
Cameron Ballard, OMS 2028; Adam Youssef, OMS 2028; Dryden Dalbey, OMS 2028; Paul Doney, OMS 2028; Jeffrey Staudinger, PhD
Kansas City University College of Osteopathic Medicine
DOI: http://doi.org/10.70709/0g2g0epnu37gru
Abstract
Background
Synovial chondromatosis is a rare, benign condition in which synovium transforms into cartilaginous nodules that may detach as loose, intra-articular bodies, resulting in pain, swelling, and restricted motion. Although it most commonly affects the knee and hip, its occurrence in the upper extremity is rare, leading to mismanagement and delayed diagnosis. This study aims to identify optimal treatment strategies for synovial chondromatosis of the upper extremity based on joint involvement and recurrence.
Methods
A PRISMA‑guided systematic review identified 74 case reports/series of upper‑extremity synovial chondromatosis in PubMed, Embase, and Scopus. Titles, abstracts, and full texts were screened to include studies examining the affected joint, treatment, and outcomes. Data was synthesized descriptively to evaluate joint involvement, treatment strategies, and recurrence rates by anatomical location.
Results
97 upper‑extremity synovial chondromatosis cases were identified: shoulder (56), elbow (18), biceps tendon sheath (18), hand (3), and wrist (2). Among shoulder cases, 38 arthroscopic procedures, including synovectomy (± capsular release or acromioplasty), debridement (± loose‑body removal), and related approaches, had a 10.5% recurrence (4/38) with three after synovectomy and one after arthroscopic removal. Open procedures (9), reverse arthroplasty (2), and conservative management (3) showed no recurrences. All elbow cases were recurrence-free, except for a malignant transformation after radiosynovectomy. Excisions in the biceps sheath (18), hand (3), and wrist (2) showed zero recurrences.
Conclusion
Arthroscopic and open techniques provided effective treatment of synovial chondromatosis in the shoulder, elbow, wrist, hand, and tendon‑sheath locations, with a recurrence risk of 10.5% of arthroscopy-related approaches. This may reflect greater synovial surface area and increased joint complexity within proximal joints leading to inadequate excision via arthroscopy. Selection of arthroscopic, combined, or open procedures should be guided by joint anatomy and disease extent with the importance of long-term follow-up to monitor recurrence.
Keywords: Synovial chondromatosis, Upper Extremity, Shoulder Arthroscopy, Synovectomy, Recurrence Rate, Systematic Review
Introduction
Synovial chondromatosis is a rare, benign joint disorder characterized by the transformation of synovial membrane into cartilaginous nodules. These nodules may calcify and either remain attached to the synovium or detach as loose bodies within the affected joint (5). While the condition most commonly affects weight-bearing joints such as the knee and hip, involvement of the upper extremity, including the shoulder, elbow, wrist, and interphalangeal joints are much less common and may lead to diagnostic difficulties and suboptimal management (3, 8, 25). Therefore, understanding joint-specific treatment outcomes may aid in optimizing surgical decision-making for rare cases such as these.
Due to the rarity of upper extremity involvement, there is no standardized treatment approach. Reported strategies range from conservative management to surgical options, including arthroscopic removal, open debridement, and partial or complete synovectomy. Outcomes vary depending on the joint involved, disease severity, and surgical technique. A previous review article published in 2013 in the Journal of Hand Surgery evaluated synovial chondromatosis within the upper extremity. However, newly reported cases and advancements in surgical techniques permit an additional analysis (75). The purpose of this systematic review was to synthesize available case-level evidence to identify treatment strategies for synovial chondromatosis of the upper extremity based on joint involvement and recurrence.
Methods
Study Design and Objective
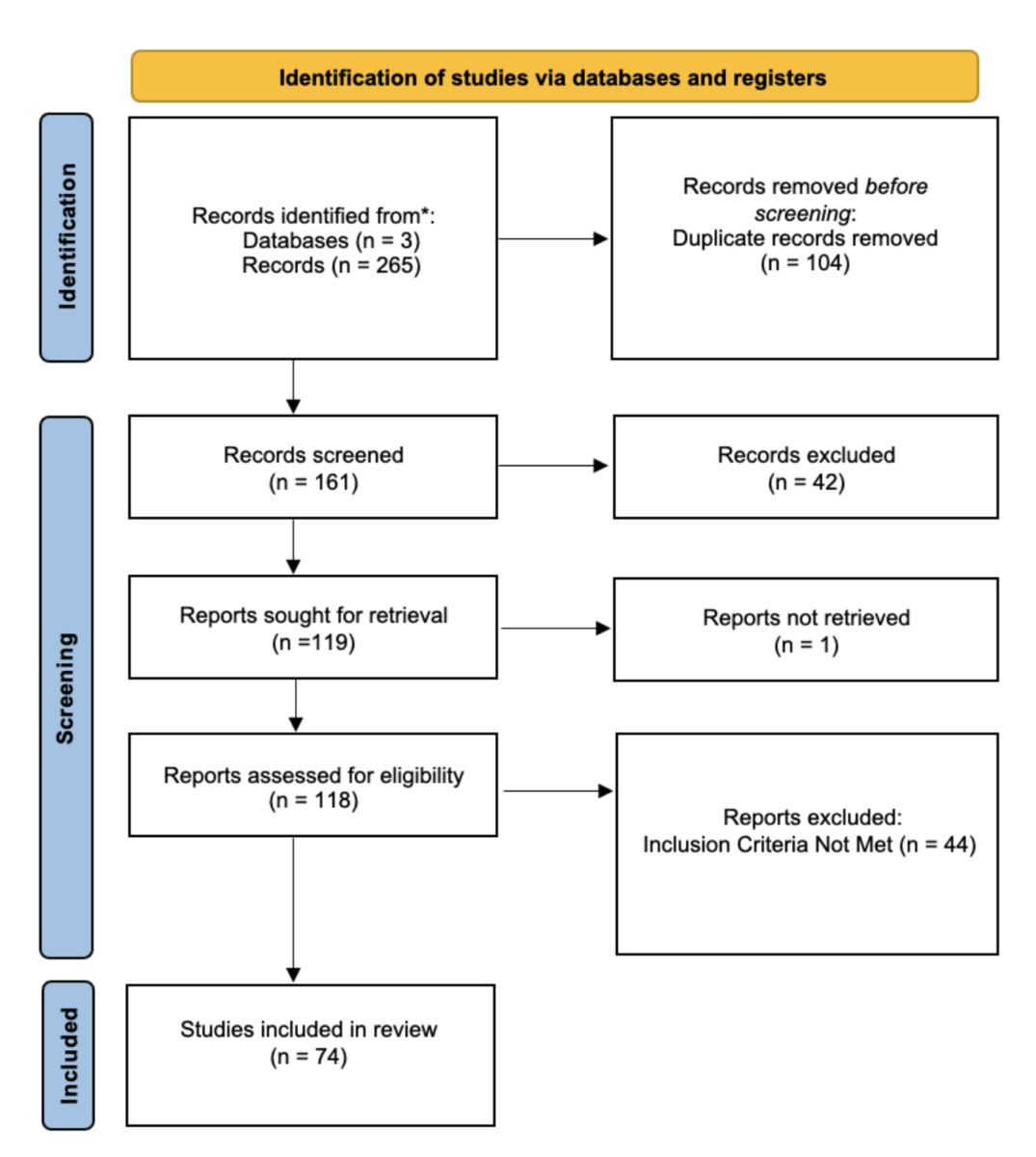
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1). The objective was to synthesize published case reports and case series describing synovial chondromatosis of the upper extremity, with a focus on the joint affected, surgical techniques used, clinical outcomes, and recurrence rates.
