful spinal metastases from NSCLC: a retrospective case-control study |
Liu, Yiming; 2023 | 18–75 years old, primary lesion confirmed as non-small lung cell cancer, single spinal metastasis confirmed by magnetic resonance or computed tomography, VAS score > 5, the presence of persistent or recurrent pain after extracorporeal radiotherapy or standard analgesics, local tumor diameter < 4 cm, Karnofsky score > 60 | Baseline and postoperatively at 1 week, 4 weeks, 3 months, and 6 months; VAS, ODI, DMC, Quality of Life, and Local Tumor Progression | VAS and DMC were significant at all timepoints. |
| Microwave ablation combined with vertebral
augmentation under real-time temperature monitoring for the treatment of painful spinal osteogenic metastases |
Fan, Jing; 2020 | Clear pathological diagnosis of primary tumor or vertebral metastasis, focal pain localized to a certain part of the vertebral body, VAS
scores ≥ 4, osteogenic metastasis type of vertebral metastasis, ≤ 4 lesions under treatment per patient, intractable pain with limited effects of radiotherapy, chemotherapy, and opioid analgesic drugs, estimated survival time of at least 3 months. |
Baseline and postoperatively 24 hours, 1 week, 4 weeks, 3 months, and 6 months after surgery; VAS, ODI, and DMC | VAS and DMC were significant at all timepoints; ODI significant at 1, 3, 6 months post-intervention. |
