
Laura M. Maharjan, DO; Victor D. Bonavida, DO; and Ashley Lamb, DO
Community Memorial Hospital
DOI: http://doi.org/10.70709/d7h5fgjys
Abstract
Intra-articular injury to the knee can have numerous sequelae, one being an acutely locked knee. A patient suffering from this pathology will have pain, mechanical symptoms, and decreased range of motion in the sagittal plane. Different causes can lead to the resulting locked knee; however, it is commonly seen after bucket handle tearing of either meniscus. A locked knee may lead to an osteochondral defect and subsequent degeneration, predisposing patients to early osteoarthritis. As a result of this anatomical and biomechanical limitation in these patients, surgical management is often indicated. In this case report, we explore the possibility of using an Osteopathic manipulative technique as a possible therapy to “unlock” the knee and avoid surgery.
Keywords: Case report, locked knee, OMM, OMT, meniscus
Introduction
A locked knee occurs when a sudden decrease in the range of motion, and the patient cannot bend or straighten the knee. These episodes may be short or longer-lasting depending on the cause. The etiology of a locked knee can be due to a mechanical cause, or a mechanism called a pseudo-locked knee can be seen as caused by pain from degenerative causes such as arthritis or muscle spasms. The most common mechanical cause of locked knees is a bucket-handle tear of the meniscus. Other well-described mechanical causes of locked knees include the formation of loose bodies from bony fragments, osteochondral defects, fractures, arthritic lesions, and plica syndrome. Typically, the fragments become fixed within the joint between the articular surface of the tibial plateau and the femoral condyles upon extension of the knee, thereby limiting motion at the joint. As a result of this pathological and biomechanical process, almost all patients will have had prior knee injury or trauma. Exam findings on these patients usually exhibit joint line tenderness with possible effusion. MRIs traditionally have been used to help differentiate between actual locking and pseudo-locking knees. 1,2
Muscle Energy
A core osteopathic modality is muscle energy technique (MET), which utilizes the muscle’s inherent actions and physiology to induce a response in either an agonistic or an antagonist manner. Traditionally, the method is accomplished by:
- Positioning the patient’s joint at the restrictive barrier
- Having the patient generate an isometric contraction against the provider’s counterforce
- Maintaining the contraction for 3-5 seconds before relaxation.
- Repositioning the joint into the new barrier, allowing for progressive improvement in range of motion
Physiologically, MET is based on two primary mechanisms: post-isometric relaxation and reciprocal inhibition. Post-isometric relaxation is thought to occur through activation of Golgi tendon organs, which sense tension during an isometric contraction and trigger reflex inhibition of the contracted muscle, allowing it to lengthen upon relaxation. In contrast, reciprocal inhibition, as described by Sherrington’s Law, involved the reflex relaxation of antagonist muscles when the agonist muscle contracts 3, 4In certain situations, a modification to this basic principle can be applied. For example, In a patient restricted in knee flexion, contraction of the quadriceps (agonist) facilitates relaxation of the hamstrings (antagonist), enhancing joint motion through reciprocal inhibition 4.
From a biomechanical perspective, MET integrates neural reflexes and gentle mobilization forces which influence joint mechanics through repeated low intensity contractions which not only reset aberrant proprioceptive input from muscle spindles but also mobilize periarticular tissues within their physiologic range 4. The origins of MET can be traced to the work of Fred L. Mitchell, Sr., DO in the mid-20th century, whose foundational writings established its clinical rationale within osteopathic manipulative medicine (OMM). Subsequent studies have validated MET’s effectiveness in improving range of motion, reducing hypertonicity, and enhancing biomechanics 5-7. T
Case
History and Physical
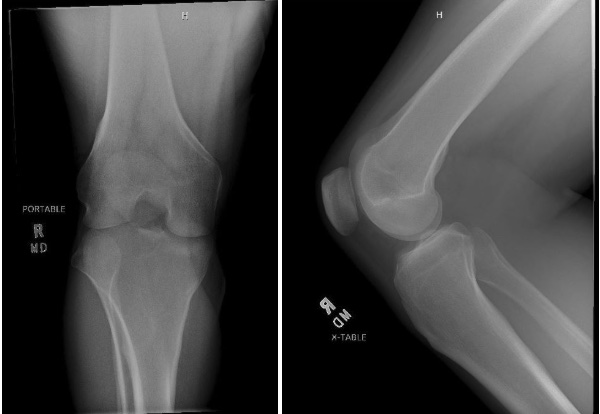
A 31-year-old male who presented to the emergency department for evaluation of right knee pain and inability to extend his knee with similar episodes prior. He was in a squatted position when he felt a snap and felt the knee lock with the inability to extend back to neutral. X-Rays were normal, but he remained unstable to extend despite medication
On a physical exam, the right knee was flexed, and it could not extend past 90 degrees. He was motor and sensory intact throughout and could move all extremities spontaneously. He was neurovascularly intact. Of note, he had hypertonicity of the hamstrings.
