
John P. Walsh, DO1; Taylor Anthony, DO1; Benjamin Moyer, DO1; Keith Kotecki, DO2
1Valley Hospital Medical Center
2Nevada Orthopedic and Spine
DOI: http://doi.org/10.70709/gxiv50on8u3zpl
ABSTRACT
Complex primary total knee arthroplasty (TKA) with bone loss may benefit from robotic assistance. We describe a stepwise technique for image-based robotic arm-assisted primary TKA (MAKO system) with femoral augmentation. Preoperative CT planning characterizes bone defects and guides augment preparation. Intraoperatively, the femoral component position is proximalized in the planning software to “trick” the robot into precise lateral distal femoral cuts, maintaining robotic precision throughout. This technique was successfully applied for lateral distal femoral condyle bone loss requiring a 10 mm augment, enabling real-time gap balancing, and eliminating conventional revision instruments. Image-based robotic-assisted TKA can be adapted for complex primary cases requiring femoral augmentation, leveraging robotic precision to address bone defects while maintaining procedural efficiency and accuracy.
Keywords: Total Knee Arthroplasty, Robotic-Assisted, Femoral Augmentation, Computer-Assisted, Bone Defect, Surgical Technique
Level of Evidence: V
Introduction
Primary total knee arthroplasty (TKA) is a safe, durable, and cost-effective procedure with favorable long-term outcomes.(1-3) TKA failure has been attributed to surgeon, patient, and implant-related factors.(4,5) From the surgeon’s perspective, the most important variables are modifiable technical factors.(6-8)
One modality to improve technical performance is robotic-assisted TKA (rTKA).(9) There is a rich body of literature describing improved alignment and reduced revision rate with rTKA relative to conventional TKA (cTKA), though clinical outcome data are less conclusive.(10-12) Notably, rTKA may be cost-effective in specific clinical settings.(13) We posit that complex primary TKA procedures present a unique opportunity to implement rTKA to overcome intraoperative technical challenges.
Several studies have described robotic systems for femoral and tibial bone preparation, yet a gap exists regarding complex primary rTKA.(14-16) The MAKO Robotic Arm Interactive Orthopedic System (Stryker, Kalamazoo, MI) has system-specific data supporting safety and accuracy.(17,18) While rTKA has demonstrated improved accuracy in implant positioning and soft tissue protection, managing bone defects requiring augmentation presents unique challenges.
Complex primary TKA conveys that specific preoperative factors suggest the procedure will be more technically challenging.(19) Such factors include exposure challenges, anatomic landmark loss, instability, and bone loss.(20,21) This technical note presents a stepwise technique for rTKA with bone loss requiring augments, eliminating the need for conventional revision instrumentation while maintaining robotic precision throughout.
Surgical Technique
Preoperative Planning: When using image-based robotic arm-assisted TKA (MAKO), the procedure is initiated preoperatively with CT-based planning.(22,23) The robotic system requires a MAKO CT protocol for segmentation and planning. The 3D CT model enables evaluation of lateral femoral condyle bone loss noted on preoperative radiographs (Figure 1), portending a more technically challenging procedure. The model enables preoperative planning of initial bony resections and estimation of bone defect location and size, ensuring required augment inventory is available on the day of surgery. Preoperative templating should be performed in standard fashion,(24,25) facilitated by the 3D model.

Patient Positioning and Exposure: Once indicated for surgery and informed consent obtained, the patient is placed supine on the operative table, a tourniquet is applied to the operative extremity, and the site is prepped and draped in a sterile fashion. A midline incision is planned in flexion, two fingerbreadths superior to the patella, ending 3-4 cm distal to the joint line on the anteromedial tibia for a standard medial parapatellar approach. The robotic system only recognizes bone tissue(26); surgeons must remain cognizant of adjacent soft tissues that may be damaged by the saw blade.
