
Daxton Kennington, OMS 20291; Carson Sautter, OMS 20291; Connor Parry DO2; Nicolette McNair DO2; Keith Kotecki DO3
1Des Moines University of Medicine and Health Sciences
2Valley Hospital Medical Center, Orthopedic Surgery, Las Vegas, Nevada, USA
3Nevada Orthopedic and Spine Center, Las Vegas, NV, USA
DOI: http://doi.org/10.70709/qbghijluqge3j8
Abstract
Background
Total knee arthroplasty (TKA) is a frequently performed orthopedic procedure, providing reliable improvements in pain, function, and quality of life for patients with advanced knee arthritis. Randomized controlled trials (RCTs) are essential for guiding decisions related to implants, surgical techniques, anesthesia, and rehabilitation. However, premature trial discontinuation or nonpublication results in lost data, wasted resources, ethical concerns regarding unshared patient contributions, and potential bias that may misinform clinical practice. The objective of this study is to determine the prevalence and characteristics of discontinued and unpublished phase 3 and 4 TKA-related RCTs registered in the United States between 2013 and 2023.
Materials and Methods
A cross-sectional analysis of ClinicalTrials.gov identified TKA interventional trials during the study period. Trial status and publication outcomes were verified using PubMed, Embase, and Google Scholar. Data on study design, sample size, sponsorship, and intervention type were extracted. Discontinuation and publication rates were summarized descriptively, and associations between trial characteristics and outcomes were analyzed using chi-square and Fisher’s exact tests.
Results
Of 173 trials, 42 (24.3%) were discontinued and 131 (75.7%) were completed; among completed trials, 31 (23.7%) remained unpublished. Discontinuation was significantly more frequent in single-center studies and those enrolling fewer than 100 participants (27.0% and 33.6%, respectively; both P < 0.05). Trials recruiting exclusively within the United States were more likely to be discontinued than international studies (37.9% vs. 10.5%, P < 0.01). No significant associations were observed between discontinuation and funding source, intervention type, or blinding (all P > 0.05). Nonpublication was not significantly associated with any trial characteristics.
Conclusions
A substantial proportion of TKA clinical trials are discontinued or unpublished, highlighting persistent gaps in transparency. Improving trial design, execution, and result dissemination is essential to reduce research waste and ensure that participant contributions advance evidence-based surgical care.
Keywords: Total knee arthroplasty, research transparency, publication bias, ClinicalTrials.gov, adult reconstruction, randomized controlled trials.
Introduction
Clinical trials are fundamental to advancing modern medicine by evaluating new surgical techniques, treatment strategies, and rehabilitation protocols (1). They generate essential evidence on the safety and effectiveness of interventions that guide clinical practice and future research (1). For this process to be effective, trial results must be publicly reported so the medical community can learn from and build upon prior findings (2). However, despite ongoing efforts to promote transparency, an estimated 30%–50% of clinical trials fail to disseminate their results (3). Premature trial discontinuation and nonpublication represent significant sources of research inefficiency, limiting the translation of valuable data into improved clinical outcomes (4).
Incomplete reporting also raises important ethical concerns. Participants accept potential risks with the expectation that their involvement will contribute to medical knowledge, an expectation undermined when studies are discontinued or results withheld (1). Nonreporting contributes to unnecessary duplication of research, financial waste, and diminished trust in the scientific process (5). When findings remain unavailable, future investigators may unknowingly repeat prior mistakes or overlook known safety concerns, underscoring the importance of reporting all results regardless of outcome (5).
These concerns are particularly relevant in orthopedic surgery, where total knee arthroplasty (TKA) is among the most performed and extensively studied procedures worldwide (6). In the United States, annual TKA volumes are projected to exceed 3.4 million by 2040, driven by an aging population and expanding indications (7). The economic impact is substantial, with hospitalizations and postoperative care exceeding $11 billion annually (8). Given this clinical and financial scale, comprehensive reporting of all TKA-related clinical evidence is essential to inform patient care, device development, and health policy.
