
Jennifer A. Kipp DPM1, William H. Fang DO2, Evan Dunn DO2, Mitchell Tingey MD2, Troy Watson MD1,2
1Desert Orthopaedic Center, Las Vegas NV
1Valley Hospital Medical Center, Department of Orthopaedics, Las Vegas NV
DOI: http://doi.org/10.70709/yhj5qlgpvop512
Abstract
Background
Navicular stress fractures are uncommon but clinically significant injuries that occur in adolescent, adult, and elite athlete populations exposed to repetitive loading. Due to the navicular bone’s limited vascularity, these fractures are at increased risk of delayed union, nonunion, and refracture. Treatment includes both operative and nonoperative fixation, with management guided by patient-specific factors.
Methods
A comprehensive narrative review was conducted using PubMed and Google Scholar online databases. These databases were searched for studies published between 2000 and 2026 that evaluated operative or nonoperative treatment of navicular stress fractures. Ten primary clinical studies met inclusion criteria and were synthesized.
Results
Operative fixation demonstrated union rates from 80-100% with reliable return-to-sport timelines in adult and athletic populations. Elite athletes treated with vascularized bone grafting achieved 100% fracture union and 94% return to sport. Nonoperative management demonstrated favorable outcomes in adolescent populations, with high success and median return-to-sport of 5 months. Conservative management demonstrated greater variability in adult and complete fracture cohorts with up to 11% refracture rates.
Conclusion
Both operative and nonoperative treatment strategies can achieve favorable outcomes tailored to fracture completeness and patient population. Operative fixation provides more predictable healing in complete fractures and high-demand athletes, while nonoperative treatment remains effective in adolescents and incomplete fractures. CT staging plays a critical role in treatment selection.
Keywords: Navicular stress fracture, treatment, operative fixation, nonoperative, athletes, return to sport
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Introduction
Navicular stress fractures are relatively uncommon but clinically significant injuries, particularly in adolescents and athletes who engage in high-volume running, jumping and impact sports. These fractures are also observed in the recreational athlete and nonathletic adult populations exposed to repetitive loading(1-3). The navicular bone plays a critical biomechanical role in force transmission through the medial longitudinal arch, articulating with the talus proximally and three cuneiforms distally. This central position subjects the navicular to significant compressive and shear forces during gait, particularly during push-off phase when forces re transmitted from the hindfoot to the forefoot(4).
The central third of the navicular bone is relatively hypovascular compared with its medial and lateral aspects, creating a watershed region that is vulnerable to stress injury and impaired healing(2,5). This limited vascular supply contributes to increased risk of delayed union, nonunion, and refracture, compared with other stress fracture locations. As a result, navicular stress fractures are often considered high-risk stress injuries that may warrant closer monitoring and, in some cases, more aggressive management than lower-risk sites.
Computed tomography (CT) plays an important role in diagnosis and classification of navicular stress fractures, complementing the sensitivity of magnetic resonance imaging (MRI) for early bone stress. The CT-based classification system described by Saxena et al. is used to stage navicular stress fractures and guide treatment decisions(1). This classification divides navicular stress fractures into three stages based on fracture completeness and displacement: type I fractures are incomplete and confined to the dorsal cortex; type II fractures are complete, extending from the dorsal cortex into the central navicular body without displacement; type III fractures are complete fractures that extend through dorsal and plantar cortices and may demonstrate displacement, sclerosis, or chronic nonunion. Higher grade fractures, particularly type III, demonstrate increased risk of delayed union and nonunion due to fracture instability and impaired vascularity(1,5).
Patients typically present with insidious onset of dorsal midfoot pain exacerbated by activity and relieved with rest. Plain radiographs may be negative in early injury stages, so advanced imaging is often used. Magnetic resonance imaging (MRI) is sensitive for early stress reactions and bone marrow edema, while CT provides superior characterization of the fracture morphology, completeness, and chronicity, and is widely used for both diagnosis and union assessment(2,3).
Treatment strategies include nonoperative immobilization and operative fixation. Historically, nonoperative treatment was considered standard for incomplete fractures, while operative fixation has gained increasing support for complete and chronic fractures, particularly in competitive and elite athletes who require reliable healing to facilitate returning to sport. (3,6-10).