Array Pin Placement and Registration: Following exposure, array pins are placed. The femoral pin is an intra-incisional, intracapsular array pin angled anteromedially into the distal femur at approximately 45°; it must not interfere with anterior or chamfer cut saw paths. The tibial pin is inserted through stab incisions along the anteromedial tibial shaft, distal to the joint line with sufficient space to avoid implant overlap (e.g., ≥130 mm distal for a 100-mm stem). Distal placement allows retention of robotic arrays throughout the entire procedure. Array loosening before resection is addressed by re-registration; after resection initiation, accuracy will be diminished. Place checkpoints far from resection planes to avoid inadvertent resection. The femoral checkpoint is optimally placed at the medial epicondyle prominence for bone quality. Registration follows MAKO protocols using the robotic-guided probe. Remove all osteophytes before gap measurements. Apply light touch during probe registration to avoid penetrating soft cartilage. Registration establishes the tibial axis using the medial and lateral malleoli and tibial knee center. The hip center is established through conical range-of-motion mapping. Femoral rotation should be manually defined due to potential differences between component position and standard references. Intraoperative gap-balance planning follows, including varus/valgus stress testing, to set rotation, position, and resection level for a symmetric flexion-extension arc.
Augment Preparation — The “Trick” Technique: Initial femoral and tibial bone cuts are performed per the MAKO plan, ignoring the area of bone defect, which has already been characterized preoperatively. In the current case, there was no lateral distal femoral cut with a residual 7 mm bone deficit following the preliminary cut. The surgeon then returns to the intraoperative planning screen and proximalizes the implant plan by 10 mm, “tricking” the robot into making a 3 mm lateral distal femoral bone cut to accommodate the 10 mm augment (Figure 2). The augment location is defined on the CT-based model and confirmed using the probe. Always re-validate checkpoints before activating the blade saw, especially following plan adjustments. The robotic arm saw is then used for precise augment resection. Surgeons must recognize that the robot plan corresponds to the implant footprint and will not restrict resection to the augmentation zone; surgeon vigilance is essential to limit resection to the confirmed augment site.

Trialing, Box Cut, and Implantation: Trial components (including augment and stem if used) are placed and limb alignment and soft tissue balance are assessed using the MAKO system’s real-time gap analysis (Table 1). Stability is assessed through a full arc of flexion-extension. Tibial rotation is confirmed and marked with electrocautery. Preparations are then made for the box cut; this technique requires posterior-stabilized implants. The box cut is planned with the robotic 3D model and probe; arrays are maintained. Patellar tracking is manually assessed. Following box cut, trial components are removed. If stems are used, cement restrictors are placed 1 cm from planned implant length (stems were not used in the current case). Bony surfaces are irrigated and dried; cement is vacuum mixed, pressurized, and applied. Construct stability is reassessed after cement cure, excess cement removed, and the final polyethylene liner inserted and locked. The knee is irrigated with dilute betadine and normal saline. Final alignment and balance are captured by the robotic software. Arrays and pins are removed, confirming no hardware failure.
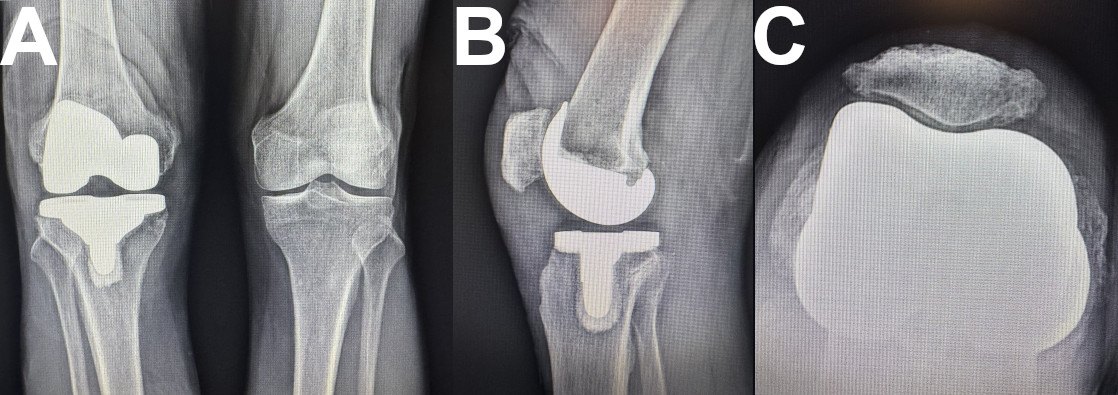
Wound Closure: Capsular closure is performed with interrupted #1 Ethibond and #1 Vicryl, followed by running #1 Stratafix. Knee range of motion and patellar tracking are assessed. Subcutaneous fat is closed with running 0 Vicryl; subcutaneous tissue with interrupted 2-0 Vicryl; skin with running 3-0 Monocryl and Dermabond. Pin sites are closed with Monocryl and Dermabond. Postoperative radiographs confirm adequate component positioning (Figure 3).