U.S. legislation, including the Food and Drug Administration Amendments Act (FDAAA), requires Applicable Clinical Trials (ACTs) to be registered and reported on ClinicalTrials.gov, establishing a legal framework for research transparency (9,10). Despite this, compliance remains inconsistent, and many orthopedic trials are terminated early or never published (11). While knee arthroplasty outcomes have been widely studied, few investigations have systematically evaluated patterns of trial discontinuation and nonpublication in this field. This study addresses this gap by examining these patterns among registered TKA clinical trials, with the goal of informing evidence-based practice and emphasizing the need for stronger accountability in surgical research.
Materials and Methods
Randomized controlled trials (RCTs) related to total knee arthroplasty (TKA) were identified through a systematic search of ClinicalTrials.gov, maintained by the U.S. National Library of Medicine (10). Trials registered between 2013 and 2023 were eligible. To allow adequate time for completion and reporting, only trials registered at least two years before the initial search date (October 5, 2025) were analyzed. Ongoing trials and those without a defined intervention were excluded.
Only Phase 3 and Phase 4 interventional studies were included to focus on trials evaluating clinical efficacy and safety. Trial characteristics were extracted from ClinicalTrials.gov records, including recruitment status, funding source, enrollment size, intervention type, blinding design, number of centers, and recruitment location (10). The search term “knee arthroplasty” was used. Recruitment status was categorized as completed, terminated, withdrawn, or suspended.
Trials not directly related to TKA, non-randomized studies, those completed after October 5, 2023, early-phase trials (Phases 1–2), and pediatric studies were excluded due to their focus on safety and the low prevalence of TKA in pediatric populations (12). Because this study analyzed all eligible total knee arthroplasty trials registered on clinicaltrials.gov during the predefined study period, no formal sample size calculation was performed. The sample size was determined by the number of studies meeting inclusion criteria.
Publication status was determined by reviewing linked publications on ClinicalTrials.gov and by conducting independent searches in PubMed, Embase, and Google Scholar using NCT numbers, investigator names, and trial titles. Publications were considered valid if reported outcomes matched the trial’s design and intervention.
For trials without identified publications, principal investigators were contacted using publicly available contact information. A standardized email inquiry was sent with up to two follow-up attempts at one-week intervals. Investigators were considered unreachable if no response was received. All investigators for this study were unreachable. Trials for which no associated publication could be identified through these methods were classified as unpublished. No statistical imputation of missing data was performed.
Primary outcomes included trial status (completed vs. discontinued, defined as terminated, withdrawn, or suspended) and publication status (published vs. unpublished among completed trials). Associations between outcomes and trial characteristics were analyzed using contingency tables. Statistical significance was set at P < 0.05, with chi-square tests used for categorical comparisons and Fisher’s exact or Fisher–Freeman–Halton tests applied when appropriate. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Statistical analysis was performed in R version 4.3.2.
To minimize bias, predefined inclusion and exclusion criteria were applied consistently, and publication status was independently verified by two reviewers. Given the observational, registry-based design, no multivariable adjustment for confounding was performed; however, key trial characteristics were compared to assess their association with study outcomes.
Results
Our initial search identified 174 registered knee arthroplasty clinical trials from 2013 to 2023. One trial was excluded during screening because it was unrelated to total knee arthroplasty, leaving 173 trials that met the inclusion and exclusion criteria for final analysis (Figure 1). These trials collectively enrolled approximately 17,300 participants across 24 countries, with the United States accounting for 88 trials (50.6%). Among international studies, Denmark (22), China (11), and Canada (9) represented the most frequent sites of trial activity.
