
Dustin Volkmer MD1; Natalie Nacy, BS, OMS II2; Alexandra Wade, BS, OMS II3
1Avera Orthopedics
2Burrell College of Osteopathic Medicine
3Idaho College of Osteopathic Medicine
DOI: http://doi.org/10.70709/g67qy5gpwyfkcg
Abstract
The physical demands of dance predispose athletes to morphological changes that can increase their risk of injury. The hip is particularly at risk, where hyperflexion, excessive external rotation, and hyperabduction are required for many dance positions. Morphological hip changes such as dysplasia and prominence of the anterior inferior iliac spine can lead to a variety of injuries in the dance population, including femoroacetabular impingement (FAI), labral tears, external and internal snapping hip syndrome, and microinstability. With the recent rise in the popularity of dance, it has become increasingly important to diagnose hip pathologies in dancers accurately and to understand how these structural changes affect the body in order to guide effective treatment. Diagnosing hip injuries in dancers can be complex, as symptoms often overlap with other conditions. When properly identified early, conservative treatments such as rest, activity modification, and physical therapy are often highly effective. In some cases, surgical treatment may be necessary and has been shown to produce favorable long-term outcomes. The purpose of this review is to provide a concise summary of current literature on hip pathologies in the dancing athletes and discuss standard diagnostic and treatment options.
Keywords: female, hip, dancer, impingement, microinstability, arthroscopy
Introduction
Interest in dance sports has experienced an upward trajectory over the past several years, fueled in part by a significant increase in virtual dance class participation resulting from the COVID-19 pandemic. The presentations of specific patterns of hip injuries are coinciding with this uptick in sport participation, which has led to increased attention to “dancer’s hip.”The spectrum of dancing sports places unique demands on the athlete’s hip. Competitive dancers typically begin training at a very young age and learn techniques that emphasize supraphysiologic motion of the hip including hyperflexion, external rotation, and abduction. Studies have reported that 14-27% of reported injuries in dancers are related to the hip and groin (1). However, as hip pathology in the younger population becomes better understood and further hip preservation techniques are developed, this incidence is likely to increase.
The purpose of this review is to provide a comprehensive overview of hip pathologies in the dancing athlete, with a focus on dance-specific morphologic adaptations, diagnostic challenges, and treatment strategies. This review aims to synthesize current research to guide accurate diagnosis, effective management, and optimal outcomes for dancers experiencing hip injuries.