| Pearls | Pitfalls |
| Insert array pins distally and at proper angle to avoid interference with saw paths and stem | Array pin loosening, poor fixation, or malposition can compromise registration accuracy |
| Mark retinaculum before arthrotomy to facilitate anatomic closure | Movement artifact or power supply issues can disrupt MAKO system functioning |
| Register anatomical points gently, especially in cartilage-deficient regions | Poor registration leads to alignment errors and loss of robotic advantages |
| Use trial augment and real-time robotic feedback before committing to final resection | Robotic system does not recognize soft tissue: prevent iatrogenic ligament or tendon injury |
| Retain array pins as long as possible during stem preparation for ongoing monitoring | Initial cases may require longer operative time due to the learning curve |
| Plan and confirm augment options and inventory preoperatively | Limited implant compatibility — ensure all required inventory is present before starting |
| Mark epicondyles during registration to help visualize femoral rotation relative to whiteside line and transepicondylar axis | Not accounting for tibial baseplate size differences when placing array pins |
Table 1: Pearls and Pitfalls of Image-Based Robotic Arm-Assisted TKA with Femoral Augmentation
Discussion
We present a stepwise technique for primary TKA with femoral augmentation using an image-based robotic arm-assisted system. Complex primary TKA presents a unique opportunity to apply the advantages of rTKA in a technically demanding setting, leveraging robotic precision to mitigate risk and optimize outcomes.
To our knowledge, only one prior surgical technique has been described for rTKA with robotically guided augment placement.(15) Similar to that report, our technique integrates robotic precision with complex reconstruction needs. Our approach, however, is specifically adapted to preserve multiple resection plans required for distal femoral preparation. The prior technique addressed tibial augmentation, which requires navigating only one prior cut, with a supplemental freehand or osteotome vertical cut. Our technique is versatile and maintains standard robotic workflow throughout. Robotic platforms will continue to evolve, and expansion to revision instrumentation may further enhance utility in complex reconstruction.(14,16)
Not all rTKA systems are equivalent. The MAKO system is FDA-approved for primary TKA only, whereas imageless systems (CORI, Smith & Nephew) may be used in both primary and revision settings. Our technique enables complex primary TKA without revision instrumentation. Preoperative CT facilitated quantification of bone loss, accurate preoperative planning, and appropriate implant inventory management, mitigating logistical demands on the day of surgery. Analogous to reports of rTKA improving outcomes in unicompartmental-to-TKA conversion,(18) we surmise complex primary rTKA may offer similar benefits. Early data support improved functional outcomes with rTKA over cTKA.(27) Future studies should assess whether complex primary rTKA improves patient satisfaction or component survival.
Disadvantages of rTKA including increased operative time, learning curves, and costs are well-documented.(14,18) Potential complications unique to robotic systems include pin-site complications, with reported rates of 1.4% for pin-site complications and 0.06-4.8% incidence of periprosthetic fracture through pin sites.(28,29) Pin size may affect fracture risk.(29,30) These complications are uncommon but require a high index of suspicion for timely diagnosis and management.