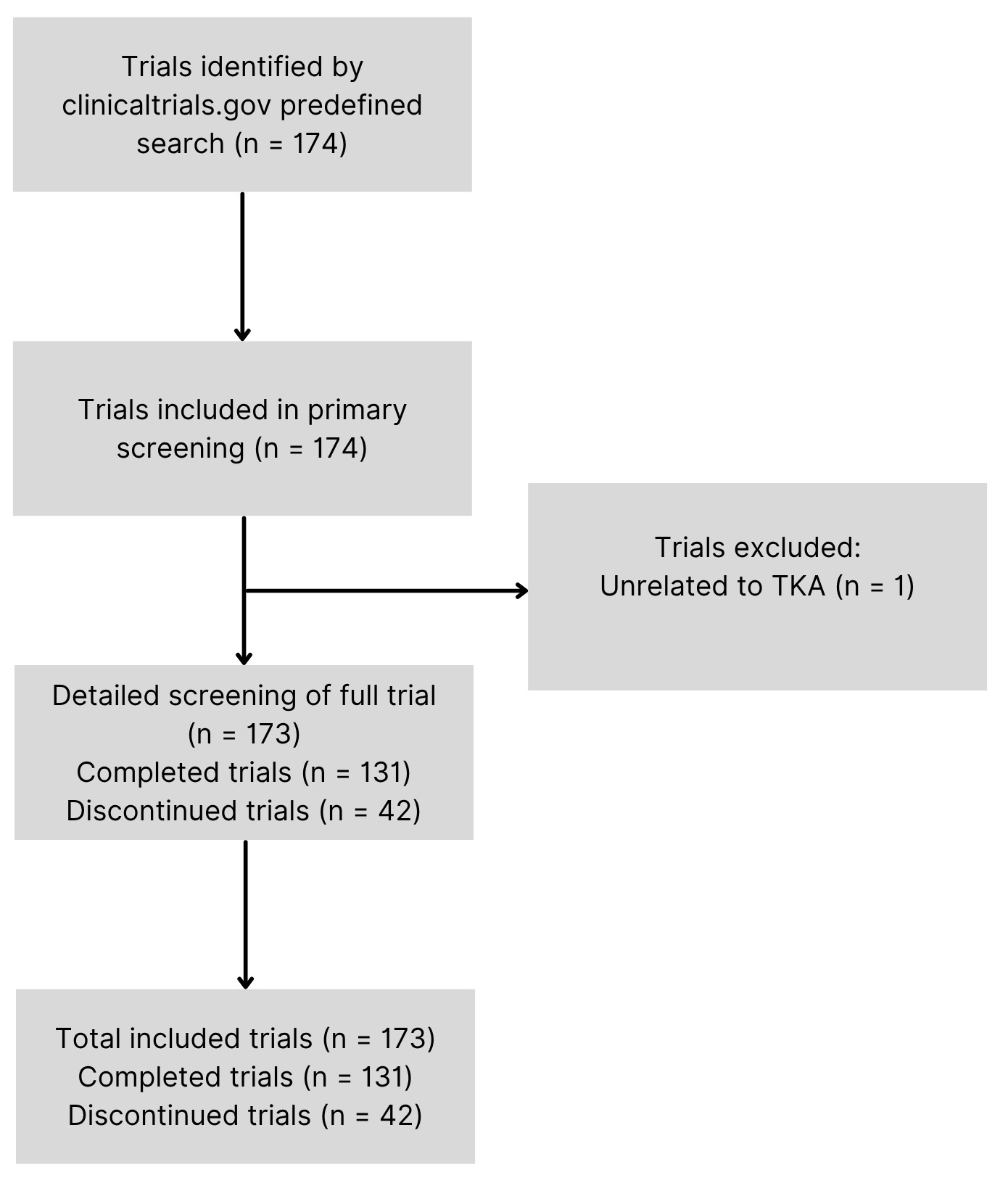
Of the 173 registered knee arthroplasty clinical trials analyzed, 131 (75.7%) were completed and 42 (24.3%) were discontinued (Figure 1, Table 1). Approximately 17,300 participants were enrolled across all included trials (mean = 100 individuals, range 0–1,089), with 16,202 (93.7%) taking part in completed trials and 1,098 (6.3%) in discontinued trials. No statistically significant association was found between trial completion status and funding source (industry vs. non-industry, p = 0.60), intervention type (p=0.34), or blinding method (p=0.25). Single-center trials were more likely to be discontinued than multi-center trials (27.0% [CI: 20.5 – 34.5] vs 4.8% [CI: 0.8 – 22.7] respectively; OR 7.4, P < 0.05, Table 1). Trials with enrollment less than 100 were more likely to be discontinued than those with enrollment greater than 100 (33.6% [CI: 25.7 – 42.6] vs 5.3% [CI: 1.8 – 14.5] respectively; OR 9.1, P < 0.05, Table 1). Trials conducted exclusively in the United States were more likely to be discontinued than those with international participant recruitment (37.9% [CI: 28.5 – 48.4] vs 10.5% [CI: 5.6 – 18.7] respectively; OR 5.2, P < 0.01, Table 1).