Pathoanatomy of Hip Injuries in Dancers
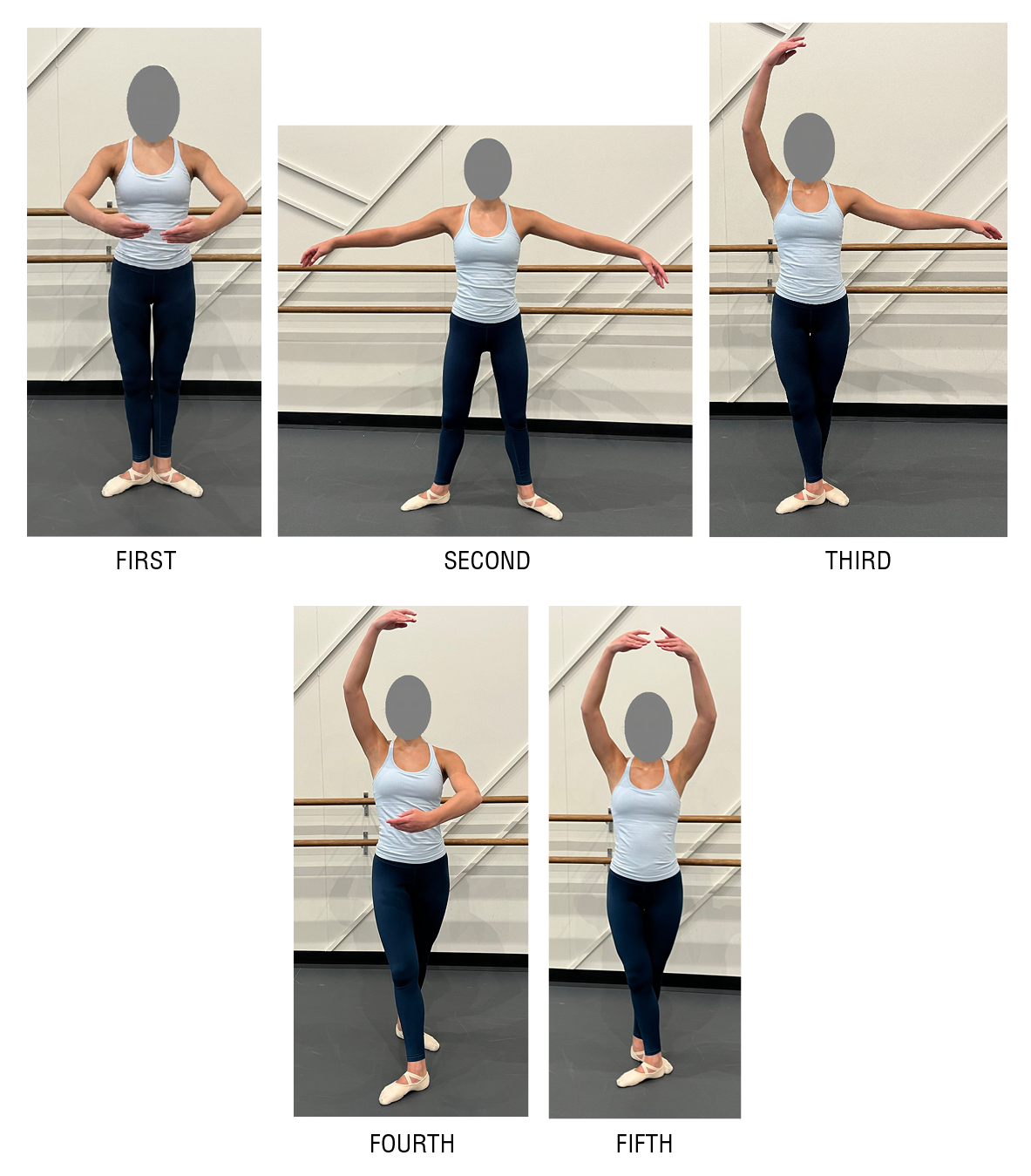
Dance sports have traditionally been grouped with other “flexibility sports” such as gymnastics, martial arts, and figure skating. However, each of these disciplines places unique demands on the athlete’s hip. Similar to other flexibility sports, dance places great emphasis on hyperflexibility, particularly of the hips and lumbar spine. These positions require very specific alignment, muscle control, body position, and movement follow-through for optimal dance performance technique. Increased strength in the hip, core, and trunk musculature to maintain body control places a dynamic load across the hip joint. In contrast to other sports, dance also demands extremes of rotation, especially external rotation, to achieve basic positions. The five standard ballet positions emphasize maximum external rotation, which is sustained and at the limit of physiologic motion of the hip, in contrast to brief or submaximal external rotation, such as kicking a ball (Figure 1). Dance instruction and training often begin as young as three years of age, where these extremes of motion can lead to adaptive changes to the acetabulum, proximal femur, and surrounding soft tissues over time. Soft tissue changes can subsequently lead to microinstability of the hip, which then further places shear forces across the joint, including the articular cartilage and chondrolabral complex.
In addition to physiologic adaptations to extreme hip positions, the dance training period tends to be year-round as opposed to other seasonal sports. In the skeletally immature athlete, the cumulative loads on the hip joint can lead to overuse injuries and further contribute to adaptive changes to the bony and soft tissue components of the joints. Studies have shown that higher-volume dancers have a higher incidence of hip dysplasia and decreased femoral anteversion, both of which are advantageous for obtaining increased flexion and external rotation (2). Repetitive extremes of motion have also been correlated with increased joint laxity and microinstability of the hip, increasing the risk for soft tissue injuries such as labral tears of the hip. Dance sports traditionally place value on lower body weight and leaner appearance, which contributes to psychosocial pressure to limit caloric intake and puts the athlete at risk for conditions such as relative energy deficiency in sports (RED-S). RED-S is an increasingly recognized cause of serious physical and psychological detrimental outcomes in this patient population, which itself contributes to decreased bone mineral density, increased risk of stress fracture or overuse injuries, hormonal imbalances, and psychological distress (3).