Effects of Intervention
The four retrospective studies included in the review yielded a total sample size of 117 patients with metastatic spinal cancer for analysis. We found clinical and statistical significance in the reduction of VAS scores at both 4-weeks (Cohen’s d = 4.00, p = 0.00, 95% CI [2.83 – 5.17]) and 12-weeks (Cohen’s d = 4.34, p = 0.00, 95% CI [3.00 – 5.67]) following MWA and VP, portrayed in Figure 4. Similarly, there was a notable clinical and statistical significance in the reduction of DMC at 4-weeks (Cohen’s d = 4.50, p = 0.01, 95% CI [1.26 – 7.73]) and at 12-weeks (Cohen’s d = 4.56, p = 0.01, 95% CI [1.14 – 7.99]), portrayed in Figure 5. There was also a significant decrease in ODI scores analyzed at 4-weeks (Cohen’s d = 3.29, p = 0.00, 95% CI [2.75 – 3.84]), portrayed in Figure 6. A summary of the results has been provided in Table 3.
The origins of the metastases were collected and are presented in Table 4.
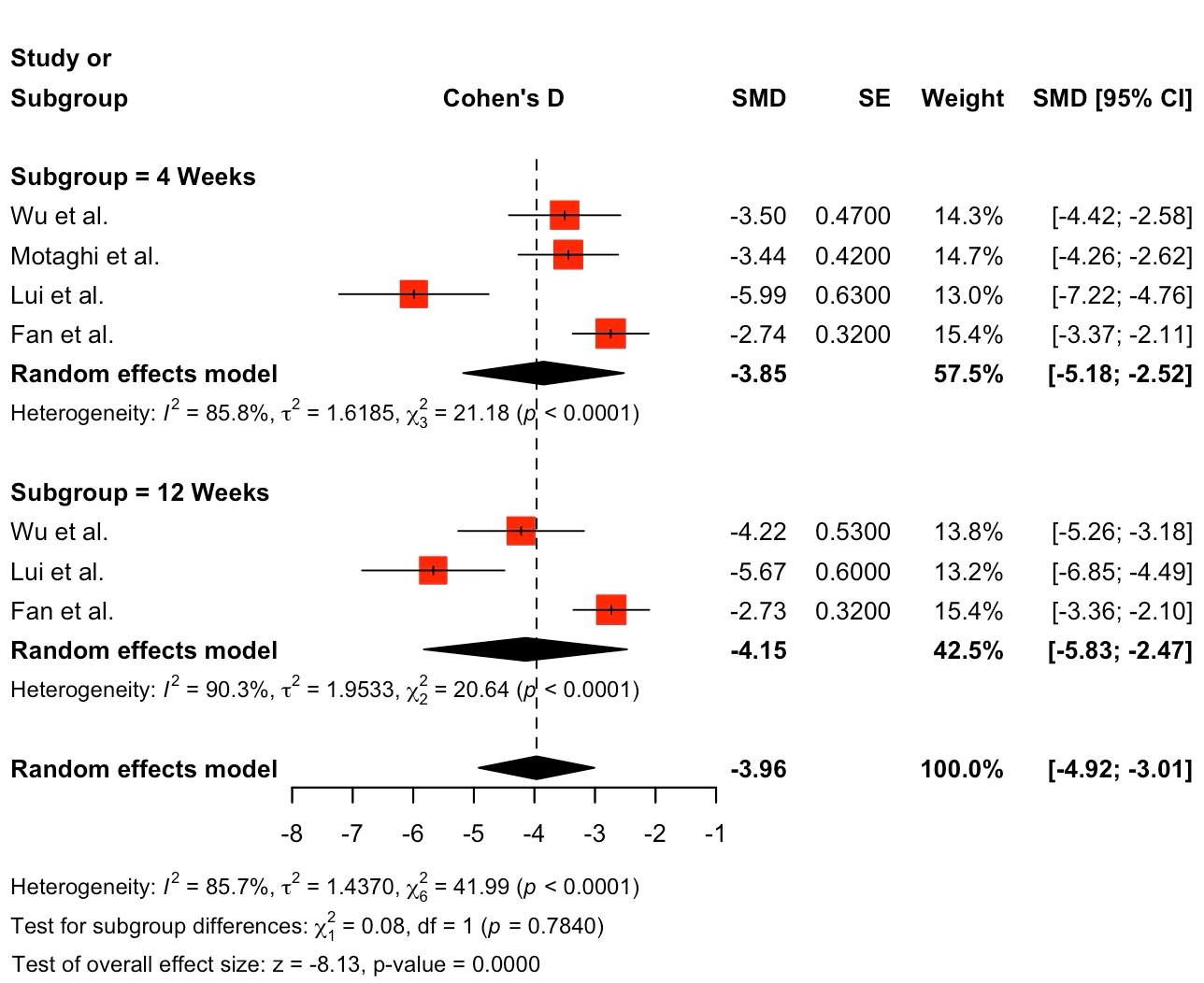
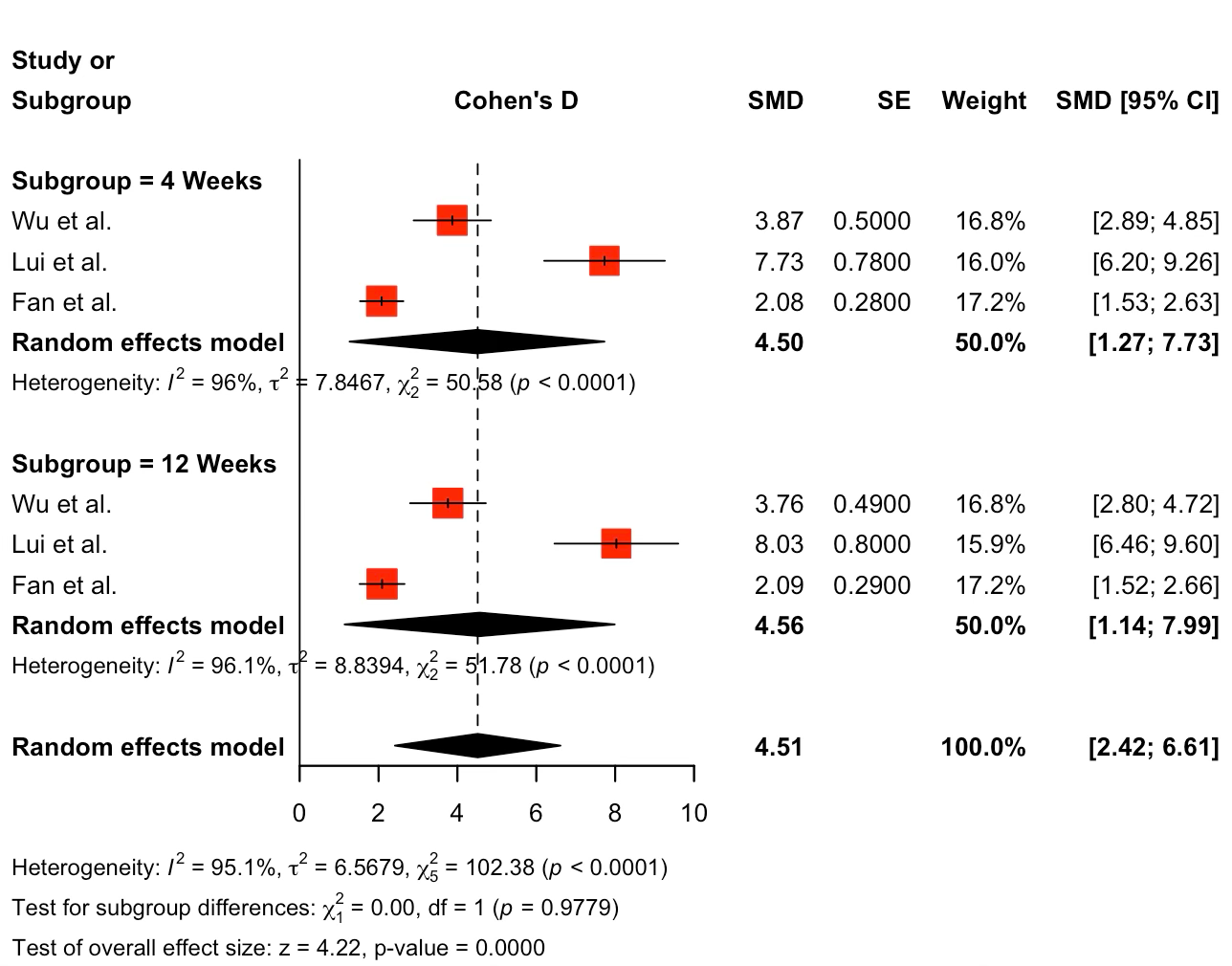
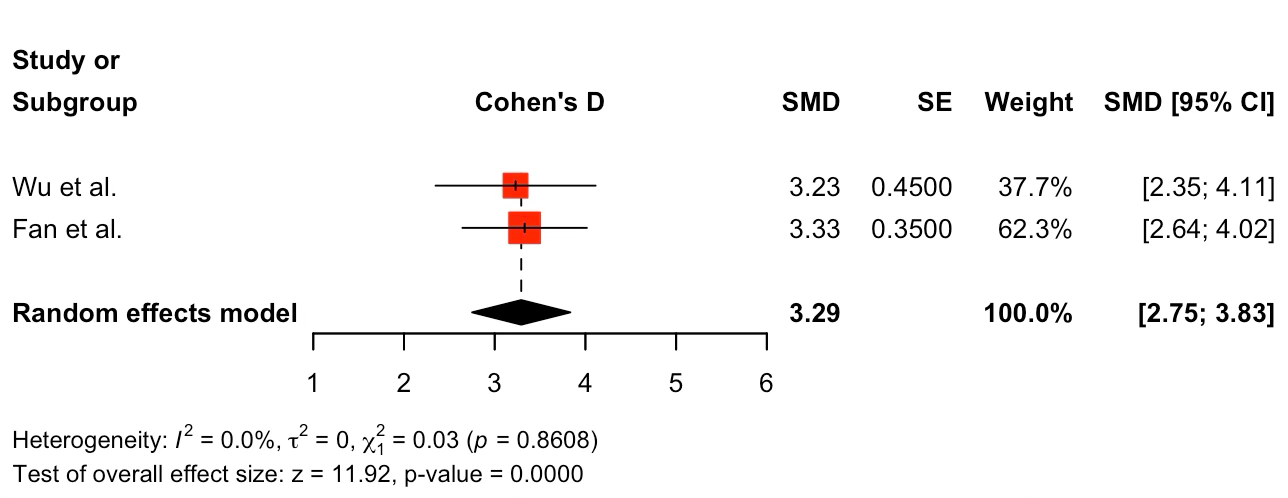
Table 3. Summary of the data portraying the VAS, DMC, and ODI analysis at 4-weeks and 12-weeks post-intervention, and ODI at 4-weeks post-intervention
