
Dr. Alyssa Kendrick, DO and Dr. Toomas Anton, MD
Western Reserve Hospital
DOI: http://doi.org/10.70709/3q7cb6bq4
Abstract
Case
A 69 year old male presented six years postoperatively from an Anterior Cervical Discectomy and Fusion with neck pain, difficulty swallowing, weakness holding his head up, and bilateral hand numbness. Xray and a swallow study demonstrated multi-level screw loosing and complete screw extrusion into esophageal tissues. The patient underwent a revision with both the spine team and the otolaryngology team to ensure safe removal of the screw and other instrumentation. Postoperative swallow studies demonstrated no leaking of contents, and the patient was advanced to a regular diet without complications.
Conclusion
ACDF screw extrusion into esophageal tissues, although rare, is not impossible. It can produce complications including esophageal rupture, infection, and instability. Utilizing swallow studies pre- and post-operatively can help determine the extent of screw extrusion. The primary surgeon should also consult other team members such as otolaryngology for assistance to create the most conducive environment for patient success.
Keywords: ACDF, screw, esophagus, extruded, instrumentation, complication
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
A Case Report
Revision of Anterior Cervical Discectomy and Fusion with Instrumentation Removal from Esophageal Tissue, A Multi-Disciplinary Approach
Introduction
This case discusses a multidisciplinary approach to revision of an anterior cervical discectomy and fusion (ACDF) failure that had associated instrumentation extrusion into esophageal tissues. There are only a small number of case reports involving this delayed complication. A recent small, single-institution case series reported an incidence for pharyngoesophageal damage from ACDF instrumentation extrusion of 0.22% and a delay averaging seven and a half years to presentation from the initial surgery (1). A handful of management techniques have been reported as well but there is no standard protocol. Some cases have involved the otolaryngology team, and others have involved a cardiothoracic team (2). A select few cases have even reported oral or fecal extrusion of instrumentation components (3, 4, 5, 6). Patients who experience screw back out or extrusion are at risk for not only local nerve and tissue damage in addition to spinal instability, but they are also at risk for life-threatening infection due to perforation of esophageal tissues and leakage of contents.1 It is crucial that this topic is brought to the forefront to promote early recognition and congruent management of care.
Informed Consent
The information presented in this case report was gathered with the utmost care to protect patient confidentiality and identity. Patient consent was obtained for educational purposes with risks and benefits discussed.
Case Report
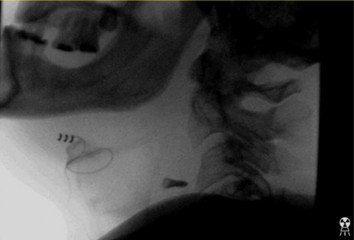
This case is centered around a 69-year-old Caucasian male who presented six and a half years status-post ACDF at the levels of C4-C7 from an outside facility. His main symptoms began six months prior to presentation and included neck pain, difficulty swallowing, weakness holding his head up, and bilateral hand numbness. X-ray imaging demonstrated a screw that had backed out on the left side of C4 and was now residing in soft tissues in addition to right sided multi-screw loosening (Figures 1,2). Additionally, a preoperative swallow study was obtained to evaluate esophageal tissue involvement. This demonstrated a loose screw that rose and fell with esophageal tissue (Figures 3, 4).



The patient elected to proceed with surgery for anterior cervical instrumentation removal and posterior instrumentation placement at C3-T2. Intraoperatively, when the time came to remove the screw closest to the esophagus, the otolaryngology surgical team was actively involved in the operative suite. They inspected for mucosal violation both with and without a nasogastric tube once the screw had been removed. The patient did not require an esophageal repair. The remainder of the anterior instrumentation was removed. Posterior instrumentation was placed at C3-T2 (figures 5-7).



A postoperative swallow study was performed demonstrating no esophageal leaks, and slow advancement of diet was well tolerated. Both teams followed the patient postoperatively to ensure that the patient was swallowing well. There were no intraoperative or immediate postoperative complications within a 3-month follow-up.
Discussion
In summary, it is highly advised providers bear in mind this unique postoperative complication and even consider educating patients on the risk of ACDF instrumentation extrusion. Doing so could prompt patients to present to the office sooner if symptoms arise even after years following an uncomplicated ACDF procedure. Earlier presentation allows the problem to be addressed before further serious complications such as esophageal perforation, infection, and instability result. Utilization of multimodal imaging strategies was essential in this case. The use of pre- and postoperative swallow studies helped to determine the severity and integrity of structures that had been affected by the extruded instrumentation. This allowed for better intraoperative planning and consultation arrangements with otolaryngologists for both intraoperative and follow-up assistance. With careful pre- and postoperative management, multimodal imaging techniques, and a multidisciplinary team approach, this patient was provided with a safe care management plan in a unique, complex problem.
References
- Yahanda AT, Pennicooke B, Ray WZ, et al. Pharyngoesophageal Damage from Hardware Extrusion at an Average of 7.5 Years After Anterior Cervical Diskectomy and Fusion: A Case Series, Discussion of Risk Factors, and Guide for Management. World Neurosurg. 2022;160:e189-e198. doi:10.1016/j.wneu.2021.12.110
- Halani SH, Baum GR, Riley JP, et al. Esophageal perforation after anterior cervical spine surgery: a systematic review of the literature. J Neurosurg Spine. 2016;25(3):285-291. doi:10.3171/2016.1.SPINE15898
- Gazzeri R, Tamorri M, Faiola A, Gazzeri G. Delayed migration of a screw into the gastrointestinal tract after anterior cervical spine plating. Spine (Phila Pa 1976). 2008;33(8):E268-E271. doi:10.1097/BRS.0b013e31816b8831
- Geyer TE, Foy MA. Oral extrusion of a screw after anterior cervical spine plating. Spine (Phila Pa 1976). 2001;26(16):1814-1816. doi:10.1097/00007632-200108150-00019
- Kapu R, Singh M, Pande A, Vasudevan MC, Ramamurthi R. Delayed anterior cervical plate dislodgement with pharyngeal wall perforation and oral extrusion of cervical plate screw after 8 years: A very rare complication. J Craniovertebr Junction Spine. 2012;3(1):19-22. doi:10.4103/0974-8237.110121
- Na D, Eom KS. Oral Extrusion of a Screw After Anterior Cervical Spine Plating: A Case Report. Korean J Neurotrauma. 2024;20(3):203-208. Published 2024 Sep 19. doi:10.13004/kjnt.2024.20.e27