Search Strategy and Data Sources
A comprehensive search of PubMed, Embase, and Scopus was conducted between May and June 2025 to identify all case reports describing synovial chondromatosis of the upper extremity, including the shoulder, elbow, wrist, interphalangeal joints, and biceps tendon sheath. The search strategy was developed in consultation with a medical librarian to ensure inclusion of both indexed terms and relevant free-text keywords. No publication date restrictions were applied. Conflicts during screening or full-text review were resolved through consensus.
Inclusion Criteria
(1) Published case reports and/or small case series; (2) patients of any age/sex; (3) upper-extremity synovial chondromatosis; (4) description of management or surgical technique; (5) English language or English translation.
Exclusion Criteria
(1) Retrospective cohort studies and large series without patient-level detail; (2) reviews; (3) non-upper-extremity joints; (4) non-human studies, letters, or articles without management details; (5) low-quality reports by JBI appraisal.
Outcome Measures
The primary outcomes assessed in this PRISMA-guided systematic review were: (1) the specific joint involved in the upper extremity, (2) the surgical technique or management approach used, and (3) the clinical outcome following treatment for synovial chondromatosis.
Data Extraction and Analysis
Titles and abstracts were screened independently by two authors to determine eligibility using a web-based systematic review platform (Rayyan). Articles meeting the initial criteria underwent full-text review to confirm inclusion. The selection process is detailed in the PRISMA flow diagram (Figure 1).
Data extraction was performed independently to ensure consistency, using the following variables: author year/publication, joint affected, surgical approach, treatment outcome, and recurrence status (if reported). Missing data was noted as “Not reported”. A summary of the extracted data is presented in Table 1.
Treatment outcomes were considered successful if there was no recurrence of symptoms or no evidence of loose bodies on postoperative imaging. Surgical interventions were also evaluated in relation to the specific joint involved. Due to several cases involving multiple surgical techniques or multi-site disease, treatment categories were not mutually exclusive. Therefore, the figures reflect procedural frequency rather than unique patient counts.
Search Strategies
Search strategies were tailored to each database using appropriate syntax. The following are the exact search strings used:
- PubMed:
(“Synovial chondromatosis”[Mesh] OR “synovial chondromatosis”[tiab] OR “primary synovial chondromatosis”[tiab] OR (synovial[tiab] AND chondromatosis[tiab]))
AND
(shoulder[tiab] OR elbow[tiab] OR glenohumeral[tiab] OR humerus[tiab] OR olecranon[tiab] OR “upper extremity”[tiab])
AND
(surgery[tiab] OR arthroscopy[tiab] OR “open excision”[tiab] OR synovectomy[tiab] OR management[tiab] OR excision[tiab] OR treatment[tiab] OR intervention[tiab])
- Embase:
(‘synovial chondromatosis’/exp OR ‘synovial chondromatosis’:ti,ab OR ‘primary synovial chondromatosis’:ti,ab OR (synovial:ti,ab AND chondromatosis:ti,ab))
AND
(shoulder:ti,ab OR elbow:ti,ab OR glenohumeral:ti,ab OR humerus:ti,ab OR olecranon:ti,ab OR ‘upper extremity’:ti,ab)
AND
(surgery:ti,ab OR arthroscopy:ti,ab OR ‘open excision’:ti,ab OR synovectomy:ti,ab OR management:ti,ab OR excision:ti,ab OR treatment:ti,ab OR intervention:ti,ab)
- Scopus:
TITLE-ABS-KEY ( “synovial chondromatosis” OR “primary synovial chondromatosis” AND shoulder OR elbow OR glenohumeral OR humerus OR olecranon OR “upper extremity” AND surgery OR arthroscopy OR “open excision” OR synovectomy OR management OR excision OR treatment OR intervention )
AND ( LIMIT-TO ( SUBJAREA , “MEDI” ) )
AND ( LIMIT-TO ( LANGUAGE , “English” ) )
Assessment of Bias
Risk of bias was independently determined through two reviewers using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports, which evaluates quality and potential sources of bias to determine the reliability of individual studies. Each article was scored on an 8-point scale:
- 7–8 points: high quality
- 4–6 points: moderate quality
- ≤3 points: low quality
Only studies rated as high or moderate quality were included to ensure methodological rigor and reliability of the findings.
Reporting Bias Assessment
Due to the inclusion of case reports/case series with no quantitative synthesis being performed, a formal assessment of reporting bias was not executed.
Certainty Assessment
A formal certainty assessment was not performed due to the descriptive nature of the case reports/case series along with no comparison nor pooled statistical analyses.
Results
Study Selection
A total of 119 articles were identified through searches of PubMed, Embase, and Scopus. Following title/abstract screening and full-text review by two independent reviewers, 74 case reports (Table 1) met all inclusion criteria and were included in the final analysis; 67 were rated high quality and 7 were rated as moderate quality using the JBI checklist.
| Authors/Year | Location of Synovial Chondromatosis | Surgical Technique or Conservative Treatment/Management | Outcome |
| Byrd, J.W. (2000) | Elbow | Patient #1 – Arthroscopy with synovial debridement | Patient #1 – Recurrence-free |
| Patient #2 – Arthroscopic debridement | Patient #2 – Recurrence-free | ||
| Covall, D.J., et al. (1994) | Biceps tendon sheath | Open surgery and partial tenosynovectomy | Recurrence-free |
| El Rassi, G., et al. (2015) | Shoulder (extra-articular) | Started on conservative treatment (NSAIDs and physiotherapy). After three months with no improvement, the patient underwent arthroscopy, total bursectomy, and debridement of acromion | Recurrence-free |
| Sachinis, N.P., et al. (2015) | Elbow | 3 rounds of radiosynovectomy | A grade II chondrosarcoma appeared, which was treated with arthroplasty. The cancer metastasized, and an amputation of the shoulder occurred |
| Maier, D., et al. (2014) | Shoulder and Biceps Tendon Sheath | Tenoscopy of the biceps tendon sheath during arthroscopic treatment. Allowed for partial tenosynovectomy | Recurrence-free |
| Griesser, M.J., et al. (2011) | Elbow | Corticosteroid injection and physical therapy at first with minimal relief. Arthroscopic removal and partial synovectomy | Recurrence-free |
| Abay, B., et al. (2014) | Biceps tendon sheath | Open surgery and allograft of bony cysts | Recurrence-free |
| Costa, F., et al. (2018) | Shoulder | Arthroscopy and excision with synovectomy | Recurrence-free |
| Ucpinar, B.A., et al. (2020) | Shoulder | Arthrotomy with concomitant synovectomy | Not reported |
| Ekman, E.F., et al. (1997) | Elbow | Arthroscopic removal | Regained full ROM at 6 months and remained asymptomatic for 5.5 years after pigmented villonodular synovitis. Synovial chondromatosis occurred at 6 years post-op |
| Ruth, R.M., et al. (1996) | Elbow | Elbow arthrotomy | Recurrence-free |
| Ozaki, J., et al. (1993) | Shoulder | Arthrography and synovectomy | Recurrence-free |
| Guglielmino, C., et al. (2019) | Shoulder | Arthroscopy with complete synovectomy | Patient A – Recurrence-free |
| Patient B – incomplete removal of loose bodies, and had a restricted range of motion after treatment despite continuous physiotherapy | |||
| De Smet, L. (2002) | Elbow | Arthroscopy with partial synovectomy | Recurrence-free |
| Tan, C.H.A., et al. (2004) | Shoulder | Patient 1 – arthroscopic drainage | Patient 1 – Recurrence-free |
| Patient 2 – arthroscopic drainage | Recurrence-free | ||
| Algazwi, D.A.R., et al. (2000) | Shoulder, Biceps tendon sheath | Combines arthroscopic and open surgical removal | Not reported |
| Trajkovsk, T., et al. (2011) | Shoulder | Conservative management initially with no improvement in symptoms. Arthrotomy with extensive synovectomy was then performed. | Recurrence-free |
| AlRashed, A.H., et al. (2022) | Wrist | OTC analgesics and physiotherapy were initially used for 2 months with no improvement. Open synovectomy was then performed | Recurrence-free |