Limitations of this report include its descriptive nature and absence of objective clinical outcome data. A comparative investigation is required to establish clinical significance, which represents an important area for future study.
We present a stepwise technique for primary total knee arthroplasty with femoral augmentation using an image-based robotic arm-assisted system. This approach maintains robotic precision throughout, eliminates the need for conventional revision instrumentation, and may optimize surgical accuracy, component placement, and reproducibility in complex primary TKA.
References
- Murray DW, MacLennan GS, Breeman S, et al. A randomised controlled trial of the clinical effectiveness and cost-effectiveness of different knee prostheses: the Knee Arthroplasty Trial (KAT). Health Technol Assess. 2014;18(19). doi:10.3310/hta18190
- Courtney PM, Howard M, Goyal N, Schwarzkopf R, Schnaser E, Sheth NP. How much do patients value total hip and knee arthroplasty? A prospective, multicenter study. J Arthroplasty. 2016;31(3):562-566.e3. doi:10.1016/j.arth.2015.10.008
- Price AJ, Alvand A, Troelsen A, et al. Knee replacement. The Lancet. 2018;392(10158):1672-1682. doi:10.1016/S0140-6736(18)32344-4
- Lombardi AV, Berend KR, Adams JB. Why knee replacements fail in 2013: patient, surgeon, or implant? Bone Jt J. 2014;96-B(11 Supple A):101-104. doi:10.1302/0301-620X.96B11.34350
- Gunaratne R, Pratt DN, Banda J, Fick DP, Khan RJK, Robertson BW. Patient dissatisfaction following total knee arthroplasty: a systematic review of the literature. J Arthroplasty. 2017;32(12):3854-3860. doi:10.1016/j.arth.2017.07.021
- Aoki SK. Editorial commentary: patient profiling — identifying risk factors that help predict outcomes of hip arthroscopy candidates. Arthrosc J Arthrosc Relat Surg. 2019;35(11):3057-3059. doi:10.1016/j.arthro.2019.07.011
- Aalen OO, Valberg M, Grotmol T, Tretli S. Understanding variation in disease risk: the elusive concept of frailty. Int J Epidemiol. 2015;44(4):1408-1421. doi:10.1093/ije/dyu192
- Andersen PK, Geskus RB, de Witte T, Putter H. Competing risks in epidemiology: possibilities and pitfalls. Int J Epidemiol. 2012;41(3):861-870. doi:10.1093/ije/dyr213
- Riantho A, Butarbutar JCP, Fidiasrianto K, et al. Radiographic outcomes of robot-assisted versus conventional total knee arthroplasty: a systematic review and meta-analysis of randomized clinical trials. JBJS Open Access. 2023;8(2):e23.00010. doi:10.2106/JBJS.OA.23.00010
- Kim YH, Yoon SH, Park JW. Does robotic-assisted TKA result in better outcome scores or long-term survivorship than conventional TKA? A randomized, controlled trial. Clin Orthop. 2020;478(2):266-275. doi:10.1097/CORR.0000000000000916
- Kort N, Stirling P, Pilot P, Müller JH. Robot-assisted knee arthroplasty improves component positioning and alignment, but results are inconclusive on whether it improves clinical scores or reduces complications and revisions: a systematic overview of meta-analyses. Knee Surg Sports Traumatol Arthrosc. 2022;30(8):2639-2653. doi:10.1007/s00167-021-06472-4
- Batailler C, White N, Ranaldi FM, Neyret P, Servien E, Lustig S. Improved implant position and lower revision rate with robotic-assisted unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1232-1240. doi:10.1007/s00167-018-5081-5
- Rajan PV, Khlopas A, Klika A, Molloy R, Krebs V, Piuzzi NS. The cost-effectiveness of robotic-assisted versus manual total knee arthroplasty: a Markov model-based evaluation. J Am Acad Orthop Surg. 2022;30(4):168-176. doi:10.5435/JAAOS-D-21-00309