The purpose of this comprehensive narrative review is to evaluate clinical outcomes of the operative and nonoperative management of navicular stress fractures across adolescent, adult, and elite athlete populations, with emphasis on fracture stage and patient-specific factors. Primary studies are the focus of the analysis, while systematic reviews and meta-analyses are discussed separately to contextualize higher-level evidence.
Materials and Methods
This comprehensive narrative review focuses on clinical outcomes following operative and nonoperative management of navicular stress fractures in the foot among adolescents, adults, and elite athletes. The goal of this review is to provide a clinically relevant overview of the available literature without conducting a formal analysis, supplemented by systematic reviews and meta-analyses for broader context.
The PubMed and Google Scholar databases were accessed on January 8th, 2026, to perform a targeted literature search. These databases were selected based on their extensive coverage of peer-review articles from 2000-2026. Search terms included: “navicular stress fracture,” “navicular bone stress injury,” “operative management navicular stress fracture,” “conservative treatment navicular stress fracture,” “return to sport navicular stress fracture,” “adolescent navicular stress fracture,” and “elite athlete navicular stress fracture.” The first 200 results per search were screened to manage the large result set. Reference lists of key articles and systematic reviews were also reviewed to identify additional eligible articles.
Inclusion criteria for the primary synthesis were human studies published between 2000-2026 with a focus on tarsal navicular stress fractures confirmed via CT and/or MRI; reporting on operative or nonoperative treatment; clinical outcomes including healing, time to return to sport, refracture, nonunion, or complications; and study designs including randomized trials, prospective or retrospective cohorts, comparative studies, and case series greater than or equal to 10 cases. Studies reporting tarsal navicular stress injuries without a defined cortical fracture line were excluded unless that fracture was later confirmed on advanced imaging.
Systematic reviews and meta-analyses identified during the search were not included in the formal synthesis but were included in the discussion. Exclusion criteria included nonhuman studies, acute traumatic navicular fractures or avulsion fractures, non-English publications, and duplicate cohorts.
The study screening and selection process was performed by a single author. Titles and abstracts were reviewed for relevance, followed by full-text review of potentially eligible studies. Articles were selected based on predefined criteria including relevance to navicular stress fracture treatment, clarity of reported outcomes, and study design. As this was a narrative review, formal consensus review and risk-of-bias analysis scoring were not performed.
Adolescents are defined in this review as skeletally immature patients less than 18 years of age or having been described as “pediatric” or “adolescent.” Adults are defined as skeletally mature patients greater than 18 years of age. Professional athletes, collegiate athletes or study-defined elite cohorts are defined as “elite athletes.”
Data charting forms were constructed to extract and organize key information from studies included in this review. Extraction fields included: author, study design, sample size, population (adolescent/adult/mixed), athlete level, imaging modality to confirm diagnosis, treatment type, follow-up duration, outcomes (union, return to sport rate, time to return, complications, reinjury). No assumptions were made beyond data explicitly reported in the included articles. Given the heterogeneity in study designs, outcomes, and treatment protocols, a qualitative narrative synthesis was performed rather than a pooled quantitative meta-analysis. Findings were organized by adolescents, adults, and elite athletes.
Results
A total of 225 studies were identified through the PubMed and Google Scholar databases. After initial screening of titles and abstracts, 38 remained. Following full-text review, 10 studies were ultimately included in the final synthesis (Figure 1).