| McFarland, E.G., et al. (2000) | Shoulder | NSAID, activity modification, and cryotherapy | Recurrence-free |
| Giannetti, S., et al. (2013) | Elbow | Open synovectomy | Recurrence-free |
| Baǧcier, F., et al. (2016) | Shoulder | Analgesic medications with no improvement. Arthroscopic debridement then proceeded | Not reported |
| Aynaci, O., et al. (2010) | Shoulder | Conservative treatment due to the patient’s refusal | Recurrence-free |
| Fujioka, H., et al. (2011) | Elbow | Synovectomy with removal of chondral fragments and neurolysis | Recurrence-free |
| Vij, N., et al. (2022) | Shoulder | Arthroscopy with extensive debridement | Recurrence-free |
| Reddy, R., et al. (2023) | Elbow | Open synovectomy. | Recurrence-free |
| Memon, F., et al. (2021) | Shoulder | Arthroscopy with partial synovectomy | Recurrence-free |
| Acharya, BM., et al. (2017) | Shoulder | Excisional biopsy | Recurrence-free |
| Fukuda, A., et al. (2019) | Shoulder | Arthroscopic removal and synovectomy | Recurrence-free |
| Terra, BB., et al. (2015) | Elbow | Arthroscopy with partial synovectomy | Recurrence-free |
| Roy, M., et al. (2024) | Elbow | Open synovectomy, ulnar nerve neurolysis, and decompression. | Recurrence-free |
| Kumar, CY., et al. (2023) | Biceps tendon | Arthroscopy and loose body removal | Recurrence-free |
| Colanese, J., et al. (2016) | Shoulder | Arthroscopy and en bloc excision | Recurrence-free |
| Yukata, K., et al. (2018) | Elbow | Arthroscopy and partial synovectomy | Recurrence-free |
| Phalak, M., et al. (2024) | Hand | Vertical capsulotomy of the PIP joint followed by partial synovectomy | Recurrence-free |
| Gill, J., et al. (2019) | Shoulder | Arthroscopy with removal of loose bodies | Recurrence-free |
| Chalasani, P., et al. (2016) | Shoulder and Long Head of Biceps | Excision biopsy | Recurrence-free |
| Hayakawa, K., et al. (2024) | Shoulder | Arthroscopic removal of loose bodies | Recurrence-free |
| Kakichi, T., et al. (2023) | Shoulder | Arthroscopic removal and partial synovectomy | Recurrence-free |
| Orner, C.A., et al. (2023) | Shoulder | Arthroscopic removal and synovectomy | Developed symptoms in the same shoulder 4 years after surgery. Was not investigated due to the patient’s decision |
| Tekaya, A.B., et al. (2023) | Shoulder | Declined surgery. Symptoms improved with anti-tumor necrosis factor drugs. | Recurrence-free |
| Trevisan, M., et al. (2022) | Shoulder | Arthroscopic removal | Recurrence-free |
| Etemad-Rezaie, A., et al. (2022) | Shoulder and biceps tendon sheath | Conservative treatment with physiotherapy for 3 months (no improvement of symptoms). Open shoulder arthrotomy proceeded | Recurrence-free |
| Benvenuti, H., et al. (2022) | Distal interphalangeal joint | Excisional biopsy through dorsal approach, then a second biopsy through volar approach 5 weeks later to allow for proper healing | Recurrence-free |
| Tang, X.F., et al. (2022) | Shoulder | Patient 1 – Arthroscopy | Patient 1 – Recurrence-free |
| Patient 2 – Arthroscopy with acromioplasty | Patient 2 – Recurrence-free | ||
| Lee, H.J., et al. (2021) | Shoulder | Reverse total arthroplasty and extensive synovectomy | Recurrence-free |
| Mo, J., et al. (2020) | Elbow | Open surgery with loose body removal | Recurrence-free |
| Sinikumpu, J.J., et al. (2020) | Shoulder and biceps tendon sheath | Arthrotomy | Recurrence-free |
| Xu, C., et al. (2020) | Shoulder and elbow | Shoulder arthroscopic synovectomy, debridement, biceps tenodesis, and subacromial decompression were conducted first. Elbow arthroscopy occurred 2 months later | Recurrence-free |
| Wahab, H., et al. (2019) | Shoulder | Arthroscopic removal of loose bodies and synovectomy | Recurrence-free |
| Senesi, L., et al. (2019) | Distal Interphalangeal joint | Surgical arthrodesis | Recurrence-free |
| Francesca, J.T., et al. (2018) | Shoulder and biceps tendon sheath | Arthroscopic synovectomy, debridement, and removal of loose bodies were performed, with subsequent conversion to open removal of loose bodies (for the biceps tendon sheath). | Recurrence-free |
| Kreines, A., et al. (2017) | Shoulder | Reverse total arthroplasty, loose body removal, and complete synovectomy | Recurrence-free |
| Frank, J.M., et al. (2016) | Elbow | Open synovectomy | Recurrence-free |
| Raval, P., et al. (2016) | Shoulder | Arthroscopic removal of loose bodies and synovectomy | Recurrence-free |
| Sun, L., et al. (2016) | Shoulder | Open surgical procedure | Recurrence-free |
| Duymus, T.M., et al. (2015) | Shoulder | Arthroscopy with partial synovectomy | Recurrence-free |
| Xu, C., et al. (2015) | Shoulder | Arthroscopy, synovectomy, subacromial debridement, and acromioplasty | Recurrence-free |
| Jung, K.A., et al. (2007) | Shoulder | Anti-inflammatory drugs and physiotherapy, but no sign of relief. Arthroscopy with partial synovectomy was then performed | Recurrence-free |
| Tokis, A.V., et al. (2006) | Shoulder and biceps tendon sheath | Arthroscopy and partial synovectomy | Recurrence-free |
| Chillemi, C., et al. (2005) | Shoulder and biceps tendon sheath | Arthroscopic removal, partial synovectomy, and decompression of the biceps tendon sheath | Recurrence-free |
| Jeon, I.H., et al. (2004) | Shoulder | Arthroscopic removal and partial synovectomy | Showed recurrence of symptoms at 18 months, with densities/calcifications showing on imaging |
| Elmali, N., et al. (2003) | Shoulder | Arthrotomy followed by synovectomy | Recurrence-free |
| Fowble, V.A., et al. (2003) | Shoulder and biceps tendon sheath | Arthroscopy with partial synovectomy. The degenerative labrum was debrided | Recurrence-free |
| Wziȩtek, B., et al. (2002) | Elbow | Arthroscopic removal of loose bodies | Recurrence-free |
| McGrory, J.E., et al. (2000) | Shoulder | Partial synovectomy | Recurrence-free |
| Wójcik, B., et al. (1998) | Shoulder | Arthroscopic removal of loose bodies | Recurrence-free |
| Covall, D.J., et al. (1993) | Shoulder and biceps tendon sheath | Treated with NSAIDS with no improvement of symptoms. 1st Surgery – Arthroscopic debridement with partial synovectomy. 2nd Surgery – Arthroscopic debridement of shoulder and arthroscopic debridement of biceps tendon sheath through open approach | Returned with symptoms after 1st surgery at 18 months. Shoulder involvement started to include biceps tendon sheath. After second surgery, patient has full ROM at 4 month follow up and has resumed normal activities |
| Richman, J.D., et al. (1990) | Shoulder and biceps tendon sheath | Open arthroscopy, partial synovectomy, and debridement of the anterior labrum | Recurrence-free |
| Tormes, F.R., et al. (1978) | Shoulder | NSAID at first, but no relief. Synovectomy was performed | Recurrence-free |
| Ranalletta, M., et al. (2009) | Shoulder | Patient 1 – Arthroscopy with partial synovectomy | Patient 1 – Recurrence-free |
| Patient 2 – Arthroscopy, partial synovectomy, and capsulotomy | Patient 2 – Recurrence-free | ||
| Patient 3 – Arthroscopy, synovectomy, and capsulotomy | Patient 3 – Recurrence-free | ||
| Buess, E., et al. (2001) | Shoulder and biceps tendon sheath | Was receiving anti-inflammatory drugs, but the pain intensified. Then underwent arthroscopy, partial synovectomy, and ventral arthrotomy | Recurrence-free |
| Jones, J.R., et al. (1987) | Patient 1 – Wrist | Patient 1 – extended longitudinal volar incision and excision of swelling. | Patient 1 – Recurrence-free |
| Patient 2 – Elbow | Patient 2 – surgical excision | Patient 2 – Recurrence-free | |
| David, T., et al. (2000) | Shoulder and biceps tendon sheath | Arthroscopic loose body removal, partial synovectomy, and open decompression of the biceps tendon sheath | Recurrence-free |
| Small, R., et al. (1981) | Shoulder and biceps tendon sheath | Patient 1 – A standard deltopectoral incision was made to expose the bicipital groove and anterior shoulder joint | Patient 1 – Recurrence-free |
| Patient 2 – Arthrotomy and debridement of the shoulder. Partial synovectomy was performed | Patient 2 – Recurrence-free |
Table 1: Overview of 74 cases of Synovial Chondromatosis within the upper extremity by location, surgical technique/treatment, and outcome.