| Time Post-Treatment | VAS | ODI | DMC |
| 4-Weeks | |||
| Subgroup Overall Effect Size (Cohen’s d) | -3.85 | 3.29 | 4.50 |
| 95% Confidence Interval | -5.18, -2.52 | 2.75, 3.84 | 1.26, 7.73 |
| 12-Weeks | |||
| Subgroup Overall Effect Size (Cohen’s d) | -4.15 | N/A | 4.56 |
| 95% Confidence Interval | -5.83, -2.47 | N/A | 1.14, 7.99 |
| Difference of Effect Size Between Timeframes | 0.30 | N/A | 0.06 |
Table 4. Summary of the original sites of malignancy
| Author | Lung | Breast | Esophagus | Other | Total |
| Wu et al. | 12 | X | 5 | 6 | 23 |
| Motaghi et al. | 7 | 11 | X | 10 | 28 |
| Liu et al. | 28 | X | X | X | 28 |
| Fan et al. | 14 | 7 | 5 | 12 | 38 |
| Total | 61 | 18 | 10 | 28 | 117 |
Risk of Bias and Certainty of Evidence Assessment
A modified version of GRADE was used to assess the quality of evidence of each study included in the review and meta-analysis. Although none were found to have serious levels of bias, the study design (nonrandomized, retrospective chart review) resulted in the downgrade of their quality of evidence (Table 5).
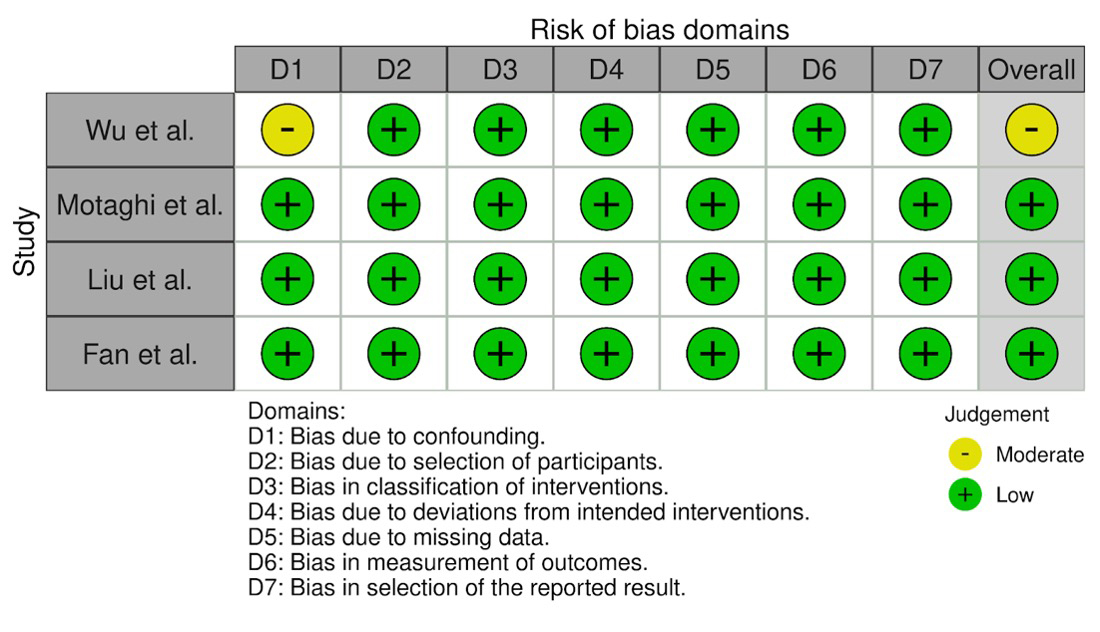
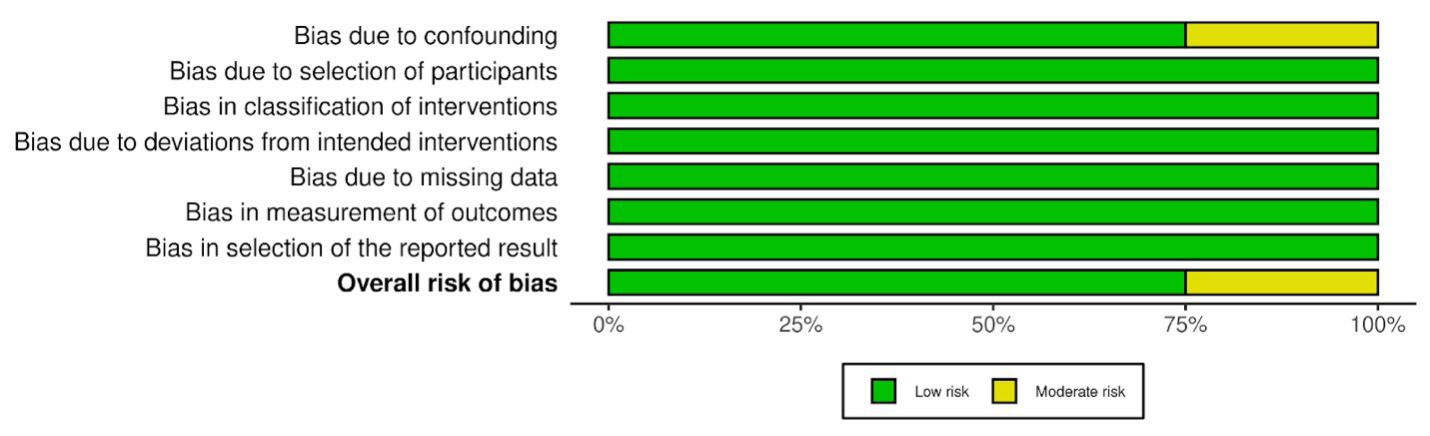