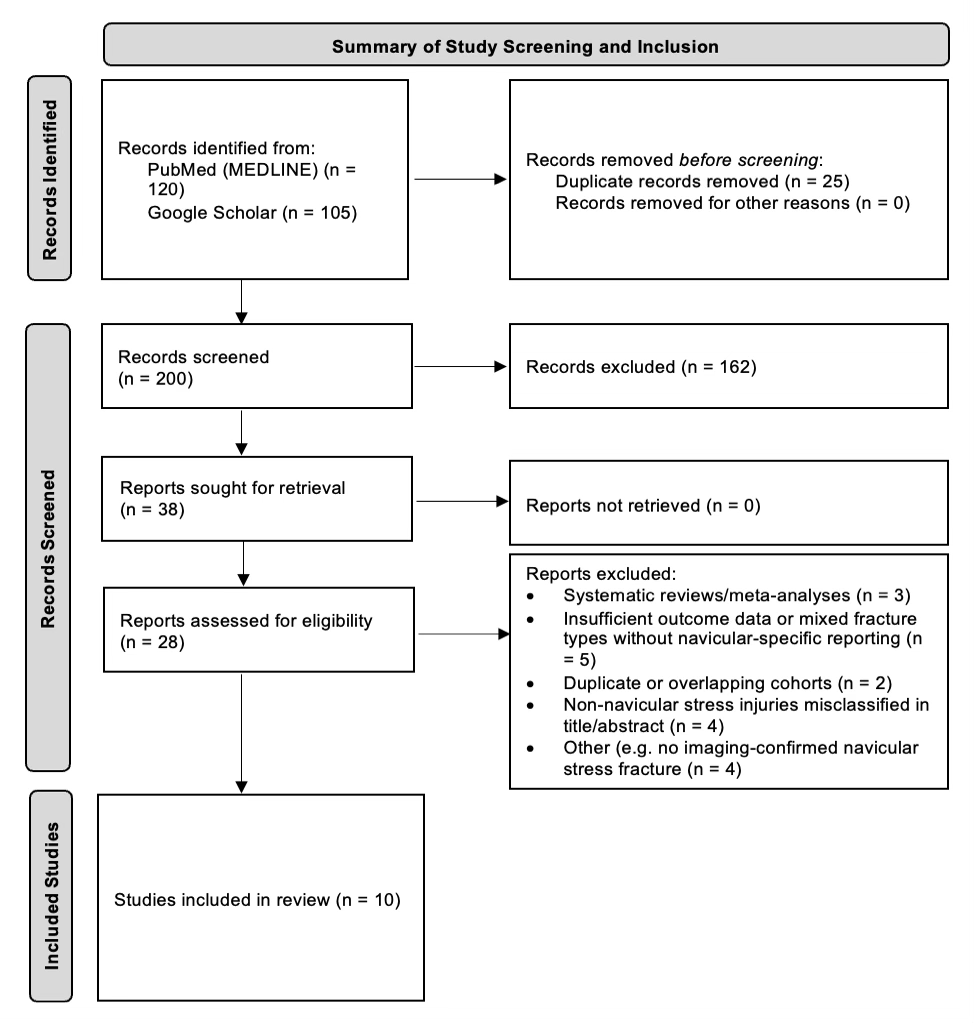
These 10 studies included adult mixed populations, competitive and elite athletes, and adolescent cohorts. Follow-up durations ranged from 18-48 months. CT was used in all cohorts, and MRI was used adjunctively in several studies to characterize early stress injury or confirm fracture presence(1-10)(Table 1).
| Author (Year) | Study Design | Sample Size | Population | Athlete Level | Imaging | Treatment | Follow-up |
| Saxena & Fullem (2000)(1) | Retrospective cohort | 22 fractures | Adults | Mixed | Radiographs, CT | Operative and nonoperative | 36 months |
| Burne et al (2005)(2) | Retrospective cohort | 55 patients | Adults | Mixed | CT, MRI | Nonoperative | 36 months |
| Potter et al (2006)(3) | Retrospective cohort | 32 fractures | Adults | Mixed | CT, MRI | Operative and nonoperative | 24 months |
| Saxena et al (2006)(4) | Prospective cohort | 20 fractures | Adults | Athletes | CT | Operative and nonoperative | 24 months |
| McCormick et al (2011)(5) | Retrospective cohort | 28 patients | Adults | Athletes | CT | Operative and nonoperative | 26 months |
| Jacob et al (2013)(6) | Retrospective cohort | 10 fractures | Adults | Mixed | CT | Operative fixation | 18 months |
| Saxena et al (2017)(7) | Prospective cohort | 62 fractures | Mixed | Mixed (professional, collegiate, recreational) | CT | Operative and nonoperative | 48 months |
| Nunley et al (2022)(8) | Retrospective cohort | 43 fractures | Adults | Mixed | CT | Operative fixation ± graft | 12+ months |
| Mehta et al (2023)(9) | Multicenter cohort | 110 patients | Adolescents (10-19 years) | Mixed (high school, collegiate) | MRI, CT | Operative and nonoperative | 18 months |
| Hong et al (2026)(10) | Retrospective cohort | 17 fractures | Adults | Elite athletes | CT | Operative vascularized graft | 42 months |
Table 1. Characteristics of Included Primary Clinical Outcome Studies (2000–2026).
