
Grayson Punzalan, OMSIV1; Greg Beato, DO, FACOI2
1Edward Via College of Osteopathic Medicine – Virginia
2Medical Associates of Southwest Virginia, Edward Via College Of Osteopathic Medicine
DOI: http://doi.org/10.70709/g1nl9hbtsk
Abstract
Case
A 47-year-old female with a childhood diagnosis of left-sided melorheostosis presented with chronic right hip, knee, and ankle pain. On examination, right-sided lower extremity shortening of 3/8-inch, restriction of right hip and knee movement, and tenderness to palpation of the lower back. Previous radiographs confirmed dense, irregular cortical hyperostosis and secondary degenerative joint changes. Pain is managed conservatively with occasional NSAID use and activity modification.
Conclusion
Adult orthopedic symptoms in melorheostosis patients often reflect a combination of limb discrepancy, altered biomechanics, and degenerative joint changes. Recognition and monitoring of long-term contralateral joint loading in patients with unilateral skeletal dysplasia remain central in such cases. Surgical correction may improve structural issues, but functional imbalance and pain can persist, requiring comprehensive biomechanical management.
Keywords: Melorheostosis, Leri’s Disease, Leg Length Discrepancy, Hyperostosis
Introduction
Melorheostosis, also known as Leri’s disease, is a rare, progressive sclerosing bone dysplasia with an estimated incidence of 0.9 cases per million individuals (1). It is characterized by segmental cortical hyperostosis that manifests in childhood or adolescence, most commonly affecting the long bones of the appendicular skeleton, typically following a sclerotomal distribution (2). Radiographically, melorheostosis exhibits a distinctive “dripping candle wax” appearance along the cortex, which is pathognomonic, but may be misinterpreted in early or atypical presentations (3). The disease can involve both bone and adjacent soft tissues, frequently leading to chronic pain, joint stiffness, limb deformity, soft tissue contractures, and restricted range of motion (4). Although traditionally considered idiopathic, recent molecular studies have identified somatic activating mutations in the MAP2K1 gene and LEMD3 gene in a subset of patients, suggesting a clinical and genetic heterogeneity among patients (3).
Given its progressive nature and potential for disabling sequelae, proper recognition and orthopedic management are fundamental. Diagnosis is currently based on clinical and radiological features, with typical treatment being often individualized for symptoms and may range from physical therapy or pharmacologic pain control to a corrective osteotomy depending on disease severity and anatomic involvement (3). No standardized therapeutic protocols exist due to the limited number of reported cases and lack of longitudinal data.
While melorheostosis is often managed in pediatric orthopedics, long-term adult outcomes are infrequently described in the literature. Recurrent symptoms in adulthood, including pain and limited mobility, are often due to secondary joint degeneration and biomechanical alterations related to previous surgical interventions.
Statement of Informed Consent
The patient was informed that data concerning the case would be submitted for publication and provided consent.
Case Report
A 47-year-old female presented to her primary care provider with complaints of chronic right-sided hip, knee, and ankle pain. The pain was insidious in onset and described as a dull ache rated a 2/10, accompanied with low back discomfort and intermittent sharp exacerbations, exacerbated by high impact activities and wearing certain types of shoes. She reported first noticing her symptoms in her 20s when she increased physical activity and engaged in frequent long-distance running. She eventually discontinued running due to worsening joint pain and now avoids high impact activities. She remains active and reports needing to be cautious with footwear, as improper shoe support often worsens her symptoms.
The patient was diagnosed with melorheostosis of the left lower extremity at age 3 after evaluations for gait abnormalities. Radiographs at the time showed classic cortical hyperostosis of the left hip, femur, tibia, and ankle. During adolescence, she developed a 3 cm LLD, with the left leg shorter, resulting in compensatory pelvic obliquity and altered gait.
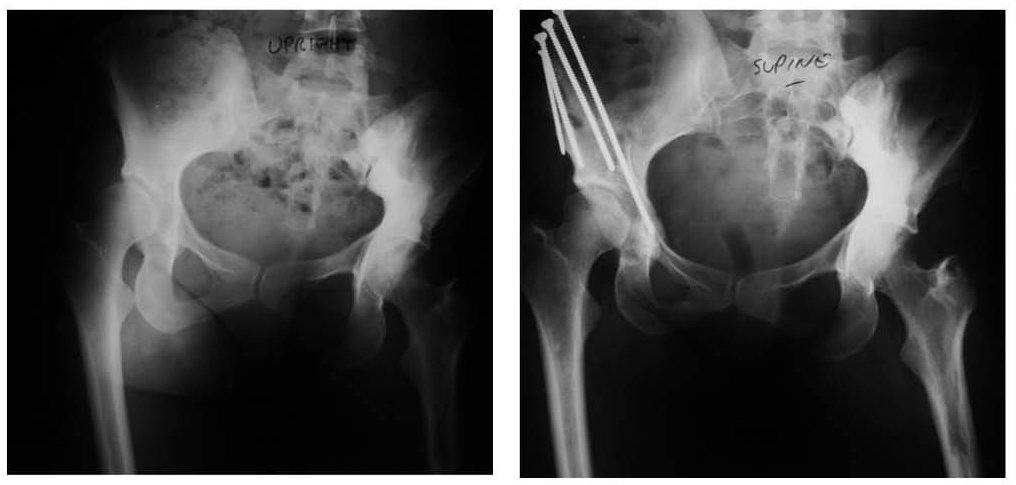
At age 30, she underwent a right periacetabular osteotomy (PAO) to address a symptomatic acetabular dysplasia, followed by a right proximal femoral osteotomy at age 37 for mechanical axis correction (Figure 1 and Figure 2). These surgeries successfully addressed her structural complaints and some of her pain, but she was left with a 3/8-inch shorter right leg.