The assessment of bias using the ROBINS-1 tool indicated one study of moderate bias, with the other three studies maintaining a low level of bias (Figure 5 and Figure 6) [20]. The retrospective review conducted by Wu et al. received a moderate level of bias in the D1 domain due to its unexplained specific inclusion and exclusion criteria and failure to cite other literature.
Table 5. Summary of modified GRADE assessment of quality of evidence for each included study
| Modified Grading of Recommendations Assessment, Development and Evaluation Criteria for Included Articles | ||||||||
| Author | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Other Factors | Final Grade |
| Wu et al. | Retrospective Study | Not serious | Serious | Not serious | Not serious | Undetected | N/A | Moderate |
| Motaghi et al. | Retrospective Study | Not serious | Serious | Not serious | Not serious | Undetected | N/A | Moderate |
| Liu et al. | Retrospective Study | Not serious | Serious | Not serious | Not serious | Undetected | N/A | Moderate |
| Fan et al. | Retrospective study | Not serious | Serious | Not serious | Not serious | Undetected | N/A | Moderate |
Discussion
This systematic review with meta-analysis highlights the possibility of MWA followed by VP as an effective treatment option in metastatic spinal cancer by demonstrating the statistical and clinical improvement in VAS, DMC and ODI. When compared to pre-treatment levels, reductions in VAS and DMC were found to be clinically significant at 4- and 12-weeks post-intervention, while ODI scores showed clinically and statistically significant increases in scores 4 weeks post-treatment.
Other benefits of this treatment may include increased spinal stability and improved survival due to a reduction in the necessity for opioid therapy. A retrospective study conducted in 2022 by Dohzono et al. explored the use of opioids and overall survival in patients with spinal metastases [34]. The results demonstrated that the use of opioids was associated with a doubled risk of shorter survival [34]. The study also noted that more patients on opioid therapy had tumor-related spinal instability.
Several mechanisms can cause pain in metastatic cancer of the spine, such as compression of the periosteum caused by tumor invasion in the vertebral body, neural fiber compression, and instability resulting from vertebral body degradation or fracture [21]. Neoplasm-induced spinal instability arises when tumor-related disruption of vertebral architecture results in mechanical pain, evolving spinal deformity, and/or functional impairment of neural structures under normal biomechanical stress [35].