This table demonstrates the study characteristics that were included in the primary review.
Abbreviations: CT, computed tomography, MRI, magnetic resonance imaging
Adult and Mixed Population Cohorts
Adult and mixed-population cohorts comprised most of the included studies and demonstrated consistently favorable outcomes following operative fixation.Saxena and Fullem evaluated 22 navicular stress fractures in adult athletes and active individuals treated with operative and nonoperative approaches(1). Operatively treated fractures achieved 100% union, and mean time to activity was shorter in the operative group (3.1 ± 1.2 months) compared to the conservative group (4.3 ± 2.8 months)(p = 0.02). Two refractures occurred in the conservative group during treatment. Authors recommend surgery for type II and type III stress fractures (Table 2).
| Author (Year) | Population | Operative Technique | Return to Sport/Activity | Time to Return | Complications |
| Saxena & Fullem (2000)(1) | Adults | Screw fixation | 100% | ~4 months | Hardware removal reported |
| Potter et al (2006)(3) | Adults | Screw fixation | 100% | ~5 months | Mild residual pain |
| McCormick et al (2011)(5) | Adult | Screw fixation | ~80% | 2.7 months to shoes, no specification on sport | Nonunion (n=2) |
| Jacob et al (2013)(6) | Adults | Percutaneous screw fixation | ~80% | ~4–5 months | Nonunion (n=2), residual pain (n=2) |
| Saxena et al (2017)(7) | Athletes | Screw fixation | 91.9% | 4.56 months | 11% screw removal |
| Nunley et al (2022)(8) | Adults | ORIF ± non vascularized or vascularized bone graft | No difference among cohorts (no precise percentage reported) | No difference among cohorts | Minimal |
| Mehta et al (2023)(9) | Adolescents | Single or double screw | Majority returned (no precise percentage reported) | Median 5 months | Delayed union (n=1), nonunion (n=1), implant removal (n=1) |
| Hong et al (2026)(10) | Elite athletes | Vascularized bone graft | 94% | 4 months return to training; 94% return to pre-injury level | Persistent pain & development of arthritis (n=1) |
Table 2. Operative Treatment Outcomes.
This table highlights the outcomes in patients who were treated operatively for navicular stress fractures.
Abbreviations: ORIF, open reduction internal fixation
Burne et al evaluated long-term outcomes of navicular stress injuries managed nonoperatively using immobilization protocols(2). While incomplete fractures generally healed successfully, outcomes are variable in complete fractures, and some patients experienced persistent symptoms or limitations in return to sport (Table 3). Imaging findings did not consistently correlate with clinical outcomes at long term follow-up, emphasizing the importance of clinical evaluation in guiding treatment decisions (2).
| Author (Year) | Population | Nonoperative Protocol | Return to Sport/Activity | Time to Return | Complications |
| Burne et al (2005)(2) | Adults | Casting, non-weightbearing | 55% | 4–6 months | Delayed union possible |
| Potter et al (2006)(3) | Adults | Casting | 100% | Slower than operative | Nonunion risk, residual pain over dorsal navicular |
| Saxena et al (2006)(4) | Adults | Casting | 94% | 4–6 months | Delayed union possible |
| Saxena et al (2017)(7) | Mixed | Casting | 91.9% | 3.97 months | 11.2% refractures |
| Mehta et al (2023)(9) | Adolescents | Protected weightbearing in a boot or cast | 94% | Shorter in nonoperative group when compared to operative (p<0.05) | Delayed union (n=1), nonunion (n=1), implant removal (n=1) |
Table 3. Nonoperative Treatment Outcomes.