The patient denies current use of prescription pain medications and orthotics. She takes ibuprofen intermittently when pain flares. No other significant medical history was noted.
On physical examination, she demonstrated a mild pelvic tilt, a right-sided Trendelenburg gait, and tenderness over the greater trochanter and lateral joint line of the right knee. Strength is preserved, and there is no neurovascular compromise. Previous imaging of the right hip showed evidence of post-osteotomy remodeling with mild degenerative changes. The left leg exhibits cortical thickening consistent with chronic melorheostosis (Figures 3, 4, 5).



Given the absence of acute pathology or progressive deformity, the patient was managed conservatively.
Discussion
The unique aspect of this case is the chronic pain in the contralateral limb, the right side, despite melorheostosis being confined to the left leg. This case highlights the long-term biomechanical and orthopedic consequences of a unilateral skeletal dysplasia and the secondary degenerative impact on the contralateral limb.
While melorheostosis is classically described as a localized, sclerosing bone disorder with a benign radiographic appearance, its functional implications, particularly when associated with significant limb length discrepancy, can be profound and progressive. Biomechanical studies confirm that even small LLDs, as little as 1 to 2 cm, can alter pelvic alignment and gait symmetry, leading to compensatory overuse of the unaffected limb (5).
Leg length discrepancy is one of the most common complications in melorheostosis, often resulting from asymmetric endochondral growth and reactive hyperostosis during development. The primary lesions in our patient affected the left lower extremity and led to a 3 cm functional LLD in adolescence and early adulthood. As a compensatory mechanism, the patient shifted weight-bearing to the unaffected right side, resulting in chronic mechanical overload. This overuse contributed to early acetabular dysplasia and joint degeneration in the right hip (6). Over time, this degeneration evolved into a clinical presentation of activity-limiting pain and restricted range of motion.
The decision to proceed with a right periacetabular osteotomy at age 30 was consistent with standard surgical indications for hip dysplasia in young, active patients. PAO is a joint preserving procedure aimed at optimizing femoral head coverage, redistributing weight-bearing forces, and delaying progression to osteoarthritis. In patients with compensatory dysplasia due to long-term asymmetric loading, PAO may be effective, but studies have demonstrated that outcomes can be dependent on the duration of symptoms and underlying biomechanics (7).
Seven years later, the patient underwent a right femoral osteotomy, likely to further optimize hip biomechanics, offset abnormalities, or address persistent mechanical symptoms. This sequence of staged surgical interventions illustrates the complexity of managing secondary degeneration in the contralateral limb, where the pathology is not congenital or dysplastic in origin but results from decades of asymmetric stress and altered mechanics. Although such interventions are effective in improving limb symmetry, they rarely eliminate the biomechanical disturbances entirely.
A key turning point in this patient’s course was the overcorrection of LLD following these surgeries. The once-longer right leg is now 3/8 inches shorter than the left. Even a seemingly minor residual discrepancy can perpetuate abnormal loading patterns, pelvic tilt, and compensatory soft tissue strain (5,8,9). Low back pain in patients with LLD is well documented, as with this patient, the persistent pelvic imbalance likely contributes to her low back pain, as studies have shown that LLD, even as small as <1cm, can increase shear forces at the lumbosacral junction and alter paraspinal muscle activity (8,9). These changes can persist even after limb correction if alignment is not adequately restored or if compensatory mechanisms have become habitual.
The patient’s sensitivity to specific footwear highlights the fragility of her current musculoskeletal alignment. Studies have demonstrated that patients with LLD or abnormal gait mechanics are significantly affected by certain shoe designs, as they may subtly alter joint angles or limb kinematics, provoking pain due to maladaptive movement patterns or stress on already compromised joints (10). This symptom points to a significant reliance on compensatory muscle groups and a finely tuned, yet vulnerable, neuromuscular control system. The patient’s need for precise footwear and orthotic adjustments underscores the importance of custom biomechanical interventions in this population.
The extensive involvement on the right side, hip, knee, and ankle, is consistent with a pattern of load transfer that extends distally along the kinetic chain. Chronic hip pathology alters pelvic mechanics, which in turn influences femoral-tibial alignment and subtalar motion. High-repetition loading, especially on a limb with joint dysplasia or malalignment, can accelerate articular cartilage wear and exacerbate underlying biomechanical dysfunction (11).