MWA is known to reduce the pain associated with metastatic spinal cancer and help with local tumor control, but it does not address spinal instability, while VP alone can yield reduction in pain but has limited effect on tumor control [22, 23]. The exact etiology of cancer pain is still unknown, but several theories have been proposed regarding the mechanism by which MWA reduces or eliminates patient pain [24]. In this procedure, microwaves are directed into the tumor via an antenna with the goal of increasing tumor cell temperature to damage their cell membrane and cause destruction of the cells. This provides targeted treatment to the tumor and minimizes the damage to structures around the tumor [26]. One proposed theory is that MWA may block pain transmission by destroying the afferent sensory nerve fibers affected by the tumor [25]. Another possibility is that, by directly shrinking the size of the tumor, the procedure eliminates compression effects on neural structures [12]. Finally, some suggest it results from the destruction of tumor cells involved in the production of cytokines which are involved in inflammation that results in pain and other cancer symptoms [27, 28]. Cytokines’ involvement in pain is thought to be related to their promotion of the release of immune mediators from tumor cells that stimulate the local nociceptor [29]. It is known that spinal proinflammatory mediators like IL-1beta can enhance pain signaling and is involved in the development of hyperalgesia and analgesic tolerance [30]. By eliminating the production of these proinflammatory cytokines through MWA, pain may also be decreased.
The combination of MWA and VP not only addresses the cancer-related back pain, but it also allows adequate distribution of the intervertebral cement to increase stability of the affected vertebrae [8]. The most common complication of vertebroplasty is cement leakage, which has been reported at a frequency of 50-80% in patients undergoing vertebroplasty for the treatment of a single vertebra [31, 32]. In 2023, Fan et al. reported a significant reduction in cement leakage post MWA following VP [1]. One possible explanation for this phenomenon is the ability of MWA to create a thermal cavity, allowing the cement to adequately fill the ablation zone [33]. These factors could contribute to the significant decrease in VAS scores and DMC as well as the increase in ODI found in our analysis.
Comparing our analysis of MWA as an adjunct to VP monotherapy in painful spinal metastases, a study conducted by Lim et al. assessing VP alone demonstrated significant improvements in VAS; however, the study did not measure ODI or DMC [36]. Additionally, a retrospective case-control study conducted by Liu et al. directly compared VP alone to VP with MWA, with results demonstrating that the utilization of MWA as an adjunct yields longer lasting pain relief, improved quality of life, lower tumor progression, and lower cement leakage rates compared to VP alone [19].
Limitations
This comprehensive systematic review and meta-analysis includes several limitations. First, the retrospective nature of all included studies inherently carries a risk of selection bias and limits the ability to control for all possible confounding factors in the study. Another significant limitation is the heterogeneity among the studies included in this review. Utilizing VAS scores to assess heterogeneity, τ2 = 1.437 and I2 = 85.7% This heterogeneity stems from variations in patient populations, intervention protocols, and sample size. The patients with metastatic spinal cancer included in this study had diverse primary cancer sites (Table 4). The response to treatment can vary significantly between the different types of primary cancers, which can potentially influence VAS, ODI, and DMC outcomes.
In addition, differences in how microwave ablation was performed, such as the power settings used or duration of ablation, or variations in the type and amount of bone cement used in vertebroplasty can affect treatment efficacy and ultimately modulate the total heterogeneity of this review. Finally, the lack of control for demographic factors such as sex, age and clinical comorbidities along with the small sample size of study participants led to additional variability in the results. All these factors pose limitations on our ability to establish definitive conclusions on the causal relationship of VAS, ODI and DMC in microwave ablation with vertebroplasty.
Future randomized controlled trials are needed to validate these findings and explore the long-term outcomes of microwave ablation with vertebroplasty. Randomized controlled trials directly comparing VP alone to VP with MWA would serve to determine the role of MWA in the combinatorial treatment. In addition, future research exploring patient-reported outcomes and quality of life metrics over longer study durations will be essential to evaluating the clinical benefits and optimal treatment protocols for patients with metastatic spinal cancer.
Conclusion
MWA followed by VP may significantly reduce disability, improve pain management and decrease daily morphine equivalent consumption in patients with metastatic spinal cancer.