Diagnostic Considerations
Hip pain in a dancing athlete is a complex entity with multiple potential causes and co-existing conditions. Particularly in the dance athlete, lumbar spine issues such as spondylolisthesis can masquerade as hip pain and must be adequately evaluated concurrently with hip pathology. Classic characteristics from the patient’s history such as pain location, quality, severity, as well as aggravating factors, can provide imperfect clues in the setting of hip pain. Anterior or deep groin pain is thought to be associated with impingement or hip flexor tendinitis. Lateral hip pain may be an indicator of abductor tendinitis, abductor fatigue from dysplasia, or postero-superior impingement with hyperabduction, external rotation, and hyperextension activities. Quality of the pain is important to note, as delayed muscle fatigue is more closely correlated with dysplasia or microinstability, as opposed to a sharp, sudden pain which is associated with mechanical impingement. A thorough exploration of the intensity of training and timing within the performance schedule may also be beneficial to identify aggravating factors.
Physical exam testing is similarly non-specific in the setting of athletic hip pain. Range of motion may be increased with hyperlaxity, but this increased range of motion is not necessarily pathologic in the dance cohort. Strength may be normal on exam in the clinic but decreases after dance activities in patients with dysplasia. Therefore, it may be beneficial to perform an exam after prolonged dance activities for improved reliability. Special exam maneuvers such as flexion/adduction/internal rotation (FADIR) and flexion/abduction/external rotation (FABER) tests may be helpful to identify anterior impingement, posterior superior impingement, and iliopsoas tendon pathology, but once again, these testing techniques may be difficult to adequately assess a hyperlax patient.. Microinstability maneuvers such as abduction-hyperextension-external rotation (AB-HEER) can help to identify microinstability, typically in the anterior direction.
Given the imprecise nature of history and physical exam maneuvers in definitively identifying the source of hip pain, a valuable diagnostic tool is a targeted injection of local anesthetic. Ultrasound-guided injections into the femoroacetabular joint, the iliopsoas tendon sheath, and the abductor tendon region can assist in sequentially ruling out various pain generators about the hip. Given the young age of most patients in this population cohort, the authors do not typically use corticosteroid injections due to the risk of chondrotoxicity and limited long-term benefit.
MR arthrogram has become the gold standard for improving diagnostic accuracy in patients who fail conservative treatment or in those who would benefit from further diagnostic imaging. This modality has shown variable sensitivity and specificity for evaluating labral tears of the hip, with some studies reporting up to 87-97% sensitivity in the adult population (4). However, a study by Kelly et al. reported lower sensitivities in the adolescent and young adult population and discrepancies between radiologists and surgeons, with 55% sensitivity by radiologists vs 65% sensitivity by surgeons (5). Thus, even with advanced imaging, labral tears may be difficult to diagnose clinically due to normal variations in anatomy and very subtle radiographic findings.
Dance-Specific Hip Pathology
Femoroacetabular Impingement
Femoroacetabular impingement (FAI) is a common intra-articular hip pathology in dancers and can contribute to hip pain as well as functional limitations. FAI is defined by abnormal contact between the femoral head/neck junction and the acetabular rim, which can lead to progressive cartilage and labrum injury. The primary morphologic subtypes are CAM, pincer, and subspine impingement, all of which are frequently observed in high-level dancers due to supraphysiological hip motion.
CAM-Type Impingement
CAM impingement is characterized by an aspherical femoral head that results in shear forces at the acetabular cartilage during flexion and internal rotation (figure 2). This can lead to posterosuperior labral tears and cartilage lesions in dancers who perform extreme movements such as turnout and splits repetitively. These stress patterns have been visualized through imaging and motion analysis studies in ballet dancers, even without apparent hip dysplasia or limited passive range of motion (1-3).
High training intensity during skeletal development, particularly between ages 11 and 14, has been associated with the development of femoral retroversion and CAM morphologies in dancers (2). Ultrasound-based studies have identified CAM-type morphologies in 65% of professional ballet dancers, with men showing a higher risk. Additionally, 95% of dancers with labral tears had a concurrent CAM lesion (5). Radiographic studies have also shown that CAM morphology may be present in asymptomatic dancers, underscoring the importance of clinical context (6).
Pincer-Type Impingement
Pincer impingement occurs when there is excessive acetabular coverage of the femoral head, causing compressive forces on the labrum during the terminal range of motion. This morphology has been observed in up to 74% of professional ballet dancers, with males more commonly exhibiting radiographic indications such as a prominent ischial spine and posterior wall sign (6). The repetitive use of extreme external rotation and abduction may exacerbate impingement mechanics and lead to degeneration of the labrum (3, 7).