This table highlights the outcomes in patients who were treated nonoperatively for navicular stress fractures.
Potter et al evaluated both operative and nonoperative management strategies and reported that operatively treated fractures demonstrated reliable union and return to activity (Tables 1-3)(3). Although long-term outcomes were generally favorable in both groups, conservatively managed fractures demonstrated slower recovery and increased variability in healing timelines. Residual pain was noted over the dorsal navicular “N” spot in both treatment cohorts, possibly attributable to hardware irritation in some surgically treated patients. Authors note that tenderness may remain over the “N” spot in a percentage of patients long-term(3).
McCormick et al evaluated 10 navicular stress fractures in adult patients and reported union rates of 80% following operative fixation, as verified by CT(5). Operatively treated patients reported significant improvements in outcomes with higher AOFAS and SF-36 scores as compared to two patients with nonunions. Complete and displaced fractures were both more likely to progress to nonunion (Table 2)(5).
Jacob et al evaluated minimally invasive operative fixation in 10 navicular stress fractures and reported 80% fracture union (Table 2)(6). Most patients returned to their pre-injury level of sports activity within 4-5 months with minimal complications. A long-term review with an average duration of 7-years post-procedure follow up showed that 6 of the 8 patients who responded were still symptom free, and 2 of the patients had intermittent pain after prolonged activity(6).
Saxena et al (2017) evaluated 62 navicular stress fractures in adult mixed-level athletes(7). 91.9% of patients treated operatively returned to their previous level of activity. Mean time to return to sport was 4.56 months in the operatively treated cohort, and 3.97 months in the nonoperatively treated cohort. Screw removal occurred in 11% of operatively treated patients, and 11% of nonoperatively treated patients refractured(Tables 2&3)(7).
Nunley et al evaluated 43 navicular stress fractures treated using an algorithmic operative approach, including open reduction and internal fixation (ORIF) alone, ORIF with non-vascularized bone grafting, and ORIF with vascularized bone grafting depending on fracture characteristics (Table 2)(8). There was a 100% union rate in navicular stress fractures treated with ORIF and vascularized bone grafting, and a 75% union rate in those with ORIF and non-vascularized bone grafting. Functional outcomes improved following operative fixation, and complications were minimal. These findings support biologically augmented fixation strategies in chronic or high-risk fractures(8).
Elite Athlete Cohorts
Elite athlete populations demonstrated excellent outcomes following operative fixation, particularly in chronic or nonunion cases. Hong et al evaluated 17 elite athletes with chronic navicular stress fracture nonunions treated with vascularized pedicle bone grafting (Table 2)(10). All fractures achieved radiographic union, representing a 100% union rate. Sixteen of 17 athletes (94%) returned to their preinjury level of sport. Mean return to training was approximately 16 weeks(10). These findings ultimately highlight the effectiveness of vascularized bone grafts in elite athletes with chronic fracture nonunion and support operative fixation in high-demand populations.
Adolescent Cohorts
Adolescent navicular stress fractures demonstrated favorable outcomes with nonoperative treatment. Mehta et al evaluated 110 adolescent navicular stress injuries in a multicenter cohort(Tables 2&3)(9). Nonoperative treatment was successful with most patients returning to sport following immobilization in a boot or cast and activity modification. Median return-to-sport time was approximately 5 months. Operative treatment was required in 15% of patients, most commonly in older adolescents, those with a higher body mass index, and those with more severe stress fractures. Median time to return to weightbearing, running, and full sport was longer for the operative group than the nonoperative group (p <.05). Surgical complications were uncommon and included one delayed union, one nonunion, and one painful implant that was ultimately removed(9).