Conservative care remains the mainstay of management in adult melorheostosis, particularly after surgical correction has been maximized. This patient remains functionally limited despite extensive surgical intervention and uses NSAIDs and activity modification as her primary management strategy. At this stage, non-operative measures should focus on addressing the residual LLD and range of motion with orthotics or custom footwear, gait retraining, and advanced pain management strategies.
While a total hip arthroplasty may eventually be indicated if arthritic progression continues, this decision must be carefully weighed against her age, activity level, and prior surgeries. While recurrence or progression of deformity after osteotomy is uncommon in melorheostosis, the natural history of the disease and underlying skeletal abnormality necessitate periodic reassessment.
This case highlights the complexity of long-term orthopedic management in affected adults with rare bone disorders with asymmetric involvement, where the unaffected limb is at high risk for overuse pathology if mechanical imbalance is left uncorrected. Biomechanical imbalance and compensatory pain can persist , therefore, early recognition and proactive management of LLD and orthopedic complications are essential in optimizing long-term outcomes. In pediatric and adolescent patients with melorheostosis or similar unilateral bone diseases, preventative care may reduce the long-term need for invasive contralateral joint surgery.
References:
- Wynne-Davies R, Gormley J. The prevalence of skeletal dysplasias. An estimate of their minimum frequency and the number of patients requiring orthopaedic care. J Bone Joint Surg Br. 1985 Jan;67(1):133-7. doi: 10.1302/0301-620X.67B1.3155744. PMID: 3155744.
- Deshmukh NS. Melorheostosis (Leri’s Disease): A Review. Cureus. 2024 Jun 8;16(6):e61950. doi: 10.7759/cureus.61950. PMID: 38978887; PMCID: PMC11230603.
- Jha S, Fratzl-Zelman N, Roschger P, Papadakis GZ, Cowen EW, Kang H, Lehky TJ, Alter K, Deng Z, Ivovic A, Flynn L, Reynolds JC, Dasgupta A, Miettinen M, Lange E, Katz J, Klaushofer K, Marini JC, Siegel RM, Bhattacharyya T. Distinct Clinical and Pathological Features of Melorheostosis Associated With Somatic MAP2K1 Mutations. J Bone Miner Res. 2019 Jan;34(1):145-156. doi: 10.1002/jbmr.3577. Epub 2018 Sep 14. PMID: 30138550; PMCID: PMC7577747.
- Fick CN, Fratzl-Zelman N, Roschger P, Klaushofer K, Jha S, Marini JC, Bhattacharyya T. Melorheostosis: A Clinical, Pathologic, and Radiologic Case Series. Am J Surg Pathol. 2019 Nov;43(11):1554-1559. doi: 10.1097/PAS.0000000000001310. PMID: 31386640; PMCID: PMC7832124.
- Gurney B. Leg length discrepancy. Gait Posture. 2002 Apr;15(2):195-206. doi: 10.1016/s0966-6362(01)00148-5. PMID: 11869914.
- Tolk JJ, Merchant R, Eastwood DM, Buddhdev P, Hashemi-Nejad A. The Development of Leg Length Difference and Influence on Persistent Dysplasia in Patients with Developmental Dysplasia of the Hip. Indian J Orthop. 2021 Aug 30;55(6):1568-1575. doi: 10.1007/s43465-021-00492-5. PMID: 35003543; PMCID: PMC8688656.
- Hamawandi SA, Sulaiman II, Abdulhameed AM. Effect of Duration of Symptoms on the Clinical and Functional Outcomes of Lumbar Microdiscectomy: A Randomized Controlled Trial. Orthop Surg. 2022 Jan;14(1):157-168. doi: 10.1111/os.13114. Epub 2021 Dec 5. PMID: 34866340; PMCID: PMC8755886.
- Friberg O. Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality. Spine (Phila Pa 1976). 1983 Sep;8(6):643-51. doi: 10.1097/00007632-198309000-00010. PMID: 6228021.
- Böhm H, Dussa CU. Impact of mild leg length discrepancy on pelvic alignment and gait compensation in children. Gait Posture. 2025 May;118:122-129. doi: 10.1016/j.gaitpost.2025.02.003. Epub 2025 Feb 13. PMID: 39965260.
- Jankaew A, Chen SJ, Lin CC, Tsai CH, Huang MT, Lin CF. Impact of bilateral motion control shoes with outsole adjustment on gait asymmetry in individuals with mild leg length discrepancy. Gait Posture. 2023 Jun;103:80-85. doi: 10.1016/j.gaitpost.2023.04.023. Epub 2023 Apr 28. PMID: 37141834.
- Hayashi D, Englund M, Roemer FW, Niu J, Sharma L, Felson DT, Crema MD, Marra MD, Segal NA, Lewis CE, Nevitt MC, Guermazi A. Knee malalignment is associated with an increased risk for incident and enlarging bone marrow lesions in the more loaded compartments: the MOST study. Osteoarthritis Cartilage. 2012 Nov;20(11):1227-33. doi: 10.1016/j.joca.2012.07.020. Epub 2012 Aug 5. PMID: 22874524; PMCID: PMC3448813.