Unlike CAM lesions, the association between pincer morphology and symptomatic hip pain is less direct. One study found that while dancers with pincer morphology demonstrated a higher rate of cartilage lesions, this did not always correlate with reported pain (8). Additionally, pincer-type impingement often coexists with capsular laxity in dancers, further complicating both diagnosis and treatment planning (9).
Surgical management of FAI in dancers typically includes labral repair and careful resection of impingement lesions. Given the demands of dance, capsular closure is essential to avoid instability, and capsular plication may be considered in cases of extreme laxity. However, overtightening the capsule should be avoided to preserve critical ranges of motion like turnout and extension (2, 10).
Subspine Impingement
An abnormality of the anterior inferior iliac spine (AIIS) causes a distinct type of mechanical hip impingement called subspine impingement that can be differentiated from the CAM and Pincer impingements previously discussed. This abnormality includes a prominence of the AIIS at the level of the acetabular rim, which can impinge the anterior hip joint capsule or the iliocapsularis muscle origin against the femoral head-neck junction during hip flexion, a position vital to the sport of dance. This prominence can develop from repeated strain on the bone, including a hip flexor avulsion fracture ossifying below the AIIS. Diagnosis of this type of impingement can be complicated as symptoms can mimic those of a typical hip strain. CT scan is typically the most reliable way to decipher between the two entities, as this will reveal AIIS prominence or osteophyte formation. Patients with this kind of bony morphology will also not see improvement with conservative measures like a typical hip strain would, making surgical resection the most definitive treatment option for subspine impingement (12)
Labral Tears
Labral tears are one of the most prevalent intra-articular hip pathologies seen in dancers and are frequently associated with FAI, microinstability, or dysplasia. These tears are often localized to the posterosuperior or anterosuperior acetabulum, reflecting the unique biomechanical stresses encountered in dance-specific movements such as turnout, splits, and grand pliés (1, 2).
In a cohort of elite ballet dancers, MRI and motion analysis during extreme positions (e.g., the splits) revealed labral tears alongside cartilage thinning and herniation pits, with many of these findings occurring even in asymptomatic individuals (3).Notably, 95% of dancers with labral tears also had a CAM lesion, supporting the connection between abnormal bony morphology and labral pathology (4).Despite the frequency of tears, pain is not always present, and the symptoms may be influenced by concurrent instability or capsular laxity (5).
Surgical management focuses on labral repair to restore the suction seal of the hip joint, which is essential for maintaining joint stability in hypermobile athletes (6). Outcomes following arthroscopic labral repair in dancers are generally positive, with return-to-dance rates as high as 97%, although only about half return to their previous level of performance (7, 8). The requirement to regain supraphysiologic motion is often a challenge in rehabilitation, increasing the risk for recurrent injury.
External Snapping Hip Syndrome
External snapping hip syndrome is one of the most common hip conditions that dancers encounter (13). Repetitive hip movements required for dance such as hip flexion and extension with abduction, result in tightening of the iliotibial (IT) band in the hip. Eventually, the IT band will continue to tighten and “snap” while passing over the greater trochanter. Over time, this leads to a progression of weakness, lateral hip pain, and decreased range of motion.14 An increased hip range of motion has been found to be an important morphology that dancers have developed for the sport. The decreased range of motion caused by external snapping hip can be detrimental and even cause retirement from the sport (13, 14).. Unfortunately, symptoms are significantly underreported, resulting in a low diagnosis rate for this hip pathology in dancers. However, when diagnosed early, patients usually have good improvement with conservative treatment including rest, soft tissue massage, stretching, non-steroidal anti-inflammatories, and light physical therapy. If the patient does not return to full recovery within 6 months, more invasive options can be explored including localized steroid injection and endoscopic IT band release (14).
A study comparing overuse injuries in different ballet disciplines found that external snapping hip was significantly more common in classical ballet and Spanish ballet than it was in neoclassical or contemporary. Structure and regulation in technique decreases from classical down to contemporary, meaning with more freedom in movement there was less evidence of overuse injuries such as snapping hip since movements are not as repetitive (17).This should be taken into account to help implement techniques that could limit the risks of developing external snapping hip syndrome (14).