Overall, navicular stress fracture treatment outcomes varied by patient population and fracture severity (Table 4). In 4 of 5 studies, nonoperative treatment resulted in >90% return to sport among adolescents and patients with incomplete fractures(3,4,7,9). However, one study reported only a 55% return-to-sport rate after nonoperative management in this same patient population(2).Operative fixation provided more reliable healing in adult and athletic populations, especially among those with complete fractures and chronic injuries.
| Population | Preferred treatment | Union rate | Return to sport | Advantages | Disadvantages |
| Adolescents | Nonoperative first-line | ~55-100% | ~4–6 months | Avoids surgery; satisfactory healing potential | Longer immobilization period |
| Adult non-elite | Operative for complete fractures; nonoperative for incomplete | ~95–100% operative | ~4–6 months | Predictable healing; structural stability | Operative risks; hardware-related complications |
| Athletes | Often operative for complete fractures | ~95–100% | ~4–5 months | Reliable healing; predictable return to sport | Operative risks; hardware-related complications |
| Elite athletes/chronic nonunion | Operative with biologic augmentation (ex. vascularized bone graft) | ~100% | ~3–4 months | High union rates in high-demand population | Surgical complexity – specialized techniques required |
Table 4. Summary of Treatment Outcomes by Population and Treatment Type.
This table summarizes overall treatment outcomes by patient population type.
Discussion
This comprehensive narrative review demonstrates that navicular stress fractures can be successfully managed using operative and nonoperative treatment strategies when individualized based on fracture characteristics and patient-specific factors. Across the included studies, operative fixation demonstrated high union rates, predictable return-to-sport timelines, and low complication rates, particularly in adult and athletic populations (1,3,8-10). In contrast, nonoperative management demonstrated satisfactory outcomes in incomplete fractures and adolescent populations but was associated with variability in healing outcomes and increased refracture risk in the adult and complete fracture cohorts(1,2,7,9).
Operative fixation demonstrated high union rates across multiple studies (1,3,8-10). McCormick et al reported an average of 2.7 months to return to regular shoes following operative treatment, with better patient-reported outcomes in those who achieved union compared with those who had developed a nonunion(5). Nunley et al reported high union rates using an algorithmic operative approach incorporating screw fixation with or without bone grafting depending on fracture chronicity and biological risk factors(8). In elite athletes with chronic navicular stress fracture nonunion, Hong et al demonstrated 100% fracture union following vascularized pedicle bone grafting, with 94% of athletes returning to their preinjury level of sport with a mean return to training at approximately 16 weeks(10). These findings highlight the structural reliability and clinical effectiveness of operative fixation, particularly in complete fractures, chronic injuries, and in high-demand patients.
The advantages of operative fixation relate primarily to restoration of structural stability and predictable healing. The navicular bone’s relatively limited vascular supply, particularly in its central third, may impair healing without mechanical stabilization, likely contributing to improved union rates following operative fixation(2,5,12,13). Internal fixation reduces fracture micromotion and restores structural continuity, allowing reliable bone healing and earlier progression to weightbearing activity(14,15). Operative fixation does however carry inherent surgical risks, including infection, neurovascular injury, and hardware-related complications. Hardware irritation requiring removal was reported in 11% of cases in one cohort(7). Although major complications are uncommon, surgical intervention remains invasive and may not be necessary for all fracture type, particularly in lower-risk, incomplete injuries.
Nonoperative treatment demonstrated favorable outcomes in appropriately selected patients, particularly adolescents and individuals with incomplete fractures. Mehta et al reported successful nonoperative treatment in the majority of adolescent navicular stress injuries, with most patients returning to sport within approximately 5 months(9). Adolescents likely demonstrate improved healing potential due to skeletal immaturity and greater biological healing capacity (16,18). Conservative management also demonstrated favorable outcomes in incomplete fractures in adult populations(1,7). However, nonoperative management was associated with greater variability in healing outcomes in complete fractures and adult cohorts. Saxena et al reported approximately 11% refracture rate in conservatively treated patients(7). Conservative treatment also requires prolonged immobilization and activity restriction, which may delay return to sport and increase refracture risk in high-demand individuals(14,18).
Several intrinsic and extrinsic factors contribute to the development of navicular stress fractures. Repetitive loading is the primary extrinsic factor, especially with rapid increases in training volume or intensity(15,17-20). Intrinsic factors including altered foot biomechanics, cavus foot morphology, limited ankle dorsiflexion, and metabolic factors such as bone mineral density may increase susceptibility to stress injury (16,18,20). Recognition of these risk factors is important for early diagnosis, prevention, and individualized treatment strategies to reduce progression to complete fractures and optimize clinical outcomes.