| Characteristic | Discontinued (n=42) | Completed (n=131) | Total (173) | Discontinuation Rate | 95% CI | P-Value |
| Non-Industry | 37 | 119 | 156 | 23.7% | 17.7 – 31.0% | 0.60 |
| Industry | 5 | 12 | 17 | 29.4% | 13.3 – 53.1% | |
| Behavioral | 1 | 1 | 2 | 50.0% | 9.5 – 90.5% | 0.34 |
| Biological | 1 | 1 | 2 | 50.0% | 9.5 – 90.5% | |
| Device | 6 | 8 | 14 | 42.9% | 21.4 – 67.4% | |
| Dietary Supplement | 0 | 1 | 1 | 100.0% | 0.0 – 79.3% | |
| Drug | 40 | 124 | 164 | 24.4% | 18.5 – 31.5% | |
| Procedure | 3 | 14 | 17 | 17.6% | 6.2 – 41.0% | |
| Other | 4 | 6 | 10 | 40.0% | 16.8 – 68.7% | |
| Single Center | 41 | 111 | 152 | 27.0% | 20.5 – 34.5% | < 0.05 |
| Multi Center | 1 | 20 | 21 | 4.8% | 0.8 – 22.7% | |
| <100 | 39 | 77 | 116 | 33.6% | 25.7 – 42.6% | < 0.05 |
| >100 | 3 | 54 | 57 | 5.3% | 1.8 – 14.4% | |
| US | 33 | 54 | 87 | 37.9% | 28.5 – 48.4% | < 0.01 |
| International | 9 | 77 | 86 | 10.5% | 5.6 – 18.7% | |
| None | 7 | 24 | 31 | 22.6% | 11.4 – 39.8% | 0.25 |
| Single | 10 | 14 | 24 | 41.7% | 24.5 – 61.2% | |
| Double | 10 | 28 | 38 | 26.3% | 15.0 – 42.0% | |
| Triple | 5 | 22 | 27 | 18.5% | 8.2 – 36.7% | |
| Quadruple | 10 | 43 | 53 | 18.9% | 10.6 – 31.4% | |
Table 1. Characteristics of registered randomized controlled trials investigating therapies for Knee Arthroplasty, 2013-2023, by completion status
Of the 131 completed knee arthroplasty clinical trials, 100 studies (76.3%) were published, while 31 (23.7%) remained unpublished (Table 2). Among unpublished studies, a total of 2,813 participants were enrolled in completed trials whose results have not been disseminated. No statistically significant associations were observed between publication status and funding source, number of centers, enrollment size, intervention type, recruitment region, or blinding method (all P > 0.05, Table 2).