Iliopsoas Impingement Syndrome
Iliopsoas impingement syndrome is commonly also referred to as internal snapping hip syndrome. Similar to external snapping hip syndrome, it results from repetitive hip movements of flexion and abduction that result in tightening of the iliopsoas tendon and impingement/snapping over bony prominences (13). However, in contrast to external snapping hip, pain is localized anteriorly instead of laterally. It is often confused for other hip pathologies, but a retrospective study assessing 653 patients was able to narrow down positive exam findings definitive for iliopsoas impingement. These exam findings include weakness with resisted hip flexion in abduction and symptomatic clicking/snapping with a positive iliopsoas test. After positively identifying the patients with iliopsoas syndrome in this retrospective study, these patients were then put on a guided physical therapy protocol to assess the efficacy of conservative treatment for this etiology. The study found that all patients had a 100% improvement with conservative treatment of non-steroidal anti-inflammatory drugs, physical therapy, and activity modification, making this the standard for iliopsoas treatment (16). Although studies have found success of treatment for iliopsoas syndrome with conservative measures, it has also been found that iliopsoas impingement directly correlates with anterior labral tears, which as described above, often require surgical intervention (12).
Hip Dysplasia
Hip dysplasia is characterized by shallow acetabular coverage and increased femoral anteversion, which can contribute to instability, labral overload, and secondary FAI. Dancers with hip dysplasia often exhibit excessive joint motion and compensatory mechanisms to achieve the extreme hip ranges required by their sport (9).
Radiographic studies in elite ballet populations have shown that 89% had signs of dysplasia in at least one hip, with bilateral dysplasia more common in females (10). Although dancers with dysplasia may demonstrate normal passive ROM, the deficiency in bony support predisposes them to subluxation, particularly during high-demand movements. MRI studies have quantified this, indicating an average femoral head subluxation of 2.05 mm in dancers performing the splits (4).
This structural instability can lead to progressive labral degeneration and is often underrecognized in the early stages (11). In these cases, capsular plication during hip arthroscopy may be warranted to enhance stability, though care must be taken not to restrict motion essential to performance (6). In more severe dysplasia, periacetabular osteotomy (PAO) may be considered, particularly if instability persists or joint preservation is prioritized (9).
Microinstability of the Hip or “Hip Hypermobility Syndrome”
Microinstability of the hip is an increasingly recognized source of hip pain, particularly in the flexibility sport athletes. An alternate name of “hip hypermobility syndrome” has been proposed to more accurately describe the constellation of symptoms, clinical exam findings and radiographic findings that accompany this complex entity. Although studies have demonstrated increased incidence of dysplasia in the dance population (6), this hypermobility can occur even in the absence of dysplastic morphology due to laxity of the soft tissue restraints of the hip. Duthon et al. demonstrated increased degrees of subluxation of the hip in female dancers in the “splits” position, regardless of acetabular morphology (1). An additional study by Harris et al. demonstrated increased femoral head translation in symptomatic female dance athletes compared to non-dance athletes, as well as asymptomatic dance athletes (7). Hip hypermobility is advantageous in the dance population since most standard dance positions require extremes of motion, including external rotation, flexion, extension, and abduction.
Treatment Considerations in Dancers
Initial treatment of hip pathology in the dance population typically follows standard of care conservative treatment such as rest, activity modification, and physical therapy focused on improving core strength and hip abductor strength. Corticosteroid injections are rarely indicated in this population due to the relatively younger age of most patients and concern for chondrotoxicity.