Initial Imaging
ED Treatment
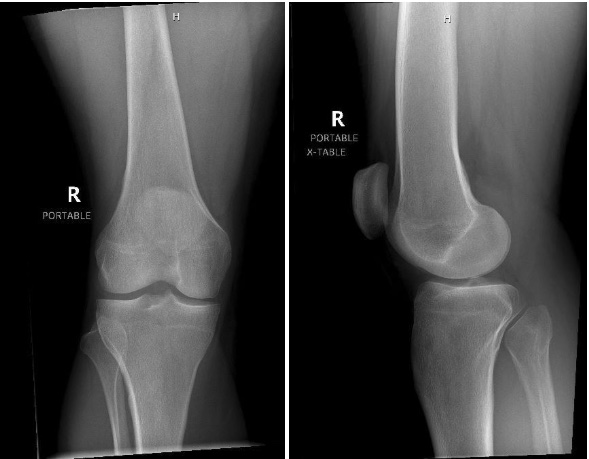
The osteopathic manipulative technique of muscle energy, employing reciprocal inhibition, involved carefully positioning the hamstring just short of causing discomfort. The patient was then instructed to engage their quadriceps by extending their leg toward the provider and performing an isometric contraction. Subsequently, as the patient exhaled and relaxed, the hamstring was gently stretched to a new limit. This procedure was repeated five more times until full extension was successfully achieved.
Following this, the patient’s knee was securely immobilized using a knee brace, and a new XR was obtained. New XR obtained post treatment as seen in Figure 2.
After successful osteopathic manipulative treatment, an MRI was ordered for further evaluation, which was completed in the outpatient setting within the week. MRI revealed a bucket-handle lateral meniscus tear with an associated large joint effusion (refer below). No additional ligament tear or chondral displacement was seen.
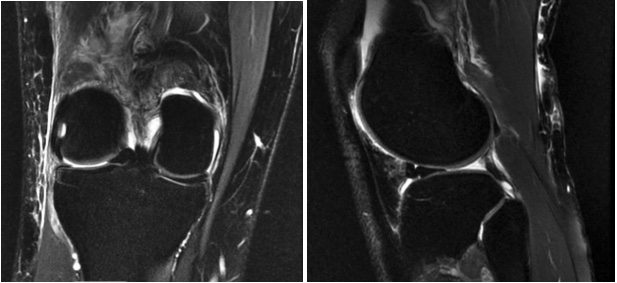
Intervention with arthroscopic partial lateral meniscectomy to address the chronic bucket-handle lateral meniscus tear was recommended and scheduled.
A comprehensive arthroscopic examination confirmed the presence of a bucket-handle tear in the mid-body of the lateral meniscus. The anterior cruciate ligament (ACL), medial meniscus, articular surface of the patellofemoral joint, femoral condyles, and tibial plateaus were all intact. The meniscus tear was meticulously debrided to a stable base during the procedure. Portals were closed in the usual fashion, local anesthesia with epinephrine was injected into the joint, and a soft compressive dressing was applied.
Outcome and Follow-Up
During the post-operative follow-up, the patient demonstrated good progress with the ability to walk without the need for any assistive devices, and demonstrated pain free full range of motion
Discussion
Locking knees can develop acutely, and when it does, it can cause significant pain and limitation in someone’s daily life. Most commonly, these symptoms occur due to intra-articular pathology of the knee. For example, meniscal tears, ligamentous injuries, and intra-articular free bodies.8Additionally, various tumors, hemangiomas, gout, lipomas, or intramuscular ganglion cysts can also cause locking knees, although they are much less common. 9-11
There is a wide range of differentials when considering knee pain. These diagnoses could include osteoarthritis, Osgood-Schlatter, patellofemoral syndrome, iliotibial band syndrome, and many more. As a result, it is crucial to obtain and perform a thorough history and physical exam. Also, imaging can help support the diagnosis of the condition that may be causing intra-articular knee pathology, leading to acute episodes of locking the knee. The above diagnosis in our patient was reached based on the patient’s clinical history, physical exam, and radiographic impression.
Meniscal tears can lead to mechanical symptoms such as catching and locking, pain, and instability. Depending on the severity of these tears, individuals may also experience a limited range of motion, an inability to fully extend the knee, or prolonged episodes of knee joint locking. Meniscus tears can arise from acute incidents and chronic degenerative changes within the tibiofemoral joint space. Regardless of the timing of the injury, patients tend to exhibit symptoms similar to those mentioned earlier. Additionally, they may present with joint effusion, tenderness along the anteromedial or anterolateral joint line, altered gait patterns, and discomfort during deep flexion (squatting). Furthermore, positive findings on the McMurray’s and Thessaly tests may be observed on the affected side.12
In the specific case we encountered, the patient presented with a locked knee that failed straightening attempts by other emergency department providers. Utilizing osteopathic principles and techniques allowed us to safely reduce the patient’s knee with minimal discomfort.