Data Synthesis and Analysis
Due to the rarity of synovial chondromatosis within the upper extremity and heterogeneity in reporting, a meta-analysis was not feasible. No formal exploration of the heterogeneity within the reporting was explored and no sensitivity analyses were conducted. The data was descriptively analyzed by (1) anatomical location of the condition, (2) surgical technique or other treatment modalities, and (3) reported outcomes. Patterns were examined to determine treatment effectiveness by joint. Recurrence was defined as either radiographic or symptomatic reappearance as reported in the follow-up with the patient.
Origin of Synovial Chondromatosis
Based on the included case reports within this study, a total of 97 cases of upper-extremity synovial chondromatosis were identified (Figure 1), as several reports described multiple
patients, and some patients had involvement of more than one anatomic site. Presentation within the shoulder predominated as the synovial chondromatosis showed its presence in 56 cases, followed by the elbow and biceps/biceps tendon sheath at 18 cases each. The remaining five cases involved the hand and wrist, with the condition appearing in three cases and two cases, respectively.

Treatment Strategy
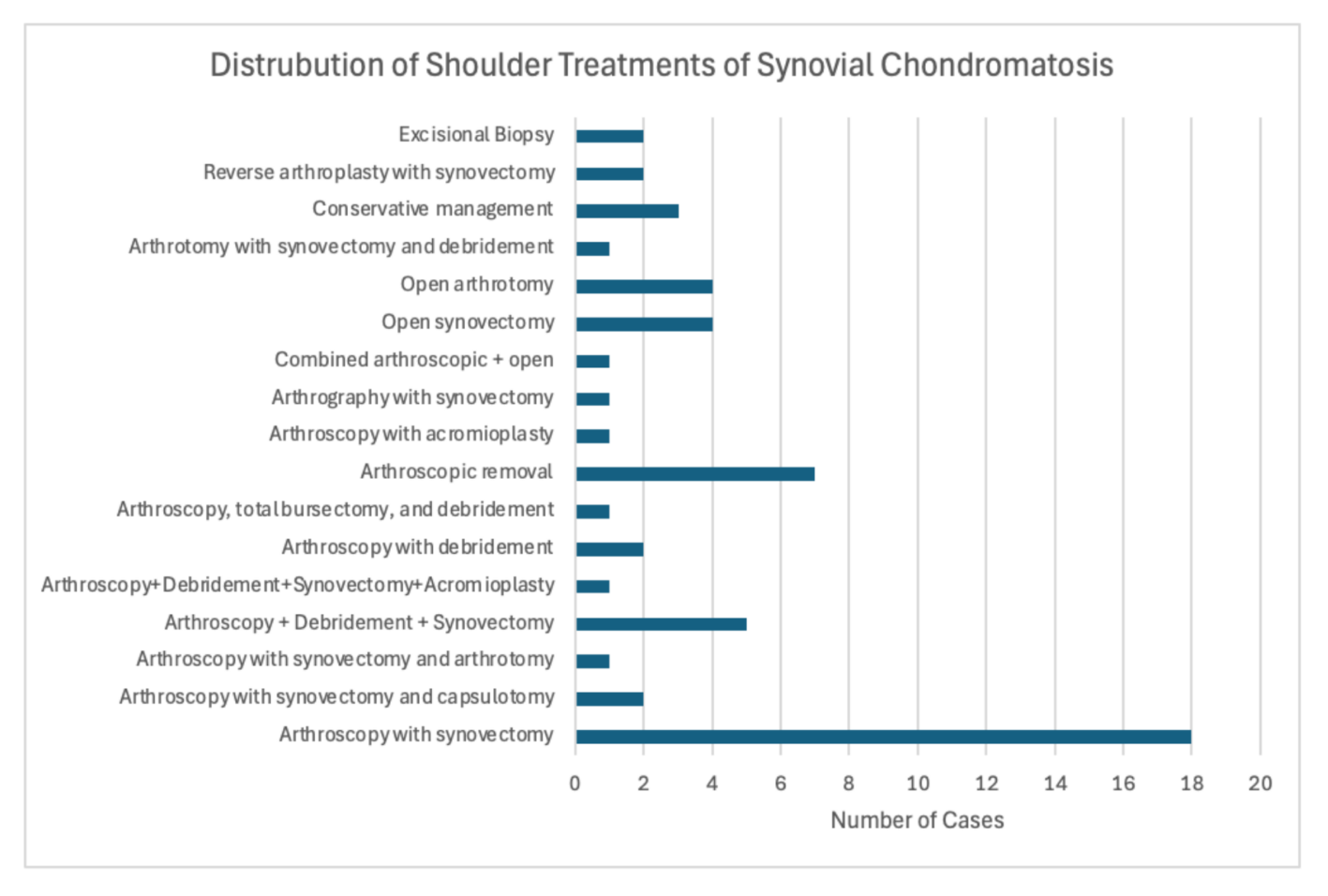
Among the patients who were treated for synovial chondromatosis within the upper extremity, the shoulder was the region most frequently affected (Figure 2). Among the 56 cases of synovial chondromatosis within the shoulder, arthroscopic procedures occurred 38 total times, including arthroscopic subtypes. Arthroscopic approaches included synovectomy alone, synovectomy with capsulotomy, synovectomy with arthrotomy, synovectomy with debridement, synovectomy combined with debridement and acromioplasty, debridement alone, loose-body removal, arthroscopy with acromioplasty, arthrography with synovectomy, and complete labral debridement with synovectomy. Conservative procedures were performed in 3 cases, reverse arthroplasty with synovectomy in 2 cases, and open procedures in 9 cases. The counts reflect individual surgical techniques, as each procedure can be visualized within Figure 3.