Attia et al performed a systematic review and meta-analysis of 315 navicular stress fractures. They reported pooled successful outcome rates of 97.9% following operative fixation compared with 78.1% following conservative treatment(21). Operative fixation was associated with significantly lower refracture rates, with refracture occurring in only 1.28% of operatively treated fractures compared with 23.5% of conservatively treated fractures(21). Return-to-sport timelines were similar between groups, but there was a trend toward superior structural reliability and reduced refracture risk with operative fixation (21). Mallee et al reported in a systematic review that operative fixation of navicular stress fractures allowed for return-to-sport at 16 weeks as opposed to 22 weeks in the nonoperative cohorts. They support the notion that surgery may offer a faster, more predictable return timeline for some patients, while acknowledging that comparative effectiveness remains limited by the underlying study quality (22). Together, these findings reinforce the role of operative fixation in improving structural healing and reducing refracture risk in high-risk fracture patterns.
Population-specific considerations are critical. Adolescents demonstrated excellent outcomes with nonoperative treatment, reflecting greater biological healing potential(9). In contrast, adult and athletic populations demonstrated more predictable healing following operative fixation, particularly in complete fractures and chronic injuries. Elite athletes represent a unique population in which reliable healing and return to sport are essential. Operative fixation with biological augmentation demonstrated excellent union rates and functional outcomes with chronic navicular stress fracture nonunion(10).
This review is not without limitations. First, study selection was performed by a single reviewer without independent duplicate screening or formal disagreement resolution, which may introduce subjectivity and potential selection bias. Most included studies were retrospective cohort studies, limiting overall level of evidence. Sample sizes were relatively small in several operative cohorts. Additionally, treatment protocols, rehabilitation plans, and outcome measures varied between studies. Several studies reported outcomes qualitatively, rather than a purely quantitative measurement, thus limiting the ability to present fully objective comparisons across cohorts. Selection bias likely influenced treatment assignment, with more severe fractures more likely to undergo operative fixation.
Although consistent trends were observed across studies, these findings were derived mostly from heterogeneous observational cohorts. The differences in study design, patient selection, and outcome measurements limit the ability to perform direct comparisons or establish causality. The results should be interpreted as descriptive rather than definitive, allowing for further prospective, standardized studies to be performed in the future.
Systematic reviews relied primarily on observational data, reflecting on the lack of randomized controlled trails(21,22). No formal risk-of-bias assessment was performed in this review, which may introduce additional selection and reporting bias. Despite these limitations, the consistent patterns observed across primary studies and systematic reviews support the conclusions of this review.
Conclusion
Overall, operative fixation provides a highly reliable fracture union and reduced refracture risk, particularly in complete fractures, chronic injuries, and in athletic populations. Nonoperative treatment remains effective in incomplete fractures and in adolescent populations. CT imaging plays an important role in fracture staging and treatment planning. Treatment decisions should be individualized based on fracture stage, chronicity, and patient-specific functional demands.