| Characteristic | Published (n=100) | Unpublished (n=31) | Total (131) | Nonpublication Rate | 95% CI | P-Value |
| Non-Industry | 93 | 26 | 119 | 21.8% | 15.4 – 30.1% | 0.12 |
| Industry | 7 | 5 | 12 | 41.7% | 19.3 – 68.0% | |
| Behavioral | 0 | 1 | 1 | 100.0% | 20.7 – 100.0% | 0.15 |
| Biological | 0 | 1 | 1 | 100.0% | 20.7 – 100.0% | |
| Device | 7 | 1 | 8 | 12.5% | 2.2 – 47.1% | |
| Dietary Supplement | 0 | 1 | 1 | 100.0% | 20.7 – 100.0% | |
| Drug | 94 | 30 | 124 | 24.2% | 17.5 – 32.4% | |
| Procedure | 11 | 3 | 14 | 21.4% | 7.6 – 47.6% | |
| Other | 5 | 1 | 6 | 16.7% | 3.0 – 56.4% | |
| Single Center | 84 | 27 | 111 | 24.3% | 17.3 – 33.1% | 0.78 |
| Multi Center | 16 | 4 | 20 | 20.0% | 8.1 – 41.6% | |
| <100 | 55 | 22 | 77 | 28.6% | 19.7 – 39.5% | 0.12 |
| >100 | 45 | 9 | 54 | 16.7% | 9.0 – 28.7% | |
| US | 38 | 16 | 54 | 29.6% | 19.1 – 42.8% | 0.18 |
| International | 62 | 15 | 77 | 19.5% | 12.2 – 29.7% | |
| None | 15 | 9 | 24 | 37.5% | 21.2 – 57.3% | 0.43 |
| Single | 12 | 2 | 14 | 14.3% | 4.0 – 39.9% | |
| Double | 21 | 7 | 28 | 25.0% | 12.7 – 43.4% | |
| Triple | 18 | 4 | 22 | 18.2% | 7.3 – 38.5% | |
| Quadruple | 34 | 9 | 43 | 20.9% | 11.4 – 35.2% | |
Table 2. Characteristics of completed randomized controlled trials investigating therapies for Knee Arthroplasty, 2013-2023, by publication status.
Discussion
A substantial proportion of registered knee arthroplasty clinical trials were either discontinued or remained unpublished despite completion. In our analysis, 24.3% of trials were discontinued, representing data from 1,098 participants that were never made publicly available. Additionally, 23.7% of completed trials remained unpublished, accounting for 2,813 participants whose results were not disseminated. This loss of data limits transparency and weakens the evidence base guiding total knee arthroplasty (TKA) practice. These findings align with prior surgical research reporting discontinuation rates of 20–25% and nonpublication rates exceeding 30% (13,14).
These patterns raise significant ethical and scientific concerns. Trial participants assume risk with the expectation that their involvement will advance medical knowledge, an obligation undermined when studies are discontinued or unpublished (15). The selective dissemination of positive findings further contributes to publication bias, distorting assessments of treatment efficacy and potentially influencing clinical decision-making in orthopedic care (16,17).
The lack of publicly available TKA trial data also affects innovation and guideline development. Incomplete reporting may lead to prosthesis refinement based on selectively positive evidence, unrecognized complications, or premature adoption of surgical techniques and perioperative protocols (17,18). Clinical guidelines built on incomplete data risk reflecting publication bias rather than true clinical outcomes (19). Strengthening transparency through stricter enforcement of result reporting, funding-contingent publication requirements, and registry audits may improve accountability and ensure evidence-based advancement in TKA care.
Trial design characteristics were associated with discontinuation risk. Single-center studies were discontinued more frequently than multicenter trials (27.0% vs. 4.8%, P < 0.05), consistent with evidence that collaborative frameworks improve recruitment and resource stability (20). Smaller trials (<100 participants) were also discontinued at higher rates than larger studies (33.6% vs. 5.3%, P < 0.05), reinforcing the role of inadequate recruitment as a major driver of trial failure. U.S.-based studies were significantly more likely to be discontinued than international trials (37.9% vs. 10.5%, P < 0.01), potentially reflecting stricter regulatory requirements, limited funding, and increased competition for participants (21).
Among completed trials, 23.7% remained unpublished, a rate consistent with nonpublication estimates across medical specialties (13,14). Unlike some prior studies, we found no significant associations between publication status and funding source, enrollment size, intervention type, study design, recruitment region, or blinding. This suggests that barriers to publication in TKA research may be systemic rather than attributable to specific trial characteristics. Regardless of cause, nonpublication undermines transparency, slows scientific progress, and risks unnecessary duplication of research (15–17).
Despite established requirements for trial registration and result reporting, many TKA trials failed to update registry records or disseminate findings. Incomplete reporting on ClinicalTrials.gov limits insight into reasons for trial failure or nonpublication, reflecting broader transparency challenges seen across medical research (21). This study relied on ClinicalTrials.gov, which may not capture all global TKA research, as some trials may be registered elsewhere or not registered publicly. Additionally, variability in terminology may have resulted in the exclusion of relevant studies.