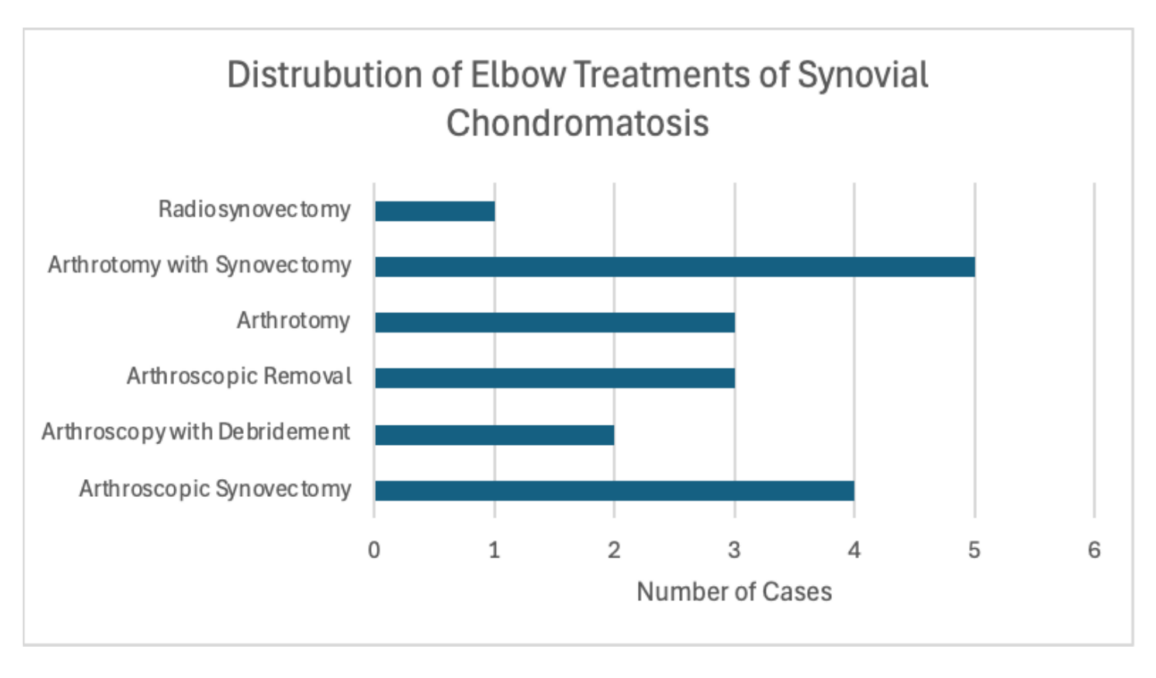
A total of 18 elbow cases were shown to have the occurrence of synovial chondromatosis. Within this region, arthroscopic procedures were shown to make up the majority, with arthroscopic synovectomy (n = 4), arthroscopic debridement (n = 2), and arthroscopic removal (n = 3) performed. Of the open approaches, arthrotomy with synovectomy was utilized the most, with a total of five cases, and arthrotomy alone was used in three cases. Additionally, a single case used radiosynovectomy as a procedure for synovial chondromatosis, but progression to secondary chondrosarcoma occurred, requiring amputation.
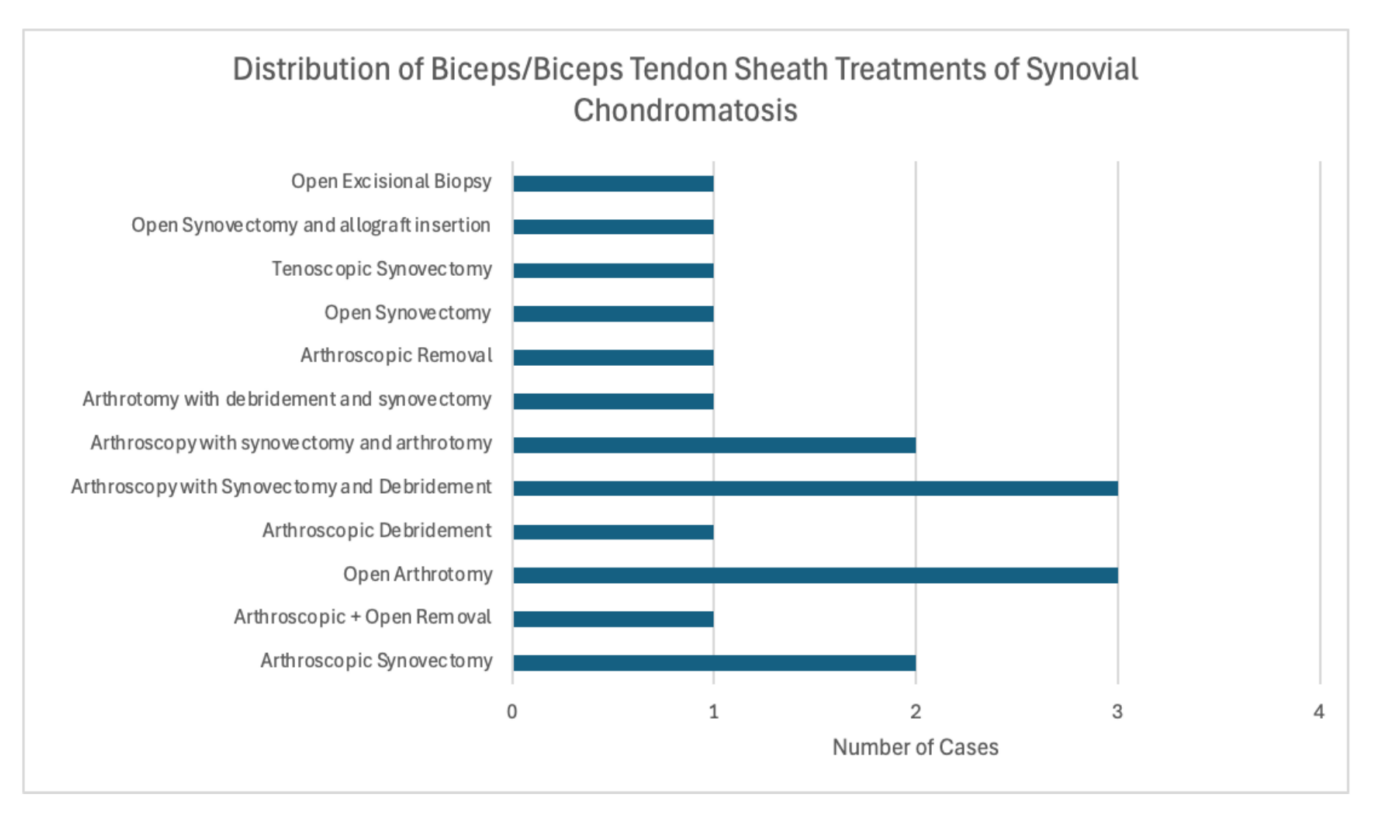
In terms of synovial chondromatosis within the biceps/biceps tendon sheath, there were a total of 18 occurrences. The arthroscopic approaches included synovectomy (n = 2), debridement (n = 1), synovectomy with debridement (n = 3), arthrotomy (n = 2), and arthroscopic removal (n = 1). Open approaches included arthrotomy (n = 3), arthrotomy with debridement and synovectomy (n = 1), open synovectomy (n = 1), open synovectomy with allograft insertion (n = 1), and excisional biopsy (n = 1).