- Mancino F, Jones CW, Benazzo F, Singlitico A, Giuliani A, De Martino I. Where are we now and what are we hoping to achieve with robotic total knee arthroplasty? A critical analysis. Orthop Res Rev. 2022;14:339-349. doi:10.2147/ORR.S294369
- Hulse N. Robotic arm-assisted augment preparation (RAAP-technique) during total knee arthroplasty. Arthroplasty Today. 2025;33:101725. doi:10.1016/j.artd.2025.101725
- Bautista M, Manrique J, Hozack WJ. Robotics in total knee arthroplasty. J Knee Surg. 2019;32(7):600-606. doi:10.1055/s-0039-1681053
- Casper M, Mitra R, Khare R, et al. Accuracy assessment of a novel image-free handheld robot for total knee arthroplasty in a cadaveric study. Comput Assist Surg. 2018;23(1):14-20. doi:10.1080/24699322.2018.1519038
- Sousa PL, Sculco PK, Mayman DJ, Jerabek SA, Ast MP, Chalmers BP. Robots in the operating room during hip and knee arthroplasty. Curr Rev Musculoskelet Med. 2020;13(3):309-317. doi:10.1007/s12178-020-09625-z
- Shah SM, Sciberras NC, Allen DJ, Picard F. Technical and surgical causes of outliers after computer navigated total knee arthroplasty. J Orthop. 2020;18:171-176. doi:10.1016/j.jor.2019.10.016
- Dennis DA. A stepwise approach to revision total knee arthroplasty. J Arthroplasty. 2007;22(4 Suppl 1):32-38. doi:10.1016/j.arth.2007.01.001
- Dennis DA, Berry DJ, Engh G, et al. Revision total knee arthroplasty. J Am Acad Orthop Surg. 2008;16(8):442-454. doi:10.5435/00124635-200808000-00003
- Yohe N, Mont MA, Chen Z, Sultan AA. MAKO robotic-arm assisted total knee arthroplasty: surgical technique from the office to the operating room. Surg Technol Int. 2021;39:375-385. doi:10.52198/21.STI.39.OS1474
- Roche M. The MAKO robotic-arm knee arthroplasty system. Arch Orthop Trauma Surg. 2021;141(12):2043-2047. doi:10.1007/s00402-021-04208-0
- Preoperative knee templating accuracy does not predict radiographic or clinical outcome in total knee arthroplasty. Orthopedics. Accessed September 23, 2025. https://journals.healio.com/doi/10.3928/01477447-20250813-01
- Tiefenboeck S, Sesselmann S, Taylor D, Forst R, Seehaus F. Preoperative planning of total knee arthroplasty: reliability of axial alignment using a three-dimensional planning approach. Acta Radiol. 2022;63(8):1051-1061. doi:10.1177/02841851211029076
- Dretakis K, Koutserimpas C. Pitfalls with the MAKO robotic-arm-assisted total knee arthroplasty. Medicina (Mex). 2024;60(2):262. doi:10.3390/medicina60020262
- Kayani B, Konan S, Tahmassebi J, Pietrzak JRT, Haddad FS. Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty. Bone Jt J. 2018;100-B(7):930-937. doi:10.1302/0301-620X.100B7.BJJ-2017-1449.R1
- Smith TJ, Siddiqi A, Forte SA, et al. Periprosthetic fractures through tracking pin sites following computer navigated and robotic total and unicompartmental knee arthroplasty: a systematic review. JBJS Rev. 2021;9(1):e20.00091. doi:10.2106/JBJS.RVW.20.00091
- Thomas TL, Goh GS, Nguyen MK, Lonner JH. Pin-related complications in computer navigated and robotic-assisted knee arthroplasty: a systematic review. J Arthroplasty. 2022;37(11):2291-2307.e2. doi:10.1016/j.arth.2022.05.012
- Desai SS, Kunes JA, Held MB, et al. A comparison of pin site complications between large and small pin diameters in robotic-assisted total knee arthroplasty. J Exp Orthop. 2023;10:22. doi:10.1186/s40634-023-00584-1