Future research should incorporate direct investigator feedback through surveys or interviews to better identify logistical, financial, and administrative barriers to trial completion and publication. Expanding analyses to include international registries and examining journal submission patterns may further clarify the mechanisms driving trial discontinuation and nonpublication.
Conclusion
Our study highlights the need for continued improvement to reduce the number of discontinued and unpublished clinical trials in knee arthroplasty. Comprehensive reporting of trial outcomes is essential to support evidence-based surgical care and improve patient outcomes. When studies are stopped early or remain unpublished, valuable data and resources are lost, and the efforts of participants may not contribute to advancing clinical knowledge. Greater commitment from researchers, sponsors, and institutions is needed to enhance trial design, conduct, and transparency, thereby reducing research waste and strengthening the evidence base for knee arthroplasty.
Ethics & Declarations
This study used publicly available, de-identified data from ClinicalTrials.gov; therefore, individual consent to participate was not required. Because the analysis relied solely on publicly accessible registry data and did not involve human subjects research as defined by federal guidelines, institutional review board (IRB) approval was not required. Human Ethics and Consent to Participate declarations: not applicable. All data analyzed in this study are publicly accessible through ClinicalTrials.gov and are included within this manuscript and its supplementary materials. The authors declare no competing interests.
Funding
No funding was received for this work.
References
- Kandi V, Vadakedath S. Clinical Trials and Clinical Research: A Comprehensive Review. Cureus. 2023 Feb 16;15(2):e35077. doi: 10.7759/cureus.35077. PMID: 36938261; PMCID: PMC10023071.
- Morrow RL, Mintzes B, Gray G, Law MR, Garrison S, Dormuth CR. Public reporting of clinical trial findings as an ethical responsibility to participants: a qualitative study. BMJ Open. 2023 Mar 21;13(3):e068221. doi: 10.1136/bmjopen-2022-068221. PMID: 36944466; PMCID: PMC10032397.
- Ross JS, Mocanu M, Lampropulos JF, Tse T, Krumholz HM. Time to publication among completed clinical trials. JAMA Intern Med. 2013 May 13;173(9):825-8. doi: 10.1001/jamainternmed.2013.136. PMID: 23460252; PMCID: PMC3691813.
- Pica N, Bourgeois F. Discontinuation and Nonpublication of Randomized Clinical Trials Conducted in Children. Pediatrics. 2016 Sep;138(3):e20160223. doi: 10.1542/peds.2016-0223. Epub 2016 Aug 4. PMID: 27492817; PMCID: PMC5005019.
- Moher D, Glasziou P, Chalmers I, Nasser M, Bossuyt PMM, Korevaar DA, Graham ID, Ravaud P, Boutron I. Increasing value and reducing waste in biomedical research: who’s listening? Lancet. 2016 Apr 9;387(10027):1573-1586. doi: 10.1016/S0140-6736(15)00307-4. Epub 2015 Sep 27. PMID: 26423180.
- Gao J, Xing D, Dong S, Lin J. The primary total knee arthroplasty: a global analysis. J Orthop Surg Res. 2020 May 26;15(1):190. doi: 10.1186/s13018-020-01707-5. PMID: 32456654; PMCID: PMC7249396.
- Singh JA, Yu S, Chen L, Cleveland JD. Rates of Total Joint Replacement in the United States: Future Projections to 2020-2040 Using the National Inpatient Sample. J Rheumatol. 2019 Sep;46(9):1134-1140. doi: 10.3899/jrheum.170990. Epub 2019 Apr 15. PMID: 30988126.
- Losina E, Walensky RP, Kessler CL, Emrani PS, Reichmann WM, Wright EA, Holt HL, Solomon DH, Yelin E, Paltiel AD, Katz JN. Cost-effectiveness of total knee arthroplasty in the United States: patient risk and hospital volume. Arch Intern Med. 2009 Jun 22;169(12):1113-21; discussion 1121-2. doi: 10.1001/archinternmed.2009.136. PMID: 19546411; PMCID: PMC2731300.
- Department of Health and Human Services. The Final Rule. https://www.cms.gov/OpenPayments/Downloads/Affordable-Care-Act-Section-6002-Final-Rule.pdf. Accessed November 9, 2024.