Due to staffing limitations, we could not obtain an MRI in the acute setting. An MRI was obtained in the outpatient setting 6 days after the patient’s presentation to the emergency department and successful “unlocking” of the knee. Therefore, we can only ascertain from a close follow-up MRI that the locked knee presentation was due to a bucket-handle meniscus tear.
Conclusion
In conclusion, the presented case highlights the potential utility of OMM, particularly the muscle energy technique, as an effective intervention for patients presenting with acutely locked knees. In this instance, the successful reduction of the locked knee, followed by MRI confirmation of a bucket-handle tear of the lateral meniscus, highlights the valuable diagnostic and therapeutic role that osteopathic manipulative techniques may play in the acute clinical setting.
A review of the current literature revealed no published studies specifically examining the use of OMM or osteopathic manipulative treatment (OMT) in the management of bucket-handle meniscus tears, either prior to surgical intervention or with documented postoperative outcomes. This absence of evidence emphasizes the novelty of the present case and underscores the need for future research exploring the role of OMT in meniscal injuries and related orthopedic conditions. Evidence from other musculoskeletal and perioperative contexts such as knee osteoarthritis and postoperative rehabilitation suggests potential benefits of OMT in improving function and reducing pain, supporting its consideration as an adjunctive, non-invasive therapeutic option.
Broader integration of OMT within orthopedic and sports medicine practice may be facilitated through continued research, interdisciplinary collaboration, and appropriate coding and billing pathways that support its use in outpatient settings. Further studies are warranted to establish standardized treatment protocols, evaluate patient outcomes, and clarify the mechanisms by which OMT may contribute to musculoskeletal recovery and function within orthopedic care.
References
- Mohd Miswan MF, Latiff Alsagoff S, Muhamad Effendi F, Ibrahim MI. The unusual traumatic locked young knee. Malays Fam Physician. 2019 Aug 31;14(2):26-28. PMID: 31827732; PMCID: PMC6818690.
- FOM IV, Seffinger MA, executive ed., Foundations of Osteopathic Medicine. 4e Philadelphia, PA: Wolters, Kluwer; 2018: pp. 797-812
- Waxenbaum JA, Woo MJ, Lu M. Physiology, Muscle Energy. [Updated 2024 Jan 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559029/
- Fryer G. “Muscle energy technique: an evidence-informed approach.” Int J Osteopath Med. 2011;14(1):3–9.
- Shirodkar, Kapil; Ariyaratne, Sisith; Gavvala, Sai Niharika; Jenko, Nathan; Iyengar, Karthikeyan P.1; Botchu, Rajesh. Understanding Locked Knees: A Comprehensive Analysis of Causative Pathologies. Journal of Arthroscopy and Joint Surgery 12(2):p 88-92, Apr–Jun 2025. | DOI: 10.4103/jajs.jajs_31_24
- Banerjee SB, Mukhi S. Immediate Effect of Non Ballistic Active Knee Extension in Neural Slump Position Versus Muscle Energy Technique on Hamstring Flexiblity in Young Adults-Comparitive Study. Indian Journal of Physiotherapy & Occupational Therapy. 2020;14(3):245-252. doi:10.37506/ijpot.v14i3.9703
- Kalidhasan S, Kotteeswaran K, J. P. AA, Manickavasagam I. Effectiveness of Muscle Energy Technique and Strengthening Exercises by KOOS in Knee Osteoarthritis Strengthening Exercise in Reducing Pain to Improve Functional Activity Measured by KOOS in Knee Osteoarthritis. Indian Journal of Physiotherapy & Occupational Therapy. 2024;18:574-580. doi:10.37506/78vcac66
- Allum RL, Jones JR. The locked knee. Injury. 1986 Jul;17(4):256-8. doi: 10.1016/0020-1383(86)90231-7. PMID: 3770920.
- Tzurbakis M, Mouzopoulos G, Morakis E, Nikolaras G, Georgilas I. Intra-articular knee haemangioma originating from the anterior cruciate ligament: a case report. J Med Case Rep. 2008;2:254
- Sakti M, Usman MA, Lee J, Benjamin M, Maulidiah Q. Atypical musculoskeletal manifestations of gout in hyperuricemia patients. Open Access Rheumatol. 2019;11:47–52
- Kim H, Shin DC, Lee KS, Jang IT, Lee K. Localized pigmented villonodular synovitis with hemorrhage arising from lateral meniscocapsular junction: A case report. Eklem Hastalik Cerrahisi. 2019;30:177–181
- Raj MA, Bubnis MA. Knee Meniscal Tears. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431067/