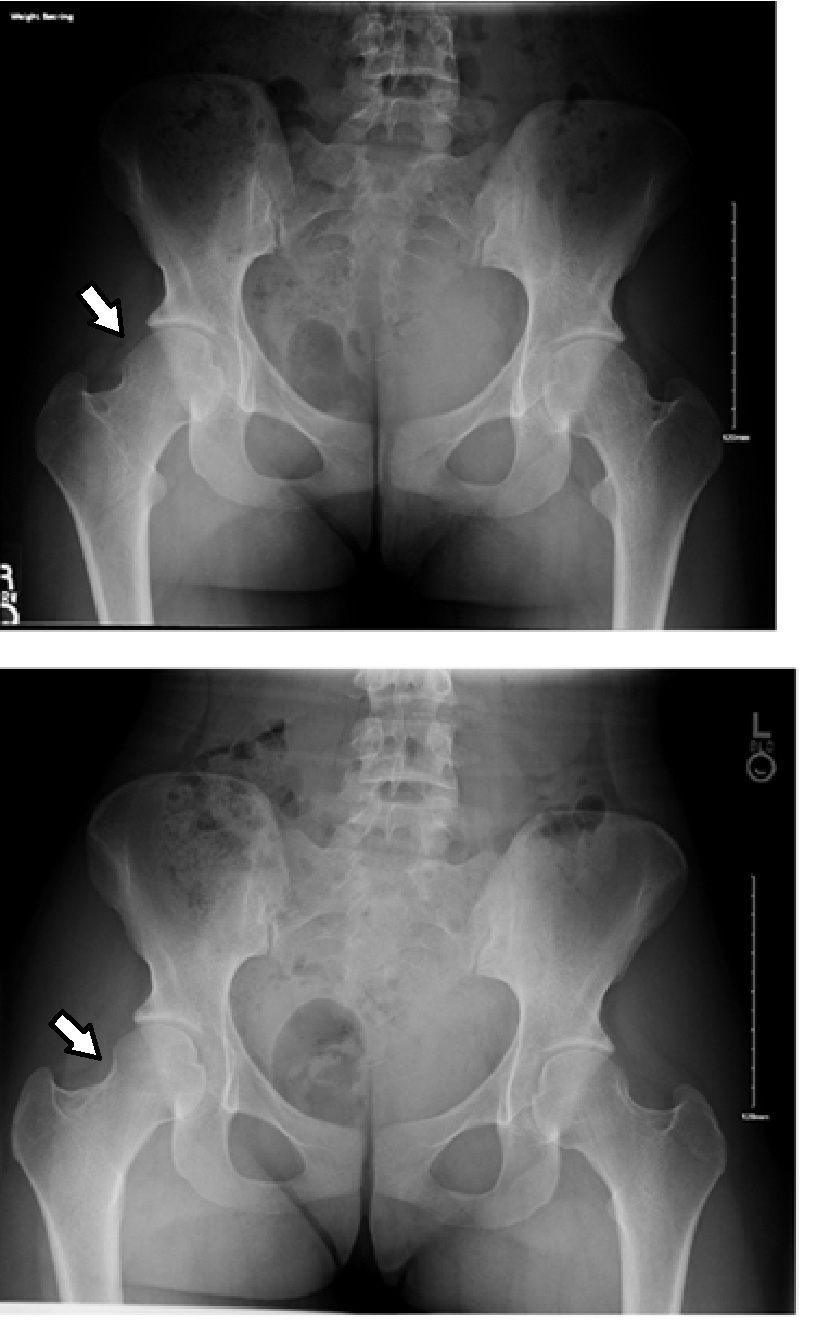
Surgical management, when indicated, should be undertaken with caution as this population presents unique challenges with surgical techniques and post-operative return to sport progression. Several modifications have been utilized to address the specifics of a dancer’s hip, including posterior acetabular rim decompression, subspine decompression, and more distal femoral neck osteoplasty. Dancers present more frequently with posterior-superior impingement than the general population due to extremes of abduction and external rotation (figure 3) and may impinge more distally on the femoral neck due to extreme hyperflexion (figure 4).


Careful capsular management is of paramount importance during arthroscopic procedures for a dancer’s hip. Many dancers have compensatory increased laxity of the hips to allow for increased motion demands, and addressing this laxity surgically may result in “over-tightening” of the hip and diminished performance ability. The surgeon’s challenge is to identify the appropriate amount of laxity for the individual patient. Conversely, improper capsular resection or failed capsular repair may accentuate pre-existing laxity, creating further instability and diminished performance. Similarly, a relatively high percentage of patients have some form of acetabular dysplasia, and therefore, over-resection during acetabuloplasty may create additional instability with subsequent pain and diminished performance. Iliopsoas lengthening and IT band lengthening for snapping hip should also be undertaken with caution due to the risk of diminished flexion strength and additional instability of the hip.
Despite the technical complexity of hip arthroscopy in the dancing athlete, studies have demonstrated excellent outcomes and high rates of return to sport. Ukwuani et al. reported up to 97% return to participation at an average of 6.9 months, with 62.5% returning at a higher level than pre-op (11).
Conclusions
Dancing athletes represent a unique patient population with an increased risk for hip injuries. Given the unique demands these activities place on the hip, these injuries present both diagnostic and treatment challenges for the health care team. Recent studies have shown excellent outcomes for arthroscopic management of many hip pathologies in the dance population, but meticulous care must be taken to arrive at the correct diagnosis and provide appropriate treatment.