- ClinicalTrials.gov. (2018, June 27). Checklist for Evaluating Whether a Clinical Trial or Study is an Applicable Clinical Trial (ACT) Under 42 CFR 11.22(b) for Clinical Trials Initiated on or After January 18, 2017. https://cdn.clinicaltrials.gov/documents/ACT_Checklist.pdf
- Singh G, Wague A, Arora A, Rao V, Ward D, Barry J. Discontinuation and nonpublication of clinical trials in orthopaedic oncology. J Orthop Surg Res. 2024 Feb 5;19(1):121. doi: 10.1186/s13018-024-04601-6. PMID: 38317223; PMCID: PMC10845780.
- Martin JR, Sutak AK, Milbrandt TA, Martin VA, Trousdale RT. Adolescent total knee arthroplasty. Arthroplast Today. 2017 Feb 13;3(2):105-109. doi: 10.1016/j.artd.2016.04.002. PMID: 28695182; PMCID: PMC5484984.
- Chapman SJ, Shelton B, Mahmood H, Fitzgerald JE, Harrison EM, Bhangu A. Discontinuation and non-publication of surgical randomised controlled trials: observational study. BMJ. 2014 Dec 9;349:g6870. doi: 10.1136/bmj.g6870. PMID: 25491195; PMCID: PMC4260649.
- Shepard S, Anderson JM, Heigle B, Thompson JC, Detweiler B, Hartwell M, Vassar M. Rates of discontinuation and non-publication of upper and lower extremity fracture clinical trials. J Orthop Surg Res. 2023 Mar 29;18(1):256. doi: 10.1186/s13018-023-03698-5. PMID: 36991514; PMCID: PMC10053675.
- Morrow RL, Mintzes B, Gray G, Law MR, Garrison S, Dormuth CR. Public reporting of clinical trial findings as an ethical responsibility to participants: a qualitative study. BMJ Open. 2023 Mar 21;13(3):e068221. doi: 10.1136/bmjopen-2022-068221. PMID: 36944466; PMCID: PMC10032397.
- Joober R, Schmitz N, Annable L, Boksa P. Publication bias: what are the challenges and can they be overcome? J Psychiatry Neurosci. 2012 May;37(3):149-52. doi: 10.1503/jpn.120065. PMID: 22515987; PMCID: PMC3341407.
- Schulz R, Langen G, Prill R, Cassel M, Weissgerber TL. Reporting and transparent research practices in sports medicine and orthopaedic clinical trials: a meta-research study. BMJ Open. 2022 Aug 8;12(8):e059347. doi: 10.1136/bmjopen-2021-059347. PMID: 35940834; PMCID: PMC9364413.
- Kulkarni PG, Paudel N, Magar S, Santilli MF, Kashyap S, Baranwal AK, Zamboni P, Vasavada P, Katiyar A, Singh AV. Overcoming Challenges and Innovations in Orthopedic Prosthesis Design: An Interdisciplinary Perspective. Biomed Mater Devices. 2023 May 12:1-12. doi: 10.1007/s44174-023-00087-8. Epub ahead of print. PMID: 37363137; PMCID: PMC10180679.
- Humphreys BL. New requirements for clinical trial transparency provide new opportunities for informatics research. J Am Med Inform Assoc. 2019 Jun 1;26(6):493-494. doi: 10.1093/jamia/ocz047. PMID: 31087069; PMCID: PMC7647345.
- Barnard KD, Dent L, Cook A. A systematic review of models to predict recruitment to multicentre clinical trials. BMC Med Res Methodol. 2010 Jul 6;10:63. doi: 10.1186/1471-2288-10-63. PMID: 20604946; PMCID: PMC2908107.
- George E, Baker McDowell A, Vozza M, Mitchell T, Quartley B, Kennedy CS, Hanlon B. Regulatory landscape with U.S. patient requirements and Clinical Trial Diversity expectations. Contemp Clin Trials Commun. 2024 Jul 6;42:101331. doi: 10.1016/j.conctc.2024.101331. PMID: 39314996; PMCID: PMC11417185.