References
- Saxena A, Fullem B. Results of treatment of 22 navicular stress fractures and a new proposed radiographic classification system. J Foot Ankle Surg. 2000;39(2):96-103. doi:10.1016/S1067-2516(00)80039-6
- Burne SG, Mahoney CM, Forster BB, Koehle MS, Taunton JE, Khan KM. Tarsal navicular stress injury: long-term outcome and clinicoradiological correlation using both computed tomography and magnetic resonance imaging. Am J Sports Med. 2005;33(12):1875-1881. doi:10.1177/0363546505278253
- Potter NJ, Brukner PD, Makdissi M, Crossley KM. Navicular stress fractures: outcomes of surgical and conservative management. Br J Sports Med. 2006;40(8):692-695. doi:10.1136/bjsm.2006.028217
- Saxena A, Fullem B, Hannaford D. Navicular stress fractures: a prospective study on athletes. Foot Ankle Int.2006;27(11):917-921. doi:10.1177/107110070602701109
- McCormick JJ, Bray CC, Davis WH, Cohen BE, Jones CP 3rd, Anderson RB. Clinical and computed tomography evaluation of surgical outcomes in tarsal navicular stress fractures. Am J Sports Med. 2011;39(8):1741-1748. doi:10.1177/0363546511401899
- Jacob KM, Paterson RS. Navicular stress fractures treated with minimally invasive fixation. Indian J Orthop. 2013;47(6):598-601. doi:10.4103/0019-5413.121589
- Saxena A, Behan SA, Valerio DL, Frosch DL. Navicular Stress Fracture Outcomes in Athletes: Analysis of 62 Injuries. J Foot Ankle Surg. 2017;56(5):943-948. doi:10.1053/j.jfas.2017.06.009
- Nunley JA, Green C, Morash J, Easley ME. Treatment of Navicular Stress Fractures With an Algorithmic Approach. Foot Ankle Int. 2022;43(1):12-20. doi:10.1177/10711007211034812
- Mehta S, Zheng E, Heyworth BE, et al. Tarsal navicular bone stress injuries: a multicenter case series investigating clinical presentation, diagnostic approach, treatment, and return to sport in adolescent athletes. Am J Sports Med.2023;51(8):2161-2168. doi:10.1177/03635465231170399
- Hong CC, Simmons J, Calder J. Vascularized pedicle bone grafting for chronic navicular stress fractures with non-union in elite athletes provided good bony union and ability to return to sports. Knee Surg Sports Traumatol Arthrosc. 2026. doi:10.1007/s00167-025-07918-y
- Torg JS, Pavlov H, Cooley LH, et al. Stress fractures of the tarsal navicular. A retrospective review of twenty-one cases. J Bone Joint Surg Am. 1982;64(5):700-712.
- Khan KM, Fuller PJ, Brukner PD, Kearney C, Burry HC. Outcome of conservative and surgical management of navicular stress fracture in athletes. Eighty-six cases proven with computerized tomography. Am J Sports Med. 1992;20(6):657-666. doi:10.1177/036354659202000606
- Boden BP, Osbahr DC, Jimenez C. Low-risk stress fractures. Am J Sports Med. 2001;29(1):100-111. doi:10.1177/03635465010290010201
- Bennell KL, Malcolm SA, Thomas SA, et al. Risk factors for stress fractures in track and field athletes. Am J Sports Med. 1996;24(6):810-818. doi:10.1177/036354659602400618
- Federicson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging.2006;17(5):309-325. doi:10.1097/RMR.0b013e3180421c8c
- Sterling JC, Edelstein DW, Calvo RD, Webb R 2nd. Stress fractures in the athlete. Diagnosis and management. Sports Med. 1992;14(5):336-346. doi:10.2165/00007256-199214050-00005
- Brukner P, Bennell K, Matheson G. Stress fractures. Lancet. 1997;350(9077):781-785. doi:10.1016/S0140-6736(97)07215-1
- Hulkko A, Orava S, Peltokallio P, Tulikoura I, Walden M. Stress fracture of the navicular bone. Nine cases in athletes. Acta Orthop Scand. 1985;56(6):503-505. doi:10.3109/17453678508993045
- Hulkko A, Orava S. Stress fractures in athletes. Int J Sports Med. 1987;8(3):221-226. doi:10.1055/s-2008-1025650
- Matheson GO, Clement DB, McKenzie DC, Taunton JE, Lloyd-Smith DR, MacIntyre JG. Stress fractures in athletes. A study of 320 cases. Am J Sports Med. 1987;15(1):46-58. doi:10.1177/036354658701500107
- Attia AK, Mahmoud K, Bariteau J, Labib SA, DiGiovanni CW, D’Hooghe P. Return to sport following navicular stress fracture: a systematic review and meta-analysis of three hundred and fifteen fractures. Int Orthop. 2021;45(10):2699-2710. doi:10.1007/s00264-021-05147-6
- Mallee WH, Weel H, van Dijk CN, van Tulder MW, Kerkhoffs GM, Lin CW. Surgical versus conservative treatment for high-risk stress fractures of the lower leg (anterior tibial cortex, navicular and fifth metatarsal base): a systematic review. Br J Sports Med. 2015;49(6):370-376. doi:10.1136/bjsports-2013-093246