Synovial chondromatosis occurred within the wrist in only two cases, in which one patient underwent an open excision due to swelling, while the other was initially managed conservatively with nonsteroidal anti-inflammatory drugs without symptomatic improvement and subsequently underwent open synovectomy. Three total cases involved the hand/interphalangeal joints with the use of partial synovectomy (n = 1), excisional biopsy (n = 1), and arthrodesis (n = 1).
Outcome/Recurrences
Recurrence of synovial chondromatosis following treatment was rare; however, when recurrence occurred, it predominated in the shoulder. Specifically, three recurrences occurred when arthroscopic removal with complete/partial synovectomy was utilized, and one recurrence occurred when arthroscopic removal was performed as treatment for synovial chondromatosis in the shoulder. In contrast, other surgical approaches, including open, combined, and arthroplasty-based intervention showed no signs of recurrence. In terms of the elbow, no recurrences took place within arthroscopic or open procedures, but one case documented progression of malignant transformation to chondrosarcoma after radiosynovectomy. Notably, all cases involving the biceps/biceps tendon sheath, wrist, and hand/interphalangeal joints documented zero recurrences across the diverse treatment strategies. Finally, one shoulder case reported recurrent symptoms but did not undergo further evaluation due to patient preference, and three case reports did not specify postoperative outcomes.
Discussion
This systematic review consisted of 74 case reports and series across various databases, including PubMed, Embase, and Scopus. The findings confirmed that the shoulder was the most affected site of synovial chondromatosis in the upper extremity. Involvement of the elbow and biceps/biceps tendon sheath followed, but involvement in the wrist/hand displayed a rare occurrence of this condition. The dominance of proximal joint involvement may be related to the increased synovial surface area and complexity of the joint anatomy compared to the more distal joints.
Management strategy varied when treating the shoulder. The most common approach was arthroscopic synovectomy, reflecting the minimally invasive nature and ability to visualize the joint. However, the majority of recurrences took place under this procedure, indicating the possibility that the arthroscopic technique alone might not completely eradicate the synovium of synovial chondromatosis. Other procedures may need to be combined with arthroscopy to eliminate the synovium, leading to superior long-term outcomes for patients.
The elbow was the next most frequently involved site. Similarly, arthroscopic procedures predominated, but both arthroscopic and open procedures showed no evidence of recurrence. These findings suggest that while both approaches can produce favorable outcomes, arthroscopic management may be preferable given its minimally invasive nature and reduced surgical morbidity. There was one recurrence of progression to secondary chondrosarcoma when radiosynovectomy was performed, but a cause-and-effect analysis was not determined within the case report.
The biceps/biceps tendon sheath, wrist, and hand all showed zero recurrences regardless of treatment approach. This could be due to a small joint space, allowing for complete excision compared to the shoulder joint.
Collectively, arthroscopic synovectomy provided the majority of the interventions, but it also consisted of a higher recurrence rate. Therefore, arthroscopy alone may not provide complete excision of the synovium as it would with other combined approaches. However, distal joints showed favorable outcomes with a diverse set of treatment procedures reflecting complete excision within this small joint space.
Limitations
This systematic review is subject to many limitations. First, the topic of the systematic review is of a rare condition described within the upper extremity. Therefore, the power of the meta-analysis was restricted, allowing for only a descriptive analysis to take place. Second, there is a risk for publication bias, as many of these presentations are atypical presentations. Third, follow-up duration was variable, which may allow for underestimation of recurrence rates for the treatment of this specific condition. Lastly, since only English-language/translated case reports/series were included, the exclusion of non-English publications may result in missed cases.
Conclusion
These findings show the importance of personalized treatment planning in terms of synovial chondromatosis in the upper extremity. Therefore, careful selection of arthroscopy, combined, or open procedures should be guided by a variety of factors, including joint anatomy, extent of the condition, and other patient-specific factors contributing to the outcome. Additionally, these cases highlight the importance of long-term follow-up to monitor for recurrence or other transformations. Follow-up duration was highly variable ranging from a low of 9 days to a high of 11 years, with a median follow-up of approximately 1 year among included studies. However, interpretation is limited due to the inconsistent reporting across the included case reports. Further multicenter studies are needed to define treatment plans for evidence-based care. Increased awareness and consistent reporting practices are needed to guide future management and clarify recurrence risk.
Other Information
The systematic review was not formally registered in PROSPERO or other international databases. The authors received no external funding for the research or publication of this scientific article. The authors declare no competing interests and all information analyzed within this study are published articles.
References
- Byrd JW. Arthroscopy of the elbow for synovial chondromatosis. J South Orthop Assoc. 2000;9(2):119-124.
- Covall DJ, Fowble CD. Synovial chondromatosis of the biceps tendon sheath. Orthop Rev. 1994;23(11):902-905.
- El Rassi G, Matta J, Hijjawi A, Khair OA, Fahs S. Extra-articular synovial chondromatosis eroding and penetrating the acromion. Arthrosc Tech. 2015;4(5):e443-e448. doi:10.1016/j.eats.2015.04.001
- Sachinis NP, Sinopidis C, Baliaka A, Givissis P. Odyssey of an elbow synovial chondromatosis. Orthopedics. 2015;38(1):e62-e67. doi:10.3928/01477447-20150105-91
- Maier D, Izadpanah K, Jaeger M, Ogon P, Südkamp NP. Biceps tenoscopy in arthroscopic treatment of primary synovial chondromatosis of the shoulder. Arthrosc Tech. 2014;3(4):e539-e545. doi:10.1016/j.eats.2014.06.011
- Griesser MJ, Harris JD, Likes RL, Jones GL. Synovial chondromatosis of the elbow causing a mechanical block to range of motion: a case report and review of the literature. Am J Orthop. 2011;40(5):253-256.
- Abay B, Aksu N, Soydan R, Ercan E, Kopuz C. Surgical treatment of synovial chondromatosis of the long biceps tendon sheath: a case report. Orthop J Sports Med. 2014;2(11):2325967114S00184. doi:10.1177/2325967114S00184
- Costa F, Freitas JP, Coutinho M, Malcata A. “Stony” shoulder: an exuberant case of glenohumeral synovial chondromatosis with extra-articular extension. BMJ Case Rep. 2018;2018:bcr2018225718. doi:10.1136/bcr-2018-225718
- Ucpinar BA, Sahin C. Primary intra-articular and extra-articular synovial chondromatosis in a child: a rare cause of shoulder pain in children. J Coll Physicians Surg Pak. 2020;30(12):1345-1347. doi:10.29271/jcpsp.2020.12.1345
- Ekman EF, Cory JW, Poehling GG. Pigmented villonodular synovitis and synovial chondromatosis arthroscopically diagnosed and treated in the same elbow. Arthroscopy. 1997;13(1):114-116. doi:10.1016/S0749-8063(97)90219-X
- Ruth RM, Groves RJ. Synovial osteochondromatosis of the elbow presenting with ulnar nerve neuropathy. Am J Orthop. 1996;25(12):843-844.