Acknowledgements
The authors gratefully acknowledge the assistance of BritZa Performing Arts Studio (Sioux Falls, SD) and Champion Legacy Dance Academy (Sioux Falls, SD) for providing photos for this article.
Disclosures
The authors declare no known conflicts of interest in the authorship and publication of this article.
References
- Duthon VB, Charbonnier C, Kolo FC, et al. Correlation of clinical and magnetic resonance imaging findings in hips of elite female ballet dancers. Arthroscopy. 2013;29(3):411-419. doi:10.1016/j.arthro.2012.10.012.
- Hamilton D, Aronsen P, Løken JH, et al. Dance training intensity at 11-14 years is associated with femoral torsion in classical ballet dancers. Br J Sports Med. 2006;40:299-303.
- Allen N, Kelly S, Lanfear M, et al. Relative energy deficiency in dance (RED-D): a consensus method approach to REDs in dance. BMJ Open Sport Exerc Med. 2024 Mar 7;10(1):e001858. doi: 10.1136/bmjsem-2023-001858.
- Charbonnier C, Kolo FC, Duthon VB, et al. Assessment of congruence and impingement of the hip joint in professional ballet dancers: A motion capture study. Am J Sports Med. 2011;39:557-566.
- Kelly CM, Chevalier NM, Vogel LA, et al. Sensitivity of magnetic resonance imaging for labral pathology in adolescent and young adult athletes. Orthop J Sports Med. 2019; 7 (suppl 3): doi: 10.1177/2325967119S00139
- Rodriguez M, Bolia IK, Philippon MD, Briggs KK, Philippon MJ. Hip Screening of a Professional Ballet Company Using Ultrasound-Assisted Physical Examination Diagnosing the At-Risk Hip. J Dance Med Sci. 2019;23(2):51-57. doi:10.12678/1089-313X.23.2.51
- Harris JD, Gerrie BJ, Varner KE, et al. Radiographic Prevalence of Dysplasia, Cam, and Pincer Deformities in Elite Ballet. Am J Sports Med. 2016;44(1):20-27. doi:10.1177/0363546515601996
- Coleman SH. Editorial Commentary: “Dancing the Hip Away.” Arthroscopy. 2019;35(4):1109-1110.
- Mayes S, Smith P, Cook J. Impingement-type bony morphology was related to cartilage defects, but not pain in professional ballet dancers’ hips. J Sci Med Sport. 2018;21(9):905-909.
- Bolia I, Utsunomiya H, Locks R, et al. Twenty-Year Systematic Review of the Hip Pathology, Risk Factors, Treatment, and Clinical Outcomes in Artistic Athletes—Dancers, Figure Skaters, and Gymnasts. Clin J Sport Med. 2018;28(1):82-90.
- Ukwuani GC, Waterman BR, Nwachukwu BU, et al. Return to Dance and Predictors of Outcome After Hip Arthroscopy for Femoroacetabular Impingement Syndrome. Arthroscopy. 2019;35(4):1101-1108.e3.
- Putko R, Safran M. Managing the Hip in Supraphysiologic Motion Athletes. Oper Tech Sports Med. 2024;32(3).
- Hammoud S, Bedi A, Voos JE, Mauro CS, Kelly BT. The recognition and evaluation of patterns of compensatory injury in patients with mechanical hip pain. Sports Health. 2014;6(2):108-118. doi:10.1177/1941738114522201
- Curley AJ, Engler ID, McClincy MP, Mauro CS. Hip Pain in Ballet Dancers: Evaluation and Management. J Am Acad Orthop Surg. 2022;30(23):1123-1130. doi:10.5435/JAAOS-D-22-00528
- Nolton EC, Ambegaonkar JP. Recognizing and Managing Snapping Hip Syndrome in Dancers. Med Probl Perform Art. 2018;33(4):286-291. doi:10.21091/mppa.2018.4042
- Laible C, Swanson D, Garofolo G, Rose DJ. Iliopsoas Syndrome in Dancers. Orthop J Sports Med. 2013;1(3):2325967113500638. Published 2013 Aug 21. doi:10.1177/2325967113500638
- Sobrino FJ, de la Cuadra C, Guillén P. Overuse Injuries in Professional Ballet: Injury-Based Differences Among Ballet Disciplines. Orthop J Sports Med. 2015;3(6):2325967115590114. Published 2015 Jun 26. doi:10.1177/2325967115590114