References
- Fan, J., Zhang, X., Li, P. et al. Microwave ablation combined with vertebral augmentation under real-time temperature monitoring for the treatment of painful spinal osteogenic metastases. BMC Neurol 23, 219 (2023). https://doi.org/10.1186/s12883-023-03263-x
- Motaghi M, England RW, Nejad NH, Sankaran N, Patel AM, Khan MA. Assessing long-term locoregional control of spinal osseous metastases after microwave ablation. J Clin Neurosci. 2022;104:48-55. doi:10.1016/j.jocn.2022.07.025
- Coleman RE, Rubens RD. The clinical course of bone metastases from breast cancer. Br J Cancer. 1987;55(1):61-66. doi:10.1038/bjc.1987.13
- Sciubba DM, Gokaslan ZL. Diagnosis and management of metastatic spine disease. Surg Oncol. 2006;15(3):141-151. doi:10.1016/j.suronc.2006.11.002
- Galibert P, Deramond H, Rosat P, Le Gars D. Note préliminaire sur le traitement des angiomes vertébraux par vertébroplastie acrylique percutanée [Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty]. Neurochirurgie. 1987;33(2):166-168.
- Cotten A, Boutry N, Cortet B, et al. Percutaneous vertebroplasty: state of the art. Radiographics. 1998;18(2):311-323. doi:10.1148/radiographics.18.2.9536480
- Chen L, Hou G, Zhang K, et al. Percutaneous CT-Guided Microwave Ablation Combined with Vertebral Augmentation for Treatment of Painful Spinal Metastases. AJNR Am J Neuroradiol. 2022;43(3):501-506. doi:10.3174/ajnr.A7415
- Wu L, Fan J, Yuan Q, Zhang X, Hu M, Zhang K. Computed tomography-guided microwave ablation combined with percutaneous vertebroplasty for treatment of painful high thoracic vertebral metastases. Int J Hyperthermia. 2021;38(1):1069-1076. doi:10.1080/02656736.2021.1951364
- Tomasian A, Jennings JW. Spine Microwave Ablation: Safety and Efficacy for Treatment of Vertebral Metastases. AJNR Am J Neuroradiol. 2022;43(3):E9-E10. doi:10.3174/ajnr.A7439
- Cazzato RL, de Rubeis G, de Marini P, et al. Percutaneous microwave ablation of bone tumors: a systematic review. Eur Radiol. 2021;31(5):3530-3541. doi:10.1007/s00330-020-07382-8
- Poulou LS, Botsa E, Thanou I, Ziakas PD, Thanos L. Percutaneous microwave ablation vs radiofrequency ablation in the treatment of hepatocellular carcinoma. World J Hepatol. 2015;7(8):1054-1063. doi:10.4254/wjh.v7.i8.1054
- Yao Y, Zhu X, Zhang N, et al. Microwave ablation versus radiofrequency ablation for treating spinal metastases. Medicine (Baltimore). 2023;102(25):e34092. doi:10.1097/MD.0000000000034092
- Brace CL. Microwave ablation technology: what every user should know. Curr Probl Diagn Radiol. 2009;38(2):61-67. doi:10.1067/j.cpradiol.2007.08.011
- Tomasian A, Gangi A, Wallace AN, Jennings JW. Percutaneous Thermal Ablation of Spinal Metastases: Recent Advances and Review. AJR Am J Roentgenol. 2018;210(1):142-152. doi:10.2214/AJR.17.18205
- Zhang X, Ye X, Zhang K, et al. Computed Tomography‒Guided Microwave Ablation Combined with Osteoplasty for the Treatment of Bone Metastases: A Multicenter Clinical Study. J Vasc Interv Radiol. 2021;32(6):861-868. doi:10.1016/j.jvir.2021.03.523
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Published 2021 Mar 29. doi:10.1136/bmj.n71
- Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. Published 2016 Oct 12. doi:10.1136/bmj.i4919
- Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924-926. doi:10.1136/bmj.39489.470347.AD
- Liu Y, Yuan H, Milan S, Zhang C, Han X, Jiao D. PVP with or without microwave ablation for the treatment of painful spinal metastases from NSCLC: a retrospective case-control study. Int J Hyperthermia. 2023;40(1):2241687. doi:10.1080/02656736.2023.2241687
- McGuinness, LA, Higgins, JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Syn Meth. 2020; 1- 7. https://doi.org/10.1002/jrsm.1411
- Jaipanya P, Chanplakorn P. Spinal metastasis: narrative reviews of the current evidence and treatment modalities. J Int Med Res. 2022;50(4):3000605221091665. doi:10.1177/03000605221091665
- Sagoo NS, Haider AS, Rowe SE, et al. Microwave Ablation as a Treatment for Spinal Metastatic Tumors: A Systematic Review. World Neurosurg. 2021;148:15-23. doi:10.1016/j.wneu.2020.12.162
- Zhang HR, Xu MY, Yang XG, et al. Percutaneous vertebral augmentation procedures in the management of spinal metastases. Cancer Lett. 2020;475:136–142. doi: 10.1016/j.canlet.2020.01.038.