- Ozaki J, Tomita Y, Nakagawa Y, Kisanuki O, Tamai S. Synovial chondromatosis of the acromioclavicular joint: a case report. Arch Orthop Trauma Surg. 1993;112(3):152-154. doi:10.1007/BF00449994
- Guglielmino C, Giunta ADI, Cassarino AM, et al. Clinical characteristics and treatment outcomes in synovial chondromatosis disease: a case report. Acta Med Mediterr. 2019;35(4):1975-1980. doi:10.19193/0393-6384_2019_4_308
- De Smet L. Synovial chondromatosis of the elbow presenting as a soft tissue tumour. Clin Rheumatol. 2002;21(5):403-404. doi:10.1007/s100670200107
- Tan CHA, Rai SB, Chandy J. MRI appearances of multiple rice body formation in chronic subacromial and subdeltoid bursitis, in association with synovial chondromatosis. Clin Radiol. 2004;59(8):753-757. doi:10.1016/j.crad.2004.03.012
- Algazwi DAR, Gartner LE, Manohara R, Hallinan JTPD. Synovial chondromatosis of the shoulder causing nerve compression. J Clin Rheumatol. 2000;26(8):e289-e290. doi:10.1097/RHU.0000000000001139
- Trajkovski T, Mayne IP, Deheshi BM, Ferguson PC. Synovial chondromatosis of the shoulder: open synovectomy and insertion of osteoarticular allograft with internal fixation to repair intraoperative glenohumeral joint instability. Am J Orthop. 2011;40(8):E154-E158.
- AlRashed AH, Almustafa MA, AlKhars AF, Almuslami AY, AlSaeed MN. A rare case of synovial chondromatosis of distal radio-ulnar joint. Int J Surg Case Rep. 2022;95:107149. doi:10.1016/j.ijscr.2022.107149
- McFarland EG, Neira CA. Synovial chondromatosis of the shoulder associated with osteoarthritis: conservative treatment in two cases and review of the literature. Am J Orthop. 2000;29(10):785-787.
- Giannetti S, Santucci A, Patricola A, Stancati A, Di Sanzo V. Neglected synovial osteochondromatosis of the elbow: a rare case. World J Surg Oncol. 2013;11:233. doi:10.1186/1477-7819-11-233
- Bağcier F, Kul A, Erdal A. Unusual shoulder pain etiology in old man: synovial chondromatosis. Turk Osteoporoz Dergisi. 2016;22(1):72-73. doi:10.4274/tod.22043
- Aynaci O, Kerimoğlu S, Karkucak M, Turgutoğlu O, Şener M. Synovial chondromatosis of the subscapular bursa. Eur J Gen Med. 2010;7(1):94-97. doi:10.29333/ejgm/82825
- Fujioka H, Futani H, Fukunaga S, et al. Posterior interosseous nerve palsy caused by synovial chondromatosis arising in the annular periradial recesses of the elbow. Mod Rheumatol. 2011;21(2):192-196. doi:10.1007/s10165-010-0358-7
- Vij N, Tran TL, Kelly BD, et al. Shoulder synovial chondromatosis in an adolescent athlete: a case report. J Orthop Case Rep. 2022;12(5):101-104. doi:10.13107/jocr.2022.v12.i05.2836
- Reddy R, Reddy VN, Kiran V. A case report of synovial chondromatosis of elbow treated with synovectomy. J Orthop Case Rep. 2023;13(8):28-31. doi:10.13107/jocr.2023.v13.i08.3802
- Memon F, Pawar ED, Gupta D, Yadav AK. Diagnosis and arthroscopic treatment of synovial chondromatosis of glenohumeral joint: a case report. J Orthop Case Rep. 2021;11(1):59-62. doi:10.13107/jocr.2021.v11.i01.1964
- Acharya BM, Devkota P, Shrestha SK, Pradhan NS, Ahmad S. Bilateral symmetrical synovial chondromatosis of shoulder: a case report. Rev Bras Ortop. 2017;53(5):647-650. doi:10.1016/j.rboe.2017.05.009
- Fukuda A, Uemura T, Nishimura A, Kato K, Sudo A. Arthroscopic treatment of primary synovial chondromatosis of the subscapular bursa: a case report. J Orthop Case Rep. 2019;9(6):40-43. doi:10.13107/jocr.2019.v09.i06.1580
- Terra BB, Moraes EW, de Souza AC, et al. Arthroscopic treatment of synovial osteochondromatosis of the elbow: case report and literature review. Rev Bras Ortop. 2015;50(5):607-612. doi:10.1016/j.rboe.2015.08.014
- Roy M, Das D, Shahare P, Dwidmuthe S, Chandrakar D. Management of synovial chondromatosis of the elbow with ulnar nerve palsy by open approach: a case report. Cureus. 2024;16(5):e59807. doi:10.7759/cureus.59807
- Kumar CY, Patil VM, Prajwal K, Reddy BMSK. Unusual case of long head of biceps tendon synovial chondromatosis. J Orthop Case Rep. 2023;13(8):11-14. doi:10.13107/jocr.2023.v13.i08.3794
- Colanese J, Cil A, Egekeze N, Lankachandra K, Kotwal S. Case report of mimicry between synovial hemangioma and synovial chondromatosis of the shoulder. J Orthop Case Rep. 2016;6(4):88-91. doi:10.13107/jocr.2250-0685.586
- Yukata K, Murase M, Hashimoto T, et al. Ulnar nerve palsy caused by synovial protrusion in synovial chondromatosis of the elbow: a case report and literature review. Shoulder Elbow. 2018;10(2):128-132. doi:10.1177/1758573216683396
- Phalak M, Nair A, Reddy R, Chopra S, Kumar S. A rare case of synovial chondromatosis in the proximal interphalangeal joint of the right index finger. Cureus. 2024;16(8):e68072. doi:10.7759/cureus.68072
- Gill J, Tytherleigh-Strong G. Osteochondritis dissecans with associated secondary chondromatosis in an adolescent shoulder. Shoulder Elbow. 2019;11(4):275-281. doi:10.1177/1758573217751653
- Chalasani P, Koduru S, Mikkineni K. A rare case of multiple rice bodies in glenohumeral joint, subscapular recess and along long head of biceps. J Orthop Case Rep. 2016;6(3):53-55. doi:10.13107/jocr.2250-0685.504
- Hayakawa K, Kawano Y, Kuroiwa T, et al. A case of glenohumeral joint impingement caused by a giant secondary synovial osteochondromatosis. Int J Surg Case Rep. 2024;125:110527. doi:10.1016/j.ijscr.2024.110527
- Kakichi T, Funasaki H, Tanaka K, et al. Primary synovial chondromatosis of the shoulder followed for 11 years after arthroscopic surgery: a case report. Radiol Case Rep. 2023;18(12):4253-4257. doi:10.1016/j.radcr.2023.08.104
- Orner CA, Shayan K, Manhard CE, Edmonds EW. Intermediate outcomes of shoulder synovial chondromatosis in an adolescent boy: a case report. JBJS Case Connect. 2023;13(3):e23.00125. doi:10.2106/JBJS.CC.23.00125
- Tekaya AB, Hamdi O, Bellil M, et al. Synovial chondromatosis of the shoulder in rheumatoid arthritis: a case report and brief review of the literature. Curr Rheumatol Rev. 2023;19(3):362-366. doi:10.2174/1573397118666221011113313
- Trevisan M, Di Lenarda L, Pastore S, et al. Shoulder pain and limitation of motion in a young girl: think different. Ital J Pediatr. 2022;48(1):132. doi:10.1186/s13052-022-01332-4
- Etemad-Rezaie A, Tarchala M, Howard A. Primary synovial osteochondromatosis of the shoulder in pediatric patient: case report and review of the literature. Arch Bone Jt Surg. 2022;10(12):1060-1064. doi:10.22038/ABJS.2022.65716.3174
- Benvenuti H, Liao CD, Pinsky B, Christy M. Primary distal interphalangeal joint tenosynovial chondromatosis of the small finger: a case report with literature review. Hand (N Y). 2022;17(6):NP1-NP5. doi:10.1177/15589447211049520
- Tang XF, Qin YG, Shen XY, Chen B, Li YZ. Arthroscopic surgery for synovial chondroma of the subacromial bursa with nontraumatic shoulder subluxation complications: two case reports. World J Clin Cases. 2022;10(5):1645-1653. doi:10.12998/wjcc.v10.i5.1645
- Lee HJ, Han W, Kim K. Secondary synovial chondromatosis of the subacromial subdeltoid bursa with coexisting glenohumeral osteoarthritis. Medicine (Baltimore). 2021;100(47):e27796. doi:10.1097/MD.0000000000027796
- Mo J, Pan J, Liu Y, et al. Bilateral synovial chondromatosis of the elbow in an adolescent: a case report and literature review. BMC Musculoskelet Disord. 2020;21(1):322. doi:10.1186/s12891-020-03322-1
- Sinikumpu JJ, Sinikumpu SP, Sirniö K, Näpänkangas J, Blanco Sequeiros R. Pediatric primary synovial chondromatosis of the shoulder, biceps tendon sheath and subcoracoid bursa. J Clin Orthop Trauma. 2020;11(2):317-320. doi:10.1016/j.jcot.2019.12.005
- Xu C, Yang X. Staged arthroscopic procedure for treating simultaneous shoulder and elbow synovial chondromatosis: a case report and literature review. SAGE Open Med Case Rep. 2020;8:2050313X20951340. doi:10.1177/2050313X20951340
- Wahab H, Hasan O, Habib A, Baloch N. Arthroscopic removal of loose bodies in synovial chondromatosis of shoulder joint, unusual location of rare disease: a case report and literature review. Ann Med Surg (Lond). 2019;37:25-29. doi:10.1016/j.amsu.2018.11.016
- Senesi L, Pangrazi PP, Marchesini A, et al. A rare case of distal interphalangeal chondromatosis in the middle finger: case report with review of literature. Anticancer Res. 2019;39(6):2951-2955. doi:10.21873/anticanres.13425
- Francesca JT, Ronquillo JC. Primary synovial chondromatosis of the shoulder with concomitant intra-articular and extra-articular involvement: More than a simple removal of loose bodies. Tech Shoulder Elbow Surg. 2018;19(1):18-23. doi:10.1097/BTE.0000000000000120
- Kreines A, Ford E, McMillan S, Dingle A. Reverse total shoulder arthroplasty for the treatment of synovial chondromatosis: a case report and review of the literature. Arch Bone Jt Surg. 2017;5(2):117-120. doi:10.22038/abjs.2016.7941
- Frank JM, Saltzman BM, Hemu M, Wysocki RW. Synovial chondromatosis of the elbow with asymptomatic ulnar nerve compression. J Hand Surg Am. 2016;41(11):e429-e431. doi:10.1016/j.jhsa.2016.08.005
- Raval P, Vijayan A, Jariwala A. Arthroscopic retrieval of over 100 loose bodies in shoulder synovial chondromatosis: a case report and review of literature. Orthop Surg. 2016;8(4):511-515. doi:10.1111/os.12294
- Sun L, Yuan L, Gao L, et al. Two cases report about the synovial chondromatosis. Int J Clin Exp Med. 2016;9(6):12170-12174.
- Duymus TM, Yucel B, Mutlu S, Tuna S, Mutlu H, Komur B. Arthroscopic treatment of synovial chondromatosis of the shoulder: a case report. Ann Med Surg (Lond). 2015;4(2):179-182. doi:10.1016/j.amsu.2015.05.001
- Xu C, Yang X, Zhao J. Arthroscopic treatment for synovial chondromatosis of the subacromial bursa associated with partial rotator cuff tear. Knee Surg Sports Traumatol Arthrosc. 2015;23(2):600-602. doi:10.1007/s00167-014-3308-7
- Jung KA, Kim SJ, Jeong JH. Arthroscopic treatment of synovial chondromatosis that possibly developed after open capsular shift for shoulder instability. Knee Surg Sports Traumatol Arthrosc. 2007;15(12):1499-1503. doi:10.1007/s00167-007-0357-1
- Tokis AV, Andrikoula SI, Chouliaras VT, Vasiliadis HS, Georgoulis AD. Diagnosis and arthroscopic treatment of primary synovial chondromatosis of the shoulder. Arthroscopy. 2007;23(9):1023.e1-1023.e5. doi:10.1016/j.arthro.2006.07.009
- Chillemi C, Marinelli M, De Cupis V. Primary synovial chondromatosis of the shoulder: clinical, arthroscopic and histopathological aspects. Knee Surg Sports Traumatol Arthrosc. 2005;13(6):483-488. doi:10.1007/s00167-004-0608-3
- Jeon IH, Ihn JC, Kyung HS. Recurrence of synovial chondromatosis of the glenohumeral joint after arthroscopic treatment. Arthroscopy. 2004;20(5):524-527. doi:10.1016/j.arthro.2004.03.014
- Elmali N, Esenkaya I, Alkan A. Synovial chondromatosis: a report of four cases with three diverse localizations. Acta Orthop Traumatol Turc. 2003;37(2):173-177.
- Fowble VA, Levy HJ. Arthroscopic treatment for synovial chondromatosis of the shoulder. Arthroscopy. 2003;19(1):E2.
- Wziętek B, Frańczuk B. Arthroscopic management of chondromatosis of the elbow: a case report. Chir Narzadow Ruchu Ortop Pol. 2002;67(3):366-369.
- McGrory JE, Rock MG. Synovial chondromatosis of the shoulder. Am J Orthop. 2000;29(10):793-795.
- Wójcik B, Wojciechowski P. Arthroscopic treatment for synovial chondromatosis of the shoulder: case report. Chir Narzadow Ruchu Ortop Pol. 1998;63(2):169-172.
- Covall DJ, Fowble CD. Arthroscopic treatment of synovial chondromatosis of the shoulder and biceps tendon sheath. Arthroscopy. 1993;9(5):602-604. doi:10.1016/S0749-8063(05)80414-1
- Richman JD, Rose DJ. The role of arthroscopy in the management of synovial chondromatosis of the shoulder: a case report. Clin Orthop Relat Res. 1990;(257):91-93. doi:10.1097/00003086-199008000-00018
- Tormes FR, Hardin NJ, Pledger SR. Synovial chondromatosis of the shoulder: case report. Mil Med. 1978;143(12):872-874. doi:10.1093/milmed/143.12.872
- Ranalletta M, Bongiovanni S, Calvo JM, Gallucci G, Maignon G. Arthroscopic treatment of synovial chondromatosis of the shoulder: report of three patients. J Shoulder Elbow Surg. 2009;18(3):e4-e8. doi:10.1016/j.jse.2008.12.003
- Buess E, Friedrich B. Synovial chondromatosis of the glenohumeral joint: a rare condition. Arch Orthop Trauma Surg. 2001;121(1):109-111. doi:10.1007/s004020000168
- Jones JR, Evans DM, Kaushik A. Synovial chondromatosis presenting with peripheral nerve compression: a report of two cases. J Hand Surg Br. 1987;12(1):25-27.
- David T, Drez DJ Jr. Synovial chondromatosis of the shoulder and biceps tendon. Orthopedics. 2000;23(6):611-613.
- Small R, Jaffe WL. Tenosynovial chondromatosis of the shoulder. Bull Hosp Jt Dis Orthop Inst. 1981;41:37-47.
- Ho Y, Chouecka J. Synovial chondromatosis of the upper extremity. J Hand Surg Am. 2013;38(4):804-810. doi:10.1016/j.jhsa.2013.01.041