- Schmidt BL. The neurobiology of cancer pain. Neuroscientist. 2014;20(5):546-562. doi:10.1177/1073858414525828
- Toyota N, Naito A, Kakizawa H, et al. Radiofrequency ablation therapy combined with cementoplasty for painful bone metastases: initial experience. Cardiovasc Intervent Radiol. 2005;28(5):578-583. doi:10.1007/s00270-004-0208-0
- Ryan MJ, Willatt J, Majdalany BS, et al. Ablation techniques for primary and metastatic liver tumors. World J Hepatol. 2016;8(3):191-199. doi:10.4254/wjh.v8.i3.191
- Callstrom MR, Charboneau JW, Goetz MP, et al. (2002) Painful metastases involving bone: feasibility of percutaneous CT- and USguided radio-frequency ablation. Radiology 224:87–97
- Vendrell I, Macedo D, Alho I, Dionísio MR, Costa L. Treatment of Cancer Pain by Targeting Cytokines. Mediators Inflamm. 2015;2015:984570. doi:10.1155/2015/984570
- Seruga B., Zhang H., Bernstein L. J., Tannock I. F. Cytokines and their relationship to the symptoms and outcome of cancer. Nature Reviews Cancer. 2008;8(11):887–899. doi: 10.1038/nrc2507.
- Johnston I. N., Milligan E. D., Wieseler-Frank J., et al. A role for proinflammatory cytokines and fractalkine in analgesia, tolerance, and subsequent pain facilitation induced by chronic intrathecal morphine. The Journal of Neuroscience. 2004;24(33):7353–7365. doi: 10.1523/jneurosci.1850-04.2004.
- Lee IJ, Choi AL, Yie M-Y, et al. CT evaluation of local leakage of bone cement after percutaneous kyphoplasty and vertebroplasty. Acta Radiologica. 2010;51(6):649-654. doi:10.3109/02841851003620366
- Liu, Tie MD*; Li, Zhe MD; Su, Qingjun MD*; Hai, Yong MD. Cement leakage in osteoporotic vertebral compression fractures with cortical defect using high-viscosity bone cement during unilateral percutaneous kyphoplasty surgery. Medicine 96(25):e7216, June 2017. | DOI: 10.1097/MD.0000000000007216
- David E, Kaduri S, Yee A, et al. Initial single center experience: radiofrequency ablation assisted vertebroplasty and osteoplasty using a bipolar device in the palliation of bone metastases. Ann Palliat Med. 2017;6(2):118–24.https://doi.org/10.21037/apm.2016.12.02.
- Dohzono S, Sasaoka R, Takamatsu K, Nakamura H. Association between Opioid Requirement and Overall Survival in Patients with Spinal Metastases. Spine Surg Relat Res. 2022;7(3):235-241. Published 2022 Oct 28. doi:10.22603/ssrr.2021-0169
- Murtaza H, Sullivan CW. Classifications in Brief: The Spinal Instability Neoplastic Score. Clin Orthop Relat Res. 2019;477(12):2798-2803. doi:10.1097/CORR.0000000000000923
- Lim BS, Chang UK, Youn SM. Clinical outcomes after percutaneous vertebroplasty for pathologic compression fractures in osteolytic metastatic spinal disease. J Korean Neurosurg Soc. 2009;45(6):369-374. doi:10.3340/jkns.2009.45.6.369
